
Research
Exercise
March 24, 2026
Adherence to Strengthening Exercise Guidelines

Introduction
We know that, in general, adherence to the World Health Organization (WHO) physical activity guidelines is low. The recommendation is that adults do at least 150–300 minutes of moderate-intensity aerobic physical activity, at least 75–150 minutes of vigorous-intensity aerobic physical activity, or an equivalent combination of moderate- and vigorous-intensity activity throughout the week, for substantial health benefits. Next to aerobic physical activity, adults should also do muscle-strengthening activities at moderate or greater intensity that involve all major muscle groups on 2 or more days a week, as these provide additional health benefits. Both received a strong recommendation, supported by moderate certainty evidence.
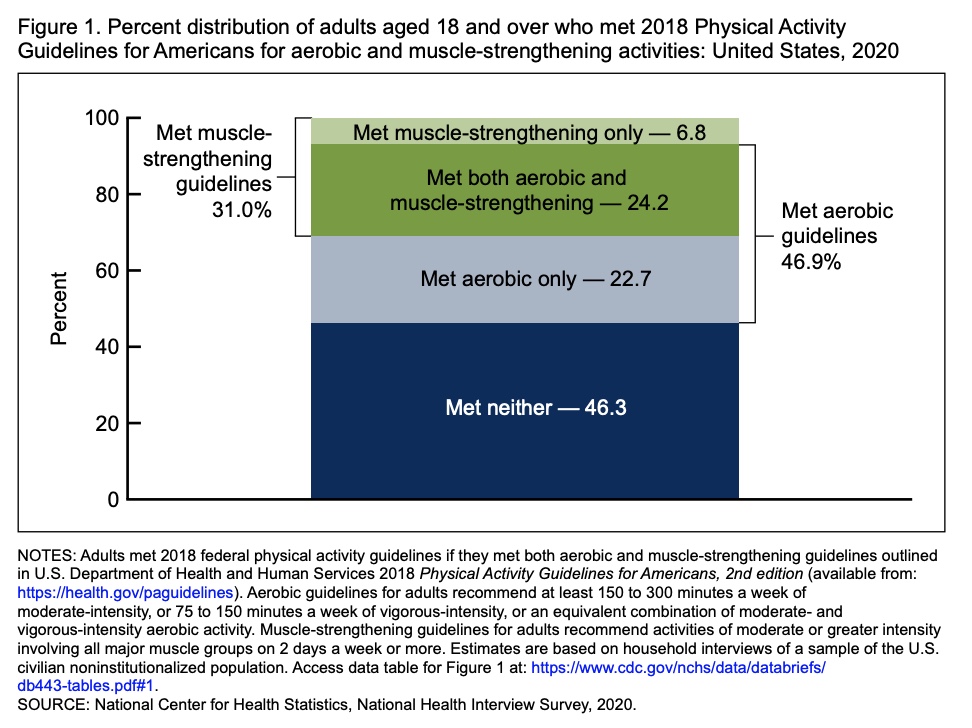
A recent report conducted in the United States concluded that, for example, only 24.2% of adults meet both aerobic and muscle-strengthening guidelines, with nearly half of adults meeting neither recommendation. Around 47% met the aerobic physical activity guidelines, while only 31% met the strengthening guidelines.
As we know, from an earlier research review, that non-adherence to the WHO guidelines leads to a 5% increase in cancer risk, and a combined non-adherence to waist circumference and physical activity guidelines increases the risk of developing cancer by 15%, the need for understanding why adults fail to meet the recommendations is of high importance. The current study summarizes the global prevalence and investigates who meets the recommendations and why.
Methods
This was a systematic review and meta-analysis conducted according to PRISMA guidelines and registered prospectively. This systematic review and meta-analysis had two primary aims: (1) to estimate the global prevalence of adults adhering to the muscle-strengthening exercise guidelines (at least two times/days per week) and (2) to synthesize the evidence on the correlates of adherence to these guidelines
Five electronic databases were searched from their inception up to March 2022. Studies included healthy adults (mean age 18 or above), and had to be observational in their study design.
