
Research
Exercise
March 26, 2026
Rehabilitation for Mild Traumatic Brain Injury: Effectiveness of Physiotherapy Interventions

Introduction
Mild traumatic brain injury occurs because of a direct or indirect impact on the head, leading to problems in brain functioning. Most patients will recover within 14 days, but some will experience long-lasting symptoms negatively impacting their quality of life. Among these impending symptoms, vertigo, dizziness, and balance dysfunction are frequently reported symptoms. Vestibular impairments are recognized as the root cause, as head trauma could have led to axonal damage (such as axonal injury, brain contusions, necrosis), resulting in structural alterations of the inner ear, the vestibulocochlear nerve, the vestibulospinal tract, and the central vestibular tract.
Vestibular rehabilitation therapy (VRT) is a core approach for vestibular symptoms management, and appears as a particularly relevant approach considering mild traumatic brain injury presentation. VRT acts through 3 different mechanisms: adaptation, substitution, and habituation.
While the effect of VRT has been widely investigated, this systematic review provides a recent overview of evidence. Including high-quality research to ground rehabilitation for Mild Traumatic Brain Injury strategies in vestibular symptoms management
Methods
For this systematic literature review with meta-analyses, available literature on RCTs was systematically investigated. Controlled trials and cohort studies were included. Different modalities of VRT were included (home-based, group sessions…).
The primary outcome was the severity of vestibular symptoms, assessed using several validated tools: the Dizziness Handicap Inventory (DHI), Vestibular/Ocular Motor Screening (VOMS), Post-Concussion Symptoms Scale (PCSS), and Balance Error Scoring System (BESS).
The DHI is a 25-item questionnaire evaluating the self-perceived impact of dizziness on physical, emotional, and functional domains, with scores ranging from 0 (no handicap) to 100 (severe handicap).
The VOMS assesses vestibular and ocular motor impairments through symptom provocation during specific tasks, including smooth pursuit, horizontal and vertical saccades, convergence, horizontal vestibulo-ocular reflex (VOR), and visual motion sensitivity (VMS).
The PCSS is a subjective symptom scale in which patients rate the severity of 22 concussion-related symptoms from 0 to 6, resulting in a maximum score of 132.
The BESS evaluates postural stability by counting balance errors during different static stances performed on firm and foam surfaces. Each stance allows up to 10 errors, with a maximum of 30 errors per surface. A modified version (mBESS) assesses balance on a firm surface only.
The secondary outcome was the number of individuals cleared to return to normal function.
Data extraction and risk of bias assessment
Data extracted from full-text articles included study design, participant baseline characteristics, type and frequency of vestibular rehabilitation for Mild Traumatic Brain Injury, follow-up period, and reported outcomes. Data extraction and risk-of-bias assessment were conducted independently by two reviewers using a standardized data collection form.
Risk of bias in randomized controlled trials was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool, while non-randomized clinical trials and cohort studies were evaluated using the ROBINS-I tool.
Statistical analyses
A random-effects model was used to combine the results from different studies. For continuous outcomes, the standardized mean difference (SMD) with a 95% confidence interval (CI) was calculated, while risk ratios (RR) with a 95% CI were used for categorical outcomes. Results were considered statistically significant when the p-value was below 0.05.
Statistical heterogeneity between studies was assessed using the I² statistic and the χ² test, with I² values greater than 50% indicating substantial heterogeneity. When more than two studies were included for an outcome, a sensitivity analysis was performed to examine the influence of study quality on the results.
Separate meta-analyses were conducted for each outcome, and subgroup analyses were performed for the five domains of the VOMS assessment. Because only a small number of studies were available, publication bias could not be evaluated using a funnel plot.
Certainty of evidences
The quality of evidence was assessed through the GRADE criteria, with four possible ratings: high, moderate, low, and very low. The quality of evidence was judged on the basis of the following factors: risk of bias, inconsistency, indirectness, and imprecision.
