
Research
Exercise
November 17, 2025
Prevention program for Hamstring injuries, insights from a cohort study on professional football players.

Introduction
Hamstring muscle injuries (HMIs) are still the most common injuries in professional football despite the widespread use of eccentric knee flexor strengthening programs. This persistence suggests that current prevention strategies, mainly focused on eccentric hamstring strength, may be too narrow and lack adherence.
Recent research by Lahti et al. proposed a broader, multifactorial program addressing various modifiable intrinsic risk factors—such as posterior-chain strength, lumbopelvic control, flexibility, triceps surae health, and sprint performance. Integrating sprint-focused training could further enhance both performance and injury prevention, fostering collaboration between medical and performance staff.
Since players’ individual risk profiles change throughout the season and only one prior study has applied such a multifactorial, individualized approach in a single club, there is a need for more accessible, scalable methods across different teams. Therefore, the present study aims to evaluate whether a multifactorial and individualized musculoskeletal program can reduce HMI occurrence in professional football teams already implementing injury prevention strategies.
Method
Study design and overall procedure
This prospective cohort study followed professional football teams over two seasons. The 2019 season served as the control period, while the 2021 season implemented a multifactorial prevention program for hamstring injuries. Data on sport exposure and injuries were collected consistently across both seasons. The intervention, initially scheduled for 2020, was delayed to 2021 due to the COVID-19 pandemic. Both seasons ran from April to October.
Participants
Participants were recruited from teams in the Finnish Premier Football League. Strength and conditioning coaches and physiotherapists were contacted individually to facilitate recruitment. Eligible participants included players who took part in training sessions during the 2019 or 2021 seasons and consented to the use of their medical data. Goalkeepers were excluded due to their lower risk of hamstring injury.