Regarding the first aim, the prevalence of adherence to the muscle-strengthening exercise guidelines was reported. The second aim looked for factors of adherence to the muscle-strengthening exercise guidelines. Studies with unhealthy participants (e.g., diagnosed physical or mental health problems), intervention studies, systematic reviews/meta-analyses, case studies, and studies not published in English were excluded.
Results
The systematic review and meta-analysis included a total of 30 observational studies, with 2,629,508 participants. Of these, 21 studies were used for the meta-analysis (Aim 1) and 12 for the systematic review of correlates (Aim 2).
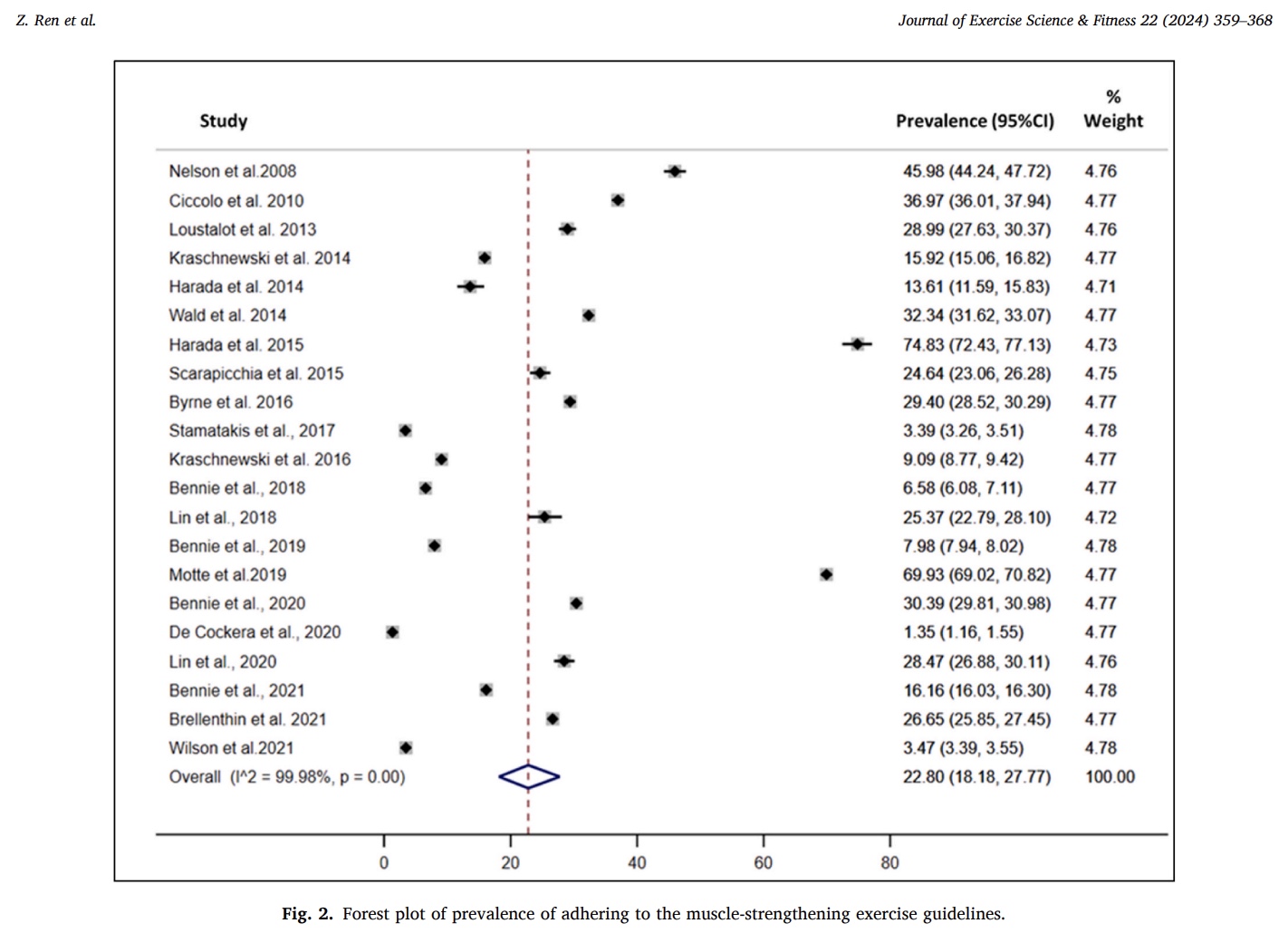
Across 21 studies included in the meta-analysis for aim 1 (n = 2,412,407 participants), the pooled prevalence of adults meeting muscle-strengthening exercise guidelines (≥2 sessions per week) was 22.8% (95% CI: 18.18–27.77). Individual study estimates varied widely, ranging from 1.3% to 76.2%, indicating substantial variability across populations.