Results
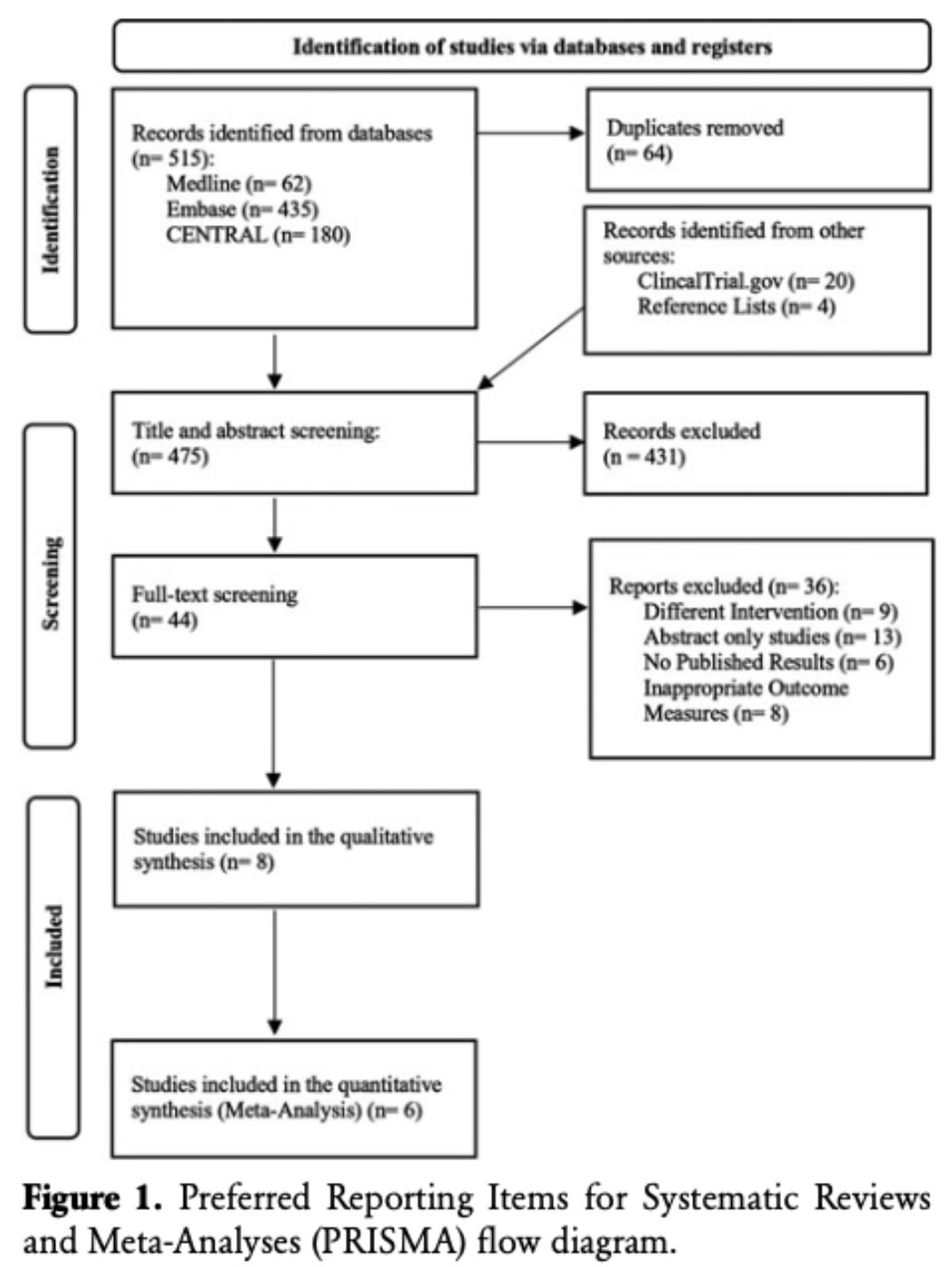
The search initially identified 515 articles, and after removing duplicates, 475 were screened by title and abstract. 44 full-text articles were assessed for eligibility, of which 8 were included in the qualitative synthesis. Of these, 6 studies met criteria for meta-analysis, while 2 cohort studies were excluded to avoid heterogeneity. Non-pooled studies were narratively summarized to support or contrast meta-analysis findings.