Primary outcomes and data collection
The study’s primary outcome was the occurrence of an index hamstring muscle injury (HMI). An HMI was defined as a traumatic or overuse injury to the posterior thigh muscles sustained during sport exposure, resulting in missed training sessions or matches. Diagnoses were made through player interviews and clinical examinations by medical staff, and confirmed using ultrasound or MRI.
Other data collection
Additional data collected included players’ baseline characteristics (such as anthropometrics, team, playing position, and hamstring injury history from the previous two seasons), as well as within-season sport exposure data (training and match hours). Screening tests and questionnaires on HMI risk factors and the perceived most effective training methods for injury reduction were completed by the coaching staff.
Intervention
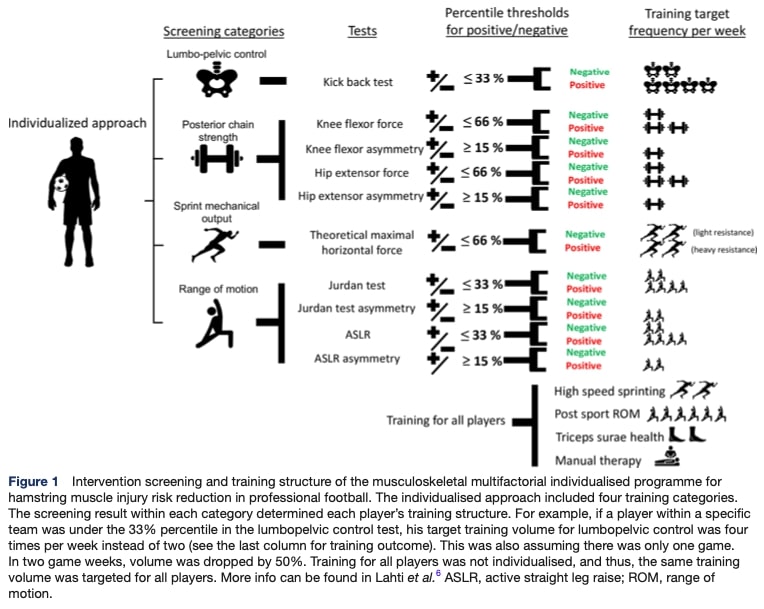
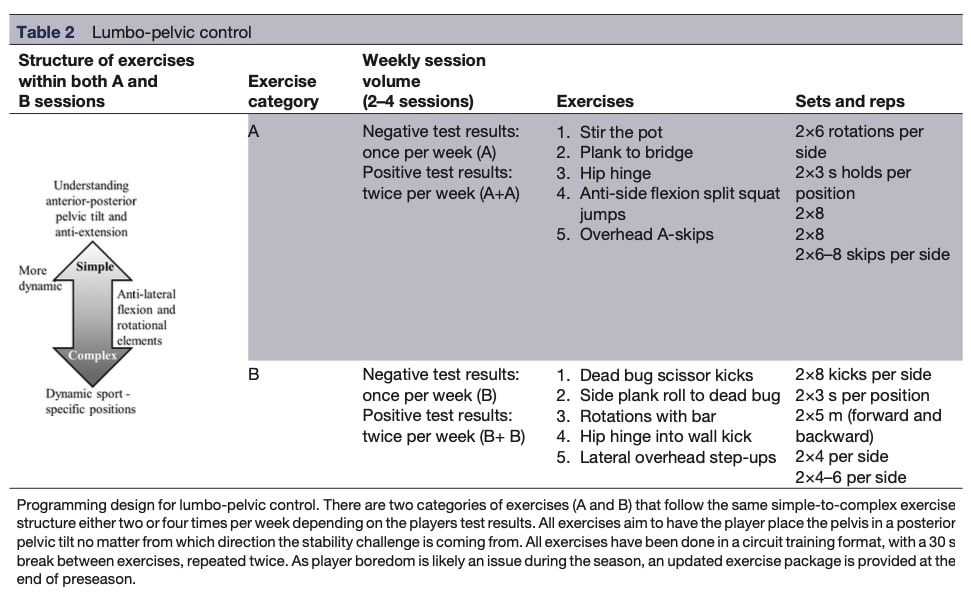
The intervention, implemented only during the 2021 season, consisted of a musculoskeletal multifactorial prevention program for hamstring injuries. Each player underwent a battery of screening tests at four time points in the season (start and end of preseason, midseason, and end of season) to personalize their training program. The screening targeted four key areas: lumbopelvic control, range of motion (ROM), posterior chain strength, and sprint mechanical output.
- Lumbopelvic control was assessed using two tests:
- A “walk test” employing a WIVA digital gyroscope to measure 3D pelvic kinematics during a 10 m walking task, providing a composite score for sagittal and frontal plane control.
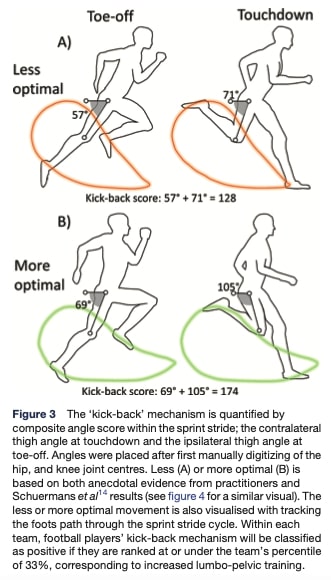
- A sprint kinematics assessment during a 30 m maximal sprint, analyzed via high-speed video (240 fps) to evaluate sagittal plane pelvic mechanics and lower-limb angles at touchdown and toe-off—indicators of sprint technique quality.