Subgroup analysis revealed that the method of muscle-strengthening exercise measurement significantly influenced prevalence. Studies using weekly recall reported higher adherence (29.53%) compared to those using monthly recall (11.43%). No significant differences were found across regions, study quality, or publication periods.
Regarding the second aim, twelve studies (n = 501,847 participants) were included in the analysis of correlates, identifying 23 potential factors across five domains: sociodemographic, physical, behavioural, cognitive, and environmental.
Consistent correlates (moderate-to-strong evidence)
Eight factors were consistently associated with adherence to strengthening exercise guidelines:
- Male sex
- Younger age
- Higher education level
- Higher socioeconomic status
- Better self-rated health
- Healthier body mass index
- Geographical region
- Employment status
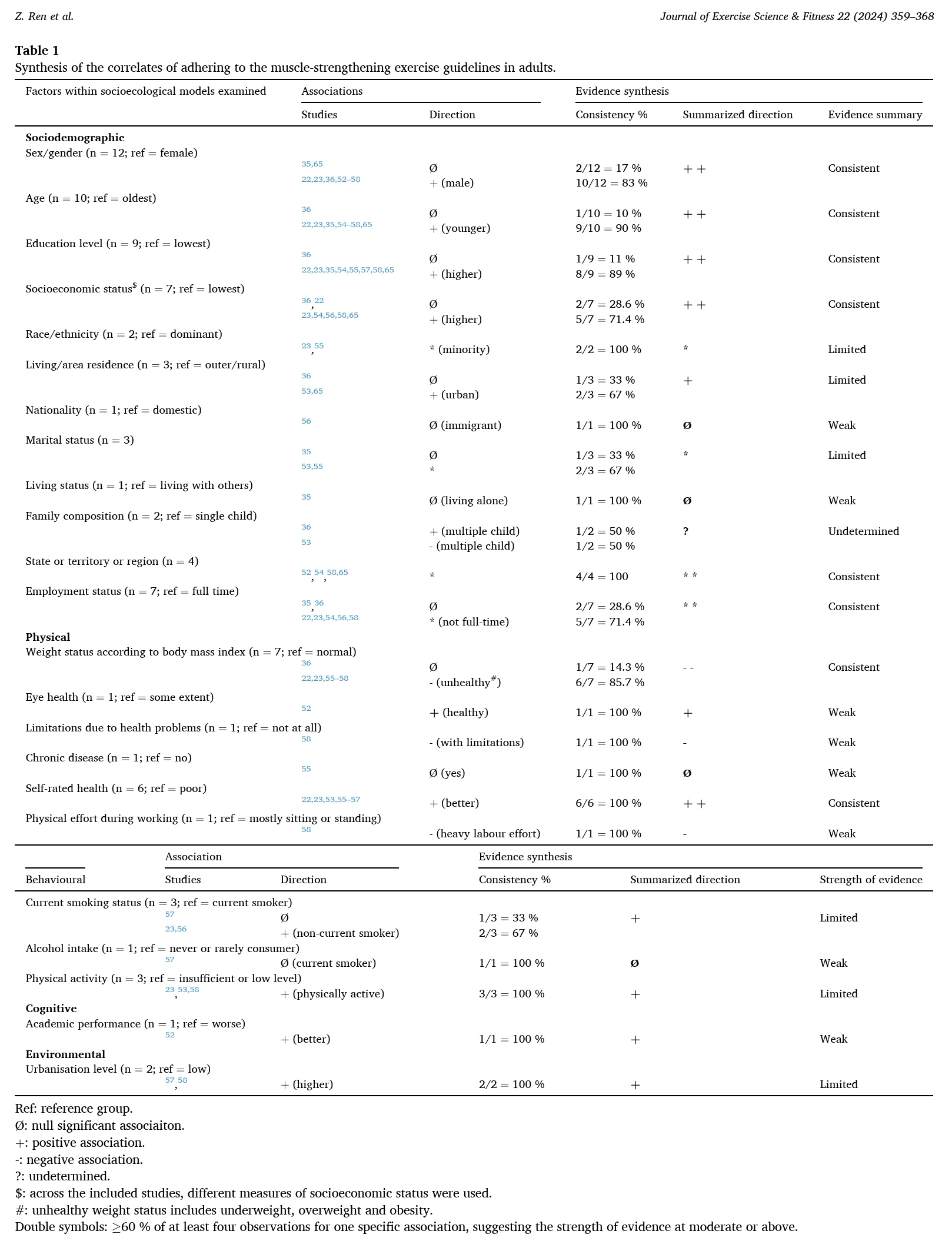
Adults who were male, younger, more educated, and of higher socioeconomic status were more likely to meet muscle-strengthening exercise guidelines. Conversely, individuals with overweight or obesity were less likely to adhere.
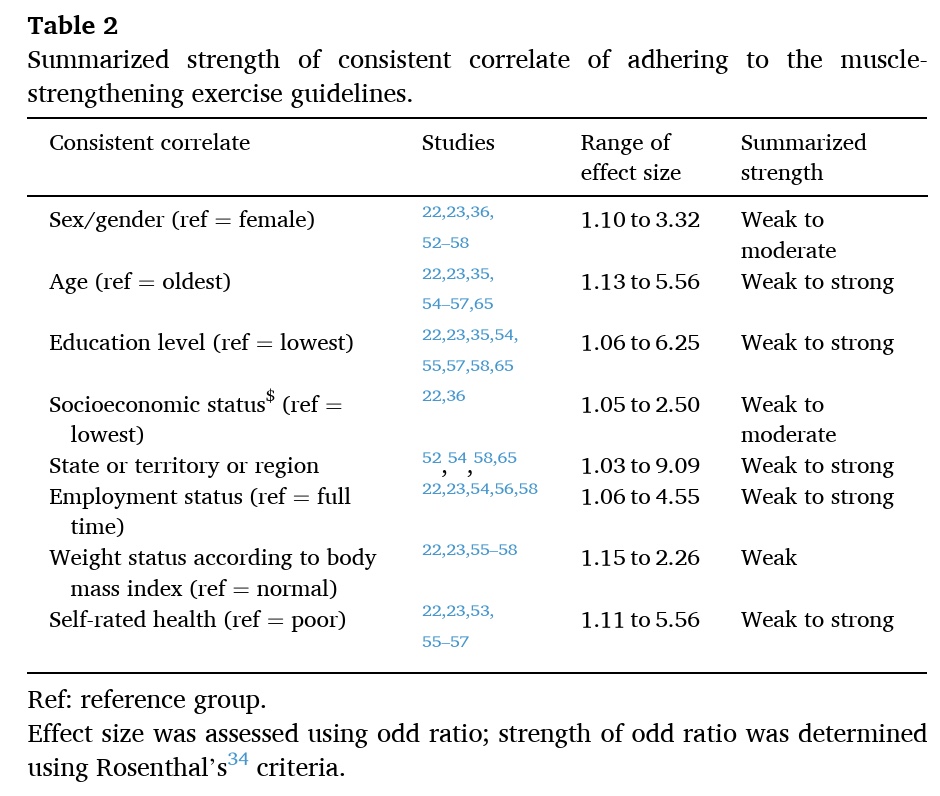
Strength of associations
Across consistent correlates, effect sizes were generally weak to moderate, with only occasional weak to strong associations reported
Limited correlates (inconclusive or weak evidence)