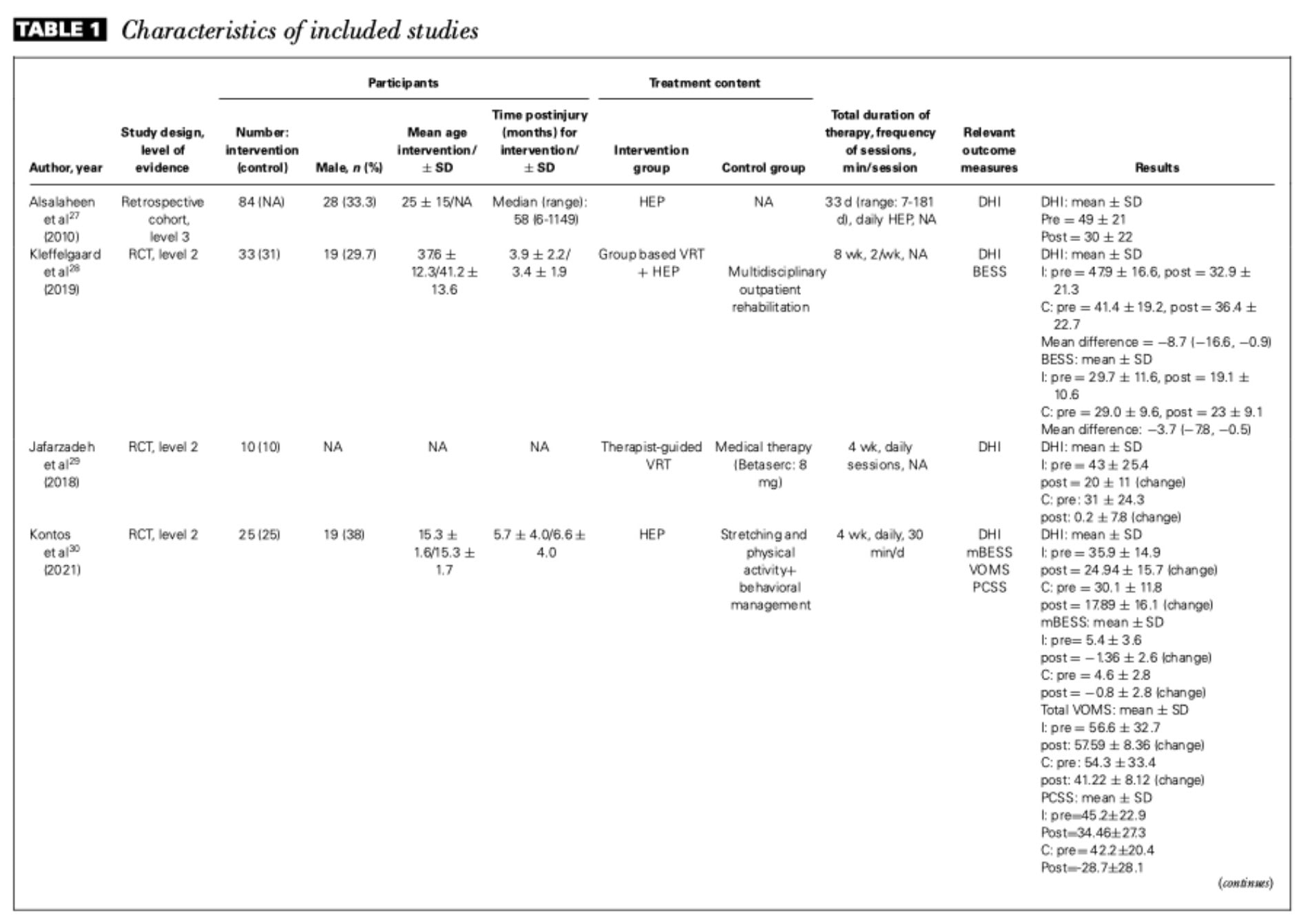
A total of 460 participants were included in the qualitative analysis, while 270 participants were included in the meta-analysis. Among the eight studies included in the qualitative synthesis, three focused on adults, two on adolescents, one on pediatric populations, one on both adolescents and adults, and one included participants across all age groups.