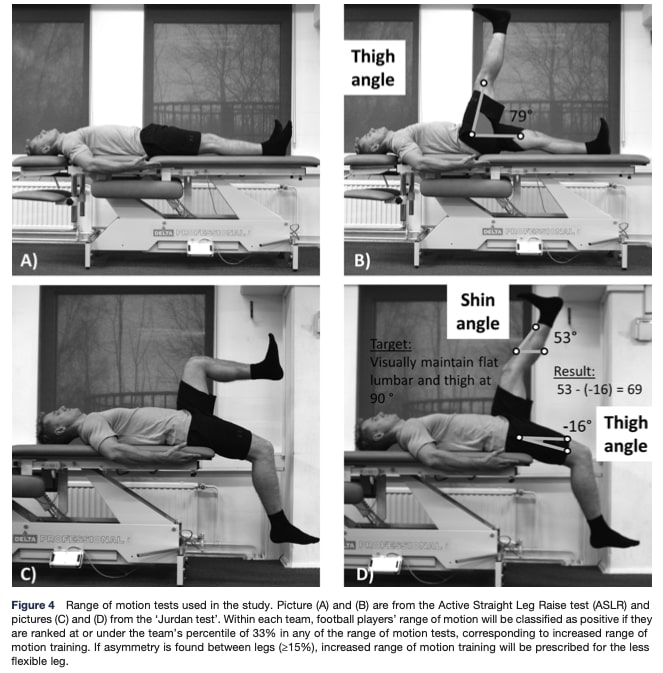
- Range of motion (ROM) was evaluated with two tests:
- The Active Straight Leg Raise (ASLR) test measuring active hamstring flexibility in supine position.
- The Jurdan test, a newly proposed measure examining the interaction between hip flexor and hamstring flexibility by combining elements of the modified Thomas and active knee extension tests, emphasizing inter-limb
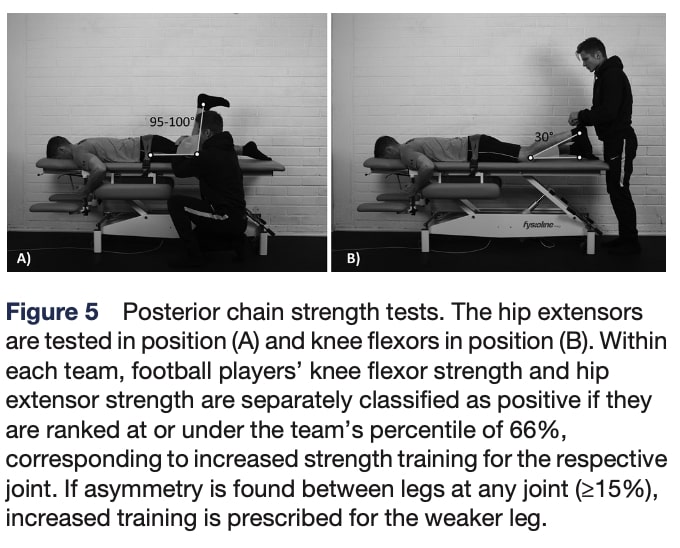
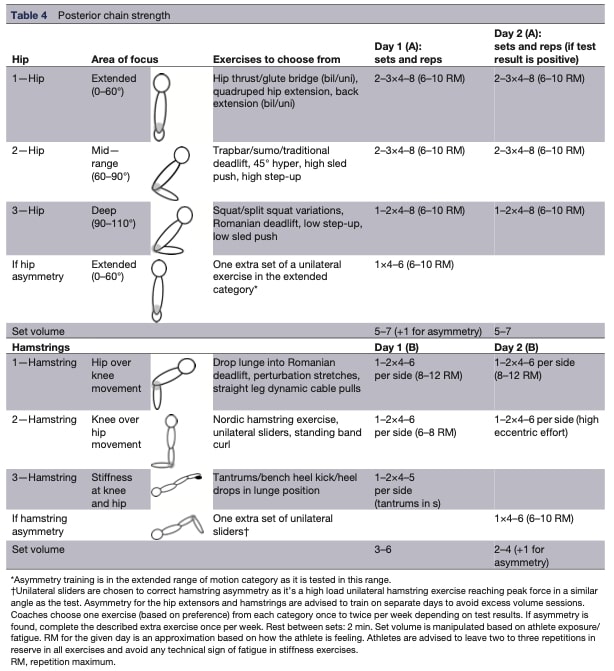
- Posterior chain strength was measured using handheld dynamometry in prone position to assess isometric strength of the hip extensors and knee flexors at standardized joint angles.