Several factors showed limited or inconsistent associations:
- Living in urban areas (positive association)
- Non-smoking status (positive association)
- Meeting aerobic physical activity guidelines (positive association)
- Race/ethnicity, marital status, and living arrangements (uncertain direction)
Single-study correlates (weak evidence)
Factors such as alcohol intake, academic performance, chronic disease, and occupational physical effort were each examined in only one study, preventing firm conclusions.
Questions and thoughts
The strongest consistent correlates identified by this systematic review are socio-demographic factors (sex, age, education, socioeconomic status). While these can help identify “vulnerable populations” (e.g., older adults, women, lower education/SES), we can not change these factors with our physiotherapy interventions.
On the other hand, other physical factors, such as body mass index (BMI) is something that we can address, or at least discuss. The benefit is twofold: engaging in muscle-strengthening exercise will help control someone’s BMI, and as the BMI improves, the odds of adherence to strengthening exercise guidelines can become better. The same holds for the self-rated health; getting someone to start with strengthening exercises can improve general health and maybe also their sense of wellbeing. Meeting aerobic physical activity guidelines showed a positive association, although supported by limited evidence. As such, promoting a combined approach to physical activity and strengthening exercise rather than separating the two seems best, as engagement in one may facilitate engagement in the other.
As adults who are overweight or obese are less likely to adhere to strengthening exercise guidelines, this highlights a key target group. Further research on specific barriers to engagement or adherence to strengthening exercise guidelines (e.g., perceived effort, joint pain, lack of confidence) can help us overcome common difficulties.
All included studies used self-reported measures of muscle-strengthening exercise adherence, and there were large variations in how it was defined. A significant finding was that prevalence was higher when measured by weekly recall (29.53%) compared to monthly recall (11.43%), suggesting that the measurement period itself significantly influences the reported adherence rate, possibly due to memory bias. This variation is a major factor influencing the accuracy and consistency of responses. In practice, using weekly reporting of adherence therefore seems best.
Talk nerdy to me
The I² statistic showed that heterogeneity was extremely high (I² = 99.98%), suggesting considerable differences in study populations, measurement methods, and contexts. This implies that the 22.8% prevalence estimate may not be globally representative, contrary to the aim of this study.