Five studies implemented an individualized rehabilitation approach, combining therapist-guided sessions and home-based exercises. These interventions included canalith repositioning, habituation exercises, gaze stabilization/adaptation, substitution strategies, and balance retraining. In addition, three studies incorporated cervical and thoracic manual therapy, including mobilization, manipulation, and soft tissue techniques.
The duration of interventions ranged from 4 to 8 weeks, and only two studies included follow-up assessments, with monitoring periods ranging from 1 to 6 months after the intervention.
The 6 studies included in the qualitative analyses were considered level 2 evidence due to their RCT design. The cohort studies included were considered level 3 evidence.
Among the 6 included RCTs, 2 studies had a high risk of bias due to lack of allocation concealment, while most studies lacked participant and assessor blinding but were considered low risk for deviations from intended interventions. Only 1 study had a high risk in domain 3 and some concerns in domains 2 and 5. Overall, 2 of 6 RCTs were judged high risk.
For the 2 cohort studies, one had low risk of bias across all domains, while the other showed high risk in outcome measurement, leading to an overall judgment of serious risk.
Outcomes
DHI
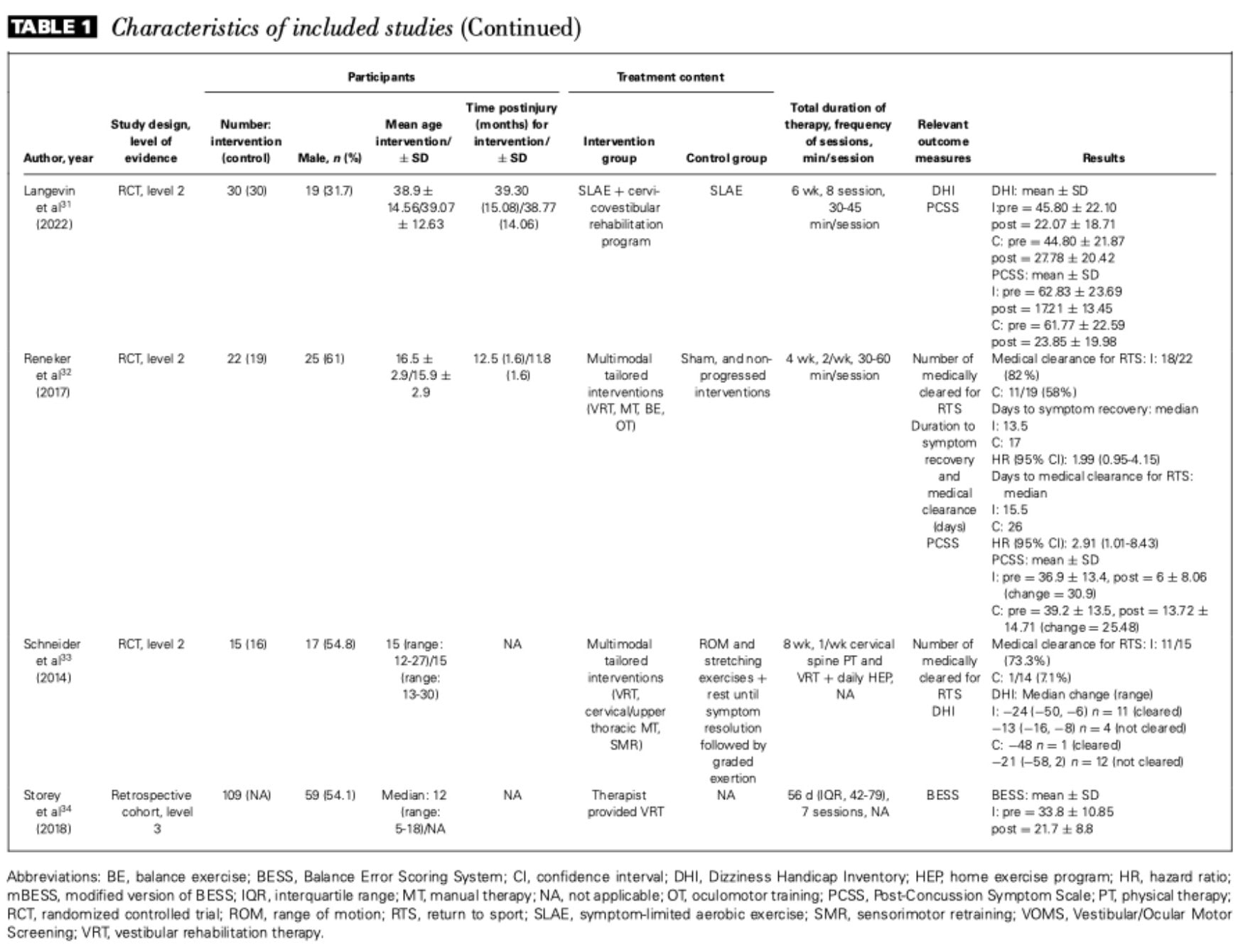