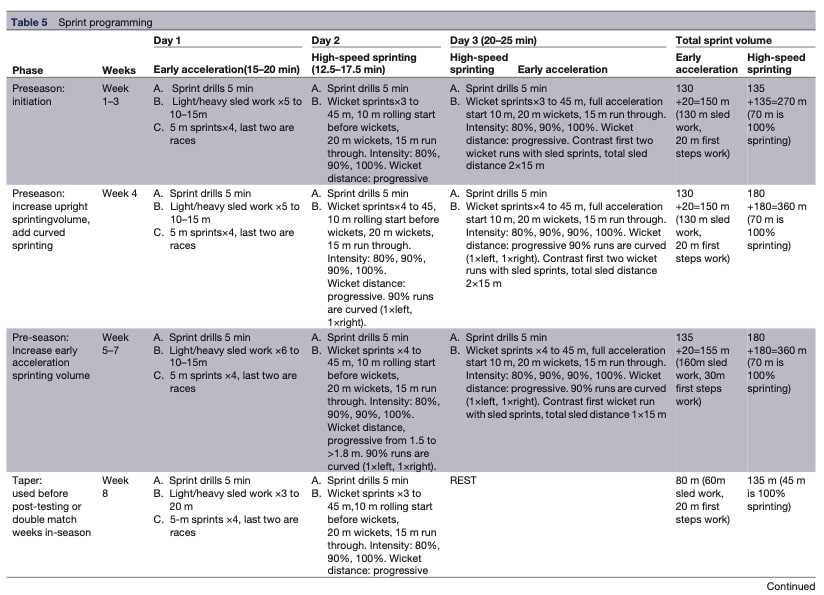
- Sprint mechanical output was assessed via two 30 m maximal sprints, using a radar device to compute sprint times, maximal velocity, and horizontal force output (F₀) through validated inverse dynamics analysis.
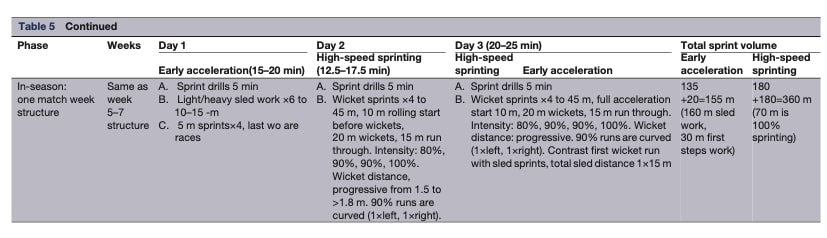
All players trained in each of the four categories, but individual training volumes were adjusted according to percentile rankings within their teams—those performing above the reference threshold followed a maintenance-focused plan. The non-individualized components of the intervention included high-speed sprinting, post-sport ROM work, triceps surae health exercises, and manual therapy.
More details on exercise types, modalities and parameters are provided in the Annex section.
Programming guidelines were provided to fit team schedules, acknowledging variations due to different resources and workloads. Interestingly, not all teams were using a GPS tracking system, further fostering the implementation of a non-individualized group. Team physiotherapists and strength and conditioning coaches were responsible for implementing the program, supported by instructional videos and a weekend workshop. The study authors anticipated considerable variability in how each team would implement the intervention’s weekly programming. The coaching staff recorded weekly compliance data for each player.
Sample Size calculation and statistical analyses
The sample size was determined based on an expected HMI prevalence of 22%, aiming for a 66% reduction in HMI occurrence, with 80% statistical power and a 5% significance level. This calculation resulted in a target recruitment of 93 players per group.
Descriptive statistics summarized player characteristics, screening test results, sport exposure, and injury data, using means and standard deviations for continuous variables and frequencies with percentages for categorical data. Compliance with the intervention was calculated for each player and training category as the percentage of completed versus targeted sessions, then averaged across categories to obtain overall compliance.
To evaluate the effectiveness of the multifactorial and individualized intervention in reducing HMI risk, a Cox proportional hazards regression was performed, comparing the control (2019) and intervention (2021) seasons. The model included time to the first new HMI as the outcome and was adjusted for age, team, body mass, height, and previous HMI history, using cumulative football exposure hours (training + competition) as the time variable. Hazard ratios (HR) with 95% confidence intervals were reported, and the proportional hazards assumption was verified.