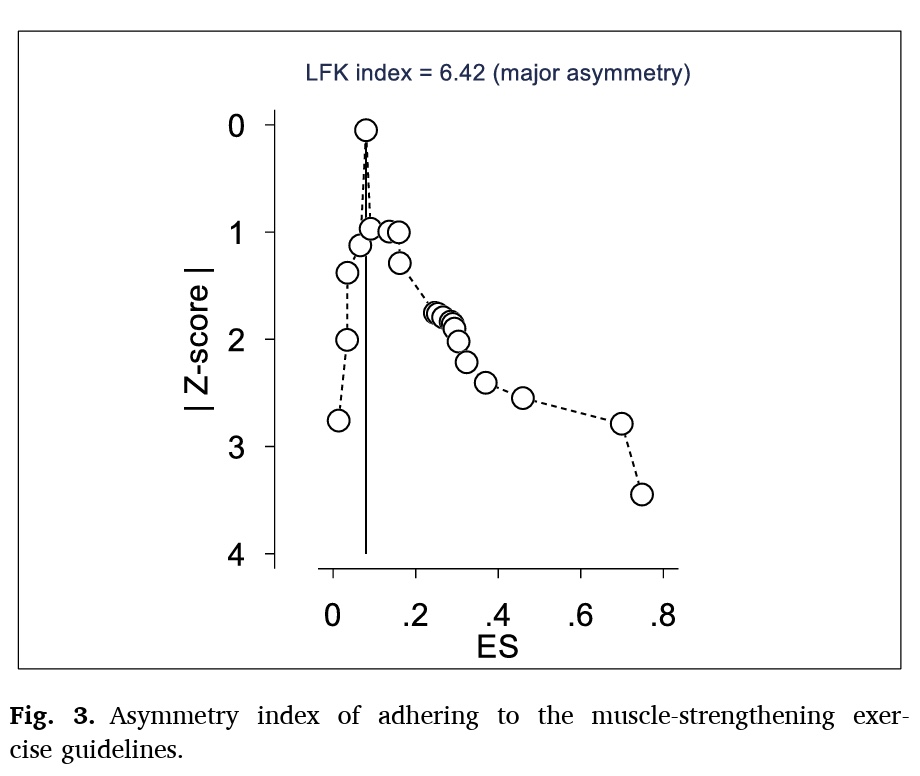
Publication bias was also identified, with a large asymmetry in the Doi plot (LFK index = 6.42), indicating potential distortion of pooled estimates. The major risk of publication bias can mean that studies reporting higher prevalence rates or stronger associations are more likely to be published, potentially inflating the pooled estimate and the reported strengths of correlates.
Additionally, correlates were synthesised narratively due to heterogeneity, meaning that the factors couldn’t be summarized into pooled effect sizes. Therefore, this is merely a qualitative synthesis rather than a quantitative pooling.
Finally, nearly all included studies were cross-sectional, so we must be aware that associations do not imply causation. Also, reverse causality is likely, for example, does better health lead to adherence to strengthening exercise guidelines, or vice versa?
Take-home messages
Less than a quarter of adults globally—only 22.8%—are meeting the recommended guidelines for muscle-strengthening exercise (MSE), which is set at least two times per week. This low rate has significant public health implications.
The adults most likely to be adhering to strengthening exercise guidelines are:
- Men
- Younger adults
- Those with higher education and better socioeconomic status
- Those who report better self-rated health and have a normal body mass index
Key take-home messages
- Target Vulnerable Populations: Identify older patients, female patients, and those with lower socioeconomic status or lower self-rated health as being at the highest risk of non-adherence to your strengthening prescriptions. These groups warrant extra focus on developing skills and confidence for muscle-strengthening exercise.
- Muscle-strengthening exercise and aerobic activity are linked: Individuals who adhere to aerobic physical activity guidelines are also more likely to adhere to muscle-strengthening exercise guidelines. Promote a combined approach to physical activity rather than separating the two, as engagement in one may facilitate engagement in the other.
- Measurement Matters: When asking patients about their exercise habits, be aware that asking for recall over a longer period (e.g., a month) may significantly underestimate their adherence compared to asking about the past week, likely due to memory bias. Use a weekly recall for the most accurate picture of your patient’s engagement
The most threatening limitation to the overall conclusions and validity of this study is the major risk of publication bias and the extremely high heterogeneity in the data used to calculate the 22.8% prevalence. This suggests that the reported global figure may be an overestimation due to selection bias in the published literature, or simply not generalizable due to vast differences between the included studies.
Reference
How Nutrition Can Be a Crucial Factor for Central Sensitisation - Video Lecture
Watch this FREE video lecture on Nutrition & Central Sensitisation by Europe’s #1 chronic pain researcher Jo Nijs. Which food patients should avoid will probably surprise you!