The effect of rehabilitation for Mild Traumatic Brain Injury on Dizziness Handicap Inventory (DHI) scores was evaluated in 5 studies (n = 206). Pooled analysis of 4 studies showed a small but significant improvement at the end of treatment.
At 4 months follow-up, 2 studies (110 participants) resulted in no significant difference between groups.
Studies excluded from the meta-analysis reported significant post-treatment improvements, with greater benefits observed in children compared to adults.
Vestibular/Occular Motor Screening
Two RCTs (n = 81) evaluated the effect of vestibular rehabilitation therapy (VRT) on VOMS scores, showing a significant overall improvement.
Subgroup analysis showed significant improvements in horizontal vestibulo-ocular reflex and visual motion sensitivity, while the other domains did not show significant changes.
Additionally, a study included in the qualitative synthesis reported a reduction in symptom provocation during horizontal and vertical saccades.
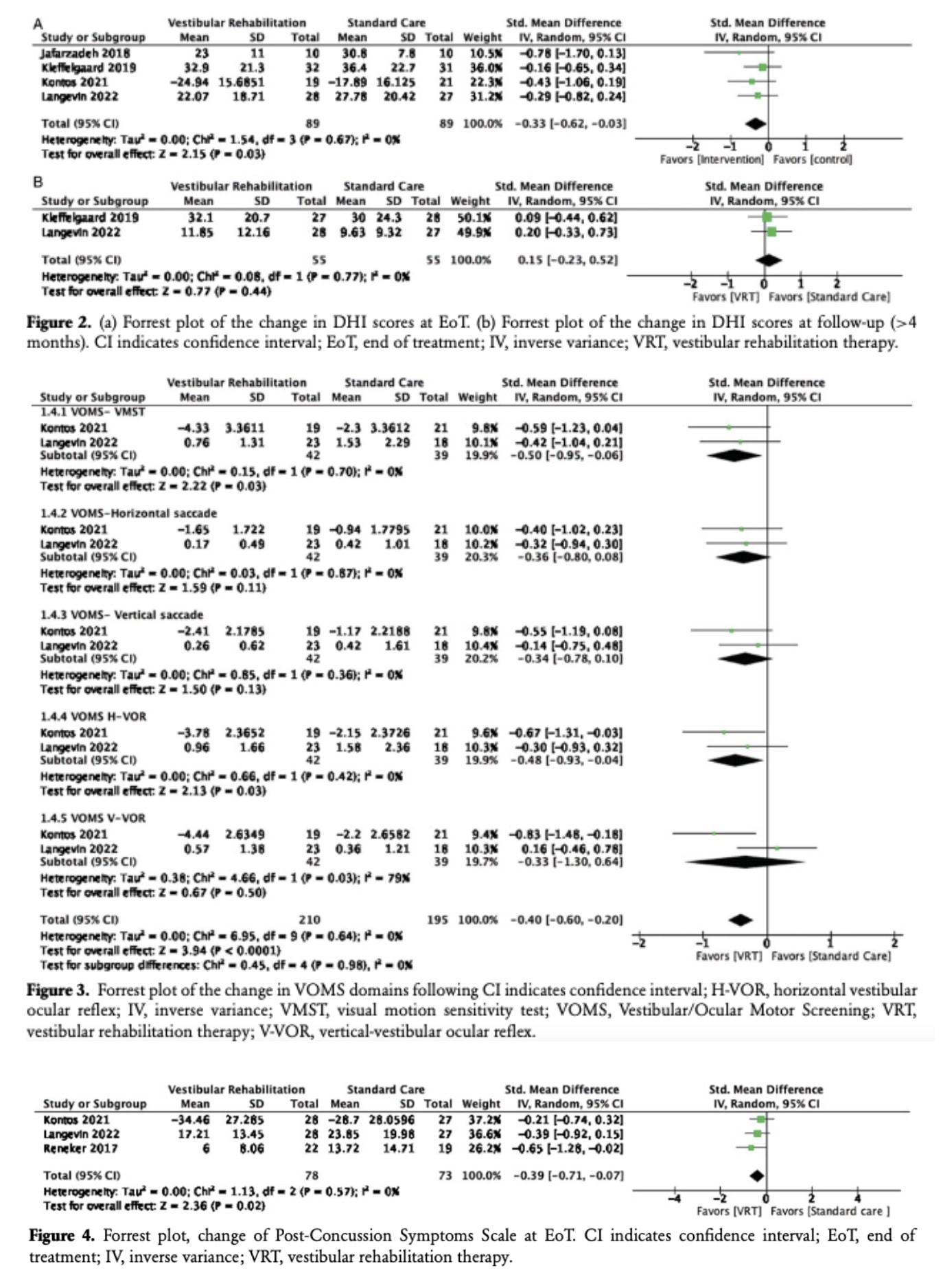
Post-Concussion Symptoms Scale
Four studies (n = 214) assessed post-concussion symptoms, though one study was excluded from the pooled analysis due to a different questionnaire. Pooled results showed a significant improvement in PCSS scores after vestibular rehabilitation therapy
Balance impairment: Balance Error Scoring System.
Two studies, which included 97 participants, evaluated balance using the BESS. Pooled analysis showed a greater decrease in scores for the VRT group, but the effect was not statistically significant.
A separate study reported a significant improvement in balance after VRT.
Return to work/sport analyses
Two RCTs evaluated the effect of individualized multimodal interventions, including VRT, on return to sport/work. Both studies reported that participants in the intervention group recovered faster and were more likely to return to activity. Meta-analysis showed a risk ratio of 3.15 for medical clearance by 8 weeks, with 78.3% of the intervention group cleared versus 37.5% of controls.
Sensitivity assessment
Sensitivity analyses were performed by removing studies with a high risk of bias. For DHI, the effect at the end of treatment became non-significant. For PCSS, the significant improvement remained unchanged.
Questions and thoughts
Because of the varied mechanisms of injury and the wide range of clinical presentations in patients with mild traumatic brain injury (mTBI), symptoms can differ greatly from one individual to another. This variability underscores the importance of a personalized, holistic approach to rehabilitation. In this context, highly rigid research protocols may fail to capture the complexity of patients’ symptoms and may therefore limit the ability to evaluate the true effectiveness of vestibular rehabilitation for Mild Traumatic Brain Injury.