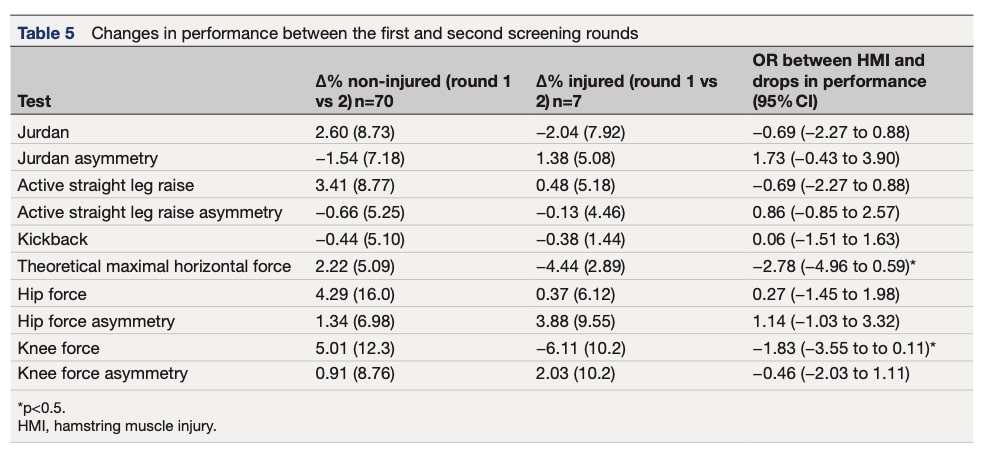
A secondary case-crossover analysis included only players who participated in both seasons, enabling within-player comparisons and controlling for individual differences. Additional analyses compared HMI prevalence (how many players were injured), incidence (injuries per exposure hour), and burden (days lost per 1000 hours) between seasons using relative risk (RR) and explored associations between declines in screening performance (% change) and subsequent HMI occurrence using odds ratios (OR).
Deviation from the protocol
The intervention season, initially planned for 2020, was delayed to 2021 due to COVID-19, resulting in three instead of four measurement rounds. Software issues also led to the removal of the walk test, leaving only the kickback test for assessing lumbopelvic control. Player characteristics between seasons were compared using t-tests and χ² tests. Additional analyses included a case-crossover design, relative risk calculations for HMI outcomes, and correlations between compliance, screening performance changes, and injury risk.
Results
Population
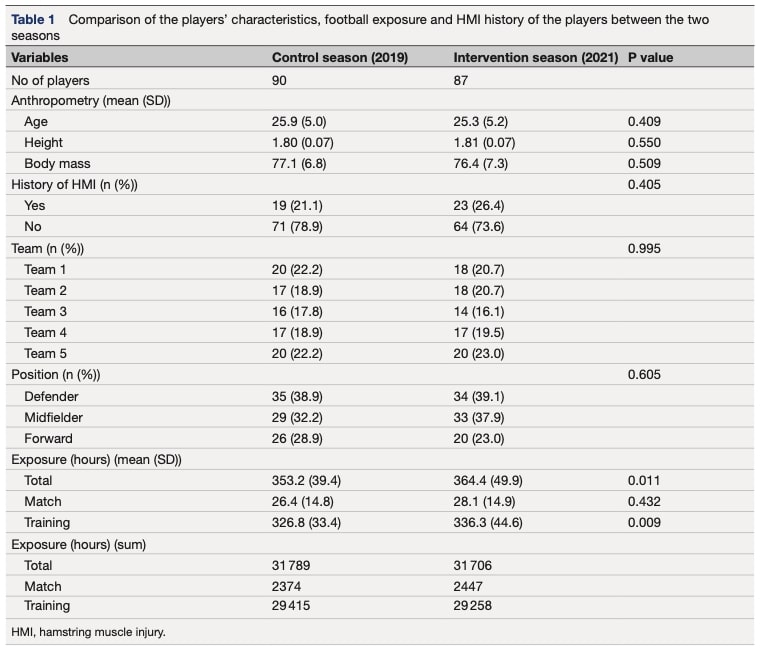
The final sample studied included 90 players from 5 different professional football teams for the control season 2019 and 85 players for the 2021 intervention season. 31 players participated in both seasons. The players’ characteristics are further described in Table 1.