Future research should aim to better account for the multidimensional nature of mTBI symptoms. This includes identifying key symptom drivers, developing standardized assessment tools to capture these dimensions, and improving patient classification. Such approaches could help guide more targeted and individualized rehabilitation interventions.
The absence of a clear effect of VRT on return to sport or normal function may also reflect the limited individualization of treatment protocols used in some studies. Returning to sport or work depends on the specific physical and cognitive demands of each individual’s activities and typically requires a thorough baseline assessment. Standardized protocols used in research may not fully address these highly individualized requirements.
Finally, previous findings suggest that the emotional domain of the Dizziness Handicap Inventory (DHI) tends to improve less than the physical and functional domains following vestibular rehabilitation for Mild Traumatic Brain Injury. This observation may indicate that VRT alone has a limited impact on emotional symptoms, further supporting the need for a more comprehensive, multidisciplinary rehabilitation approach for individuals recovering from mTBI.
Talk nerdy to me
This review included only a small number of studies, and each study had relatively few participants, which introduces important limitations for a meta-analysis.
When studies have small sample sizes, their results are more susceptible to random variation. As a result, one study may report a large treatment effect, while another may find little or no effect, even if the true effect lies somewhere in between. When these small studies are combined in a meta-analysis, the pooled estimates—such as the standardized mean difference (SMD) or risk ratio (RR)—may therefore be biased or overestimated.
Meta-analyses commonly use the I² statistic to measure heterogeneity, or variability between studies. However, when the number of included studies is small, I² may underestimate the true variability between them. This can lead to the incorrect conclusion that the studies are consistent or homogeneous, when in fact they may differ substantially in terms of results, methodology, or participant characteristics.
Additionally, there were differences in how outcomes were reported across studies. Some studies reported changes from baseline, while others presented final mean values after the intervention. These inconsistencies in reporting contributed to differences in the interpretation and comparison of results.
Take-home messages
Vestibular rehabilitation is a valuable intervention after mild TBI
Vestibular rehabilitation for Mild Traumatic Brain Injury appears to reduce dizziness and post-concussion symptoms, with improvements observed in outcomes such as the DHI, VOMS, and PCSS.
Targeting the vestibular system can improve specific impairments
VRT seems particularly effective for vestibulo-ocular deficits, including horizontal vestibulo-ocular reflex (VOR) and visual motion sensitivity. These findings highlight the importance of gaze stabilization, habituation, and adaptation exercises in rehabilitation for Mild Traumatic Brain Injury programs.
Improvements in balance are less clear
Results suggest that balance recovery after mTBI may depend on multiple systems (vestibular, cervical, visual, and sensorimotor) and may require broader rehabilitation strategies.
Multimodal rehabilitation may help patients return to activity sooner
Programs combining VRT with other interventions (such as cervical manual therapy or individualized exercise) may help patients recover faster and return to sport or work earlier, although current evidence remains limited and uncertain.
Rehabilitation should be individualized
Symptoms after mild TBI vary widely depending on the mechanism of injury, affected systems, and patient characteristics. Physiotherapists should prioritize personalized rehabilitation programs that integrate vestibular, cervical, and functional rehabilitation based on individual assessment findings.
Address the patient beyond vestibular symptoms
Vestibular rehabilitation tends to improve physical and functional symptoms, but emotional aspects (such as anxiety or fear related to dizziness) may improve less. This highlights the importance of a holistic, multidisciplinary approach that may involve psychological or cognitive support.
Interested in learning more about vestibular rehabilitation? Listen to this Physiotutors podcast episode.
Reference
Learn to Treat the Most Common Cause of Vertigo in This FREE Mini-Video-Series
Leading Vestibular Rehabilitation Expert Firat Kesgin takes you on a 3-Day Video Course on how to recognize, assess and treat posterior canal Benign-Paroxysmal Positional Vertigo (BPPV)