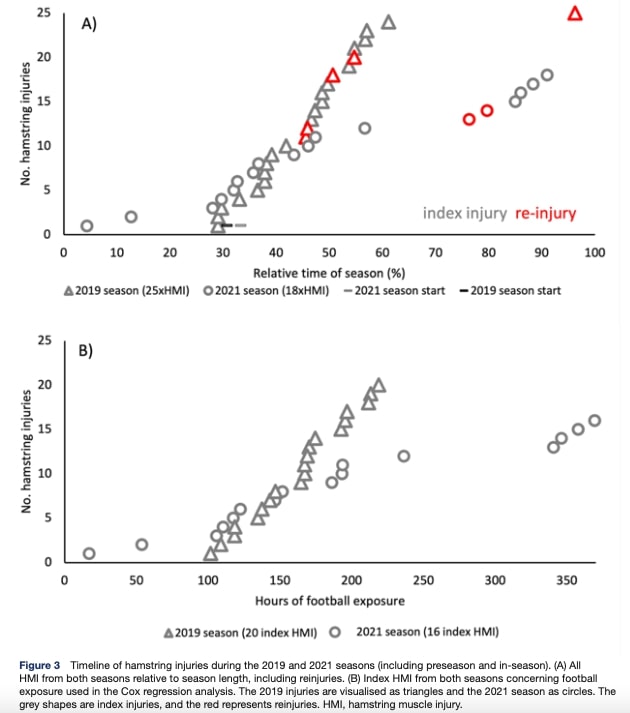
Hamstring Muscle Injuries
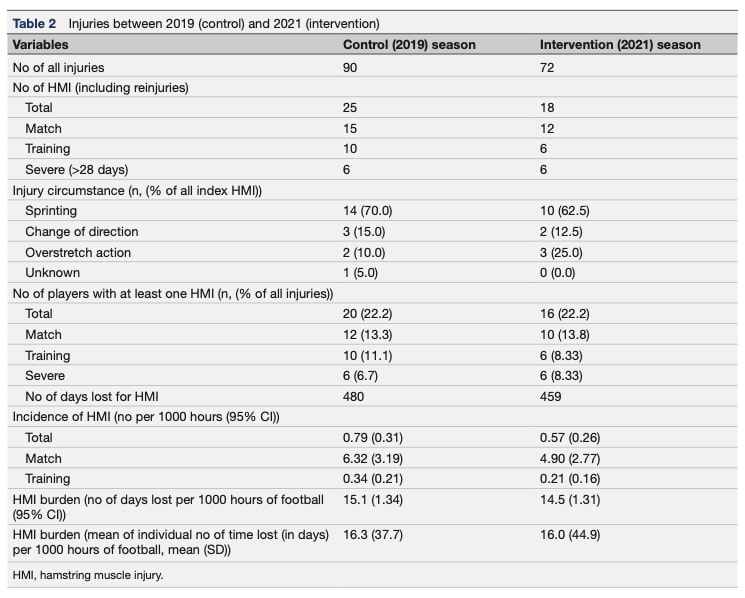
During the 2019 (control) and 2021 (intervention) seasons, 25 (27.8%) and 18 (25.0%) hamstring muscle injuries (HMIs) were recorded, affecting 20 and 16 players and resulting in 480 and 459 days lost, respectively. Overall, no significant differences were found between seasons in HMI prevalence, incidence, or burden.
Among the 31 players who participated in both the 2019 and 2021 seasons, nine hamstring muscle injuries occurred in each season, affecting seven players in 2019 and five in 2021. These injuries resulted in 173 and 114 days lost from sport, respectively. Although no significant differences were observed between seasons for HMI prevalence or incidence, the injury burden was significantly reduced from the 2019 to the 2021 season, decreasing from 15.6 to 10.5 days lost per 1,000 hours of football.
Secondary Risk Analyses and Compliance
The primary Cox proportional hazards regression, adjusted for age, team, body mass, height, and injury history, showed no significant difference in HMI risk between the control (2019) and intervention (2021) seasons. Similarly, the secondary analysis, including only players who participated in both seasons, found no significant difference in HMI risk.
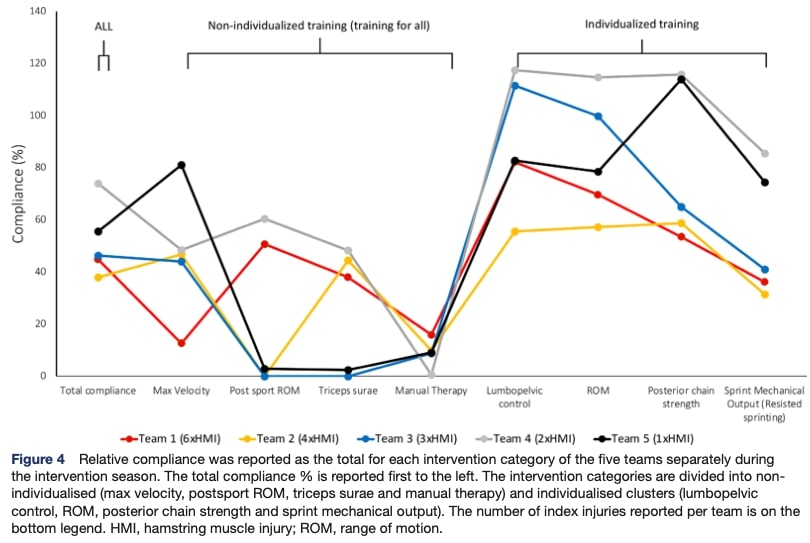
Average compliance with the prevention program for hamstring injuries varied across categories throughout the season. Significant negative correlations were observed between HMI incidence and compliance in knee strength training and maximal velocity exposure, suggesting that greater adherence in these areas was associated with a lower injury rate.
Screening Results
During the 2021 intervention season, 87 players completed the first screening, 77 the second, and 48 all three. Ten players missed the second screening due to injury, while the reduced participation in the third round was mainly due to injuries (n=12) or transfers to other teams (n=33).
Analysis of performance changes between screening rounds revealed that players showing declines in maximal theoretical horizontal force and knee flexor strength had a significantly higher risk of subsequent hamstring injury, with odds ratios of 2.78 and 1.83, respectively (p < 0.05).
Questionnaires Results
Questionnaire data from the 2019 and 2021 seasons revealed differences in training practices and perceived benefits. In 2019, sprint training—including drills, runs, and resisted sprints—was the least implemented category across the five teams. In 2021, teams with lower HMI incidence reported that increased sprint training was the most beneficial component of the intervention.
Questions and Thoughts
While this study did not demonstrate that an individualized prevention program for hamstring injuries significantly reduced HMI risk at any time point, it did show a meaningful reduction in HMI burden at the team level. The results further indicated that higher compliance with knee-strength training and maximal-velocity exposure was correlated with lower HMI incidence. In contrast, greater declines in maximal theoretical horizontal force and knee flexor strength were associated with an increased risk of HMI. One might have expected stronger effects, and the modest findings may be partly explained by methodological limitations and the intrinsic challenges of studying injury prevention. A first limitation is that the intervention season—initially scheduled for 2020—was postponed to 2021 due to the COVID-19 pandemic. The atypical training constraints and reductions in load during quarantine likely altered players’ physical preparedness and may have increased musculoskeletal injury risk during the intervention year. Another important limitation is the high number of players lost to follow-up in the screening rounds.
The reliability of intervention delivery is also questionable. The coaching staff’s knowledge of HMI risk was assessed only through questionnaires, and although a single researcher conducted all screening tests, the individualized prevention program for hamstring injuries implementation varied substantially between teams. Notably, one team experienced a 413% increase in injury burden and a rise in injury incidence between 2019 and 2021, highlighting potential issues with that team’s planning and periodization strategy. In addition, established preventive modalities—such as Nordic hamstring exercises—were not systematically integrated. Sprint exposure, which follows a U-shaped relationship with injury incidence, was also insufficiently controlled. The program compliance data further demonstrates the insufficient implementation of the author’s program. External load monitoring differed between teams, and not all used GPS tracking systems; given the strong influence of training volume and intensity on injury occurrence, tighter control of these parameters would have strengthened the interpretation of results.
Studying an individualized prevention program for hamstring injuries in football is inherently complex. Injury typically occurs when external forces exceed the organism’s capacity, yet these external forces and environmental constraints are extremely difficult to quantify in dynamic sporting contexts. Football, in particular, is highly variable, involving constant player interaction, heterogeneous surfaces, and a broad repertoire of movement solutions. In contrast, sports such as gymnastics are more codified, making external loads easier to characterize. Furthermore, as highlighted in previous research on sprint biomechanics and hamstring injury risk, multiple factors interact simultaneously, making it difficult to isolate the effect of a single prevention program. Large sample sizes are therefore required to detect meaningful intervention effects.
Talk Nerdy to Me
Because the study included fewer participants than the sample size calculation recommended (93 per group vs. 90 and 83 actually analyzed), the analyses were underpowered. An insufficient number of participants reduces the precision of the estimated effects and increases statistical noise, making it harder to detect true differences between groups. In an underpowered model, adjustments for confounders (such as age, team, anthropometrics, or previous HMI history) also become less reliable and more prone to instability. As a result, residual or unmeasured confounding may have had a greater influence on the findings, and the study may either fail to detect a real effect or produce estimates that are more vulnerable to bias.
Although the authors attempted to compensate for poor compliance by conducting simple correlations between compliance levels and HMI occurrence, this strategy is inherently limited. Correlation does not control for the many confounding variables that influence injury risk (e.g., training load, prior injuries, team practices, or physical characteristics). Consequently, the statement that “higher compliance was associated with lower HMI incidence” is considerably weakened. More robust analytical approaches—such as multivariable models, stratified analyses, or mixed-effects models—would have allowed adjustment for these confounders and yielded stronger, more reliable evidence. Without these methods, the true effect of compliance may be underestimated, overestimated, or distorted by uncontrolled variables, substantially downgrading the strength of the findings.
A similar limitation applies to the reported link between declines in horizontal force and increased HMI risk. The use of odds ratios captures only a statistical association, showing that reduced horizontal force and higher injury risk vary together, but it does not establish any causal mechanism.
Take-Home Messages
- Reduce injury burden, not just incidence: While the program didn’t significantly lower HMI risk per player, it reduced overall days lost, improving team availability.
- Compliance is crucial: Higher adherence to knee flexor strength training and maximal velocity sprinting was correlated with lower injury incidence. Ensuring consistent program delivery is essential.
- Monitor performance changes: Declines in posterior-chain strength and sprint force correlated with higher HMI risk. Regular screening can identify at-risk players.
- Adopt a multifactorial approach: Effective individualized prevention program for hamstring injuries should include posterior-chain strength, lumbopelvic control, flexibility, triceps surae health, and sprint mechanics to provide a more holistic injury-prevention strategy.
- Control training load: Variations in volume and intensity affect HMI risk. Consistent external load monitoring supports better prevention strategies.
- Study limitations: The study was underpowered, had high player dropout, COVID-19–related delays, and variability in program implementation and external load monitoring. These factors limit the strength of conclusions.
- Understand sport-specific challenges: Football’s dynamic nature and multiple interacting risk factors make isolating prevention effects difficult, but multifactorial, individualized programs can still reduce team injury burden.
To explore more about injury prevention programs in football, check out this Physiotutors article review
For a deeper dive into injury prevention strategies, listen to this Physiotutors podcast and explore their masterclass for advanced insights!
Reference
Annex
THE ROLE OF THE VMO & QUADS IN PFP
Watch this FREE 2-PART VIDEO LECTURE by knee pain expert Claire Robertson who dissects the literature on the topic and how it impacts clinical practice.
