
Research
Exercise
March 3, 2025
Stroke Recovery: How Extrinsic Feedback and Rewards Drive Upper Limb Motor Gains

Introduction
Extrinsic feedback, which refers to information provided to an individual about their performance from an external source (such as a coach, therapist, or technological device), plays a critical role in motor control. It has been shown to enhance both performance and learning in healthy individuals and stroke survivors. However, there is no clear consensus on the most effective methods for its implementation or the specific outcomes that should be targeted.
Research shows that different types of feedback—such as error correction, rewards, and punishments—can influence motor learning and neuroplasticity, depending on factors like sensory modality, timing, and frequency. Feedback can impact motor performance, long-term learning, and action selection, each crucial for stroke recovery.
This review aims to fill gaps in the literature by examining how extrinsic feedback affects upper extremity motor function post-stroke. It compares feedback conditions and explores how parameters like sensory modality and motivation influence recovery, offering a more up-to-date and comprehensive analysis of feedback in stroke recovery rehabilitation.
Methods
This scoping review followed the PRISMA guidelines for systematic reviews and meta- analyses. Eligible studies included peer-reviewed articles in English with the following criteria: participants were adult stroke survivors (greater than 18 years of age), performed tasks or therapies involving the affected upper extremity with extrinsic feedback, and included at least two experimental groups with differing feedback conditions. Studies that focused on error augmentation or reduction were excluded.
The search strategy, developed by a health sciences librarian, was conducted in MEDLINE, Embase, PsycInfo, and CINAHL. No date or language restrictions were applied. After deduplication in Endnote, the articles were screened by two independent reviewers using Rayyan software. Discrepancies were resolved through discussion.
Data extraction was performed using a standardized form in Covidence software, with two independent reviewers. The extracted data included study design, participant characteristics (age, sex, stroke type, lesion location, etc.), intervention details (task performed, number of movements), feedback characteristics (concurrent to movement, summary), valence (feedback stimuli delivered for good or bad performance) and study results (motor outcomes). These data were summarized in tables and descriptive overviews, focusing on clinical outcomes, motor performance (immediate changes in motor function in response to feedback), motor learning (changes in motor performance measured in the absence of feedback following repeated practice of a specific task), and action selection (increased use of the affected upper extremity or decreased use of compensatory movement patterns).
Results
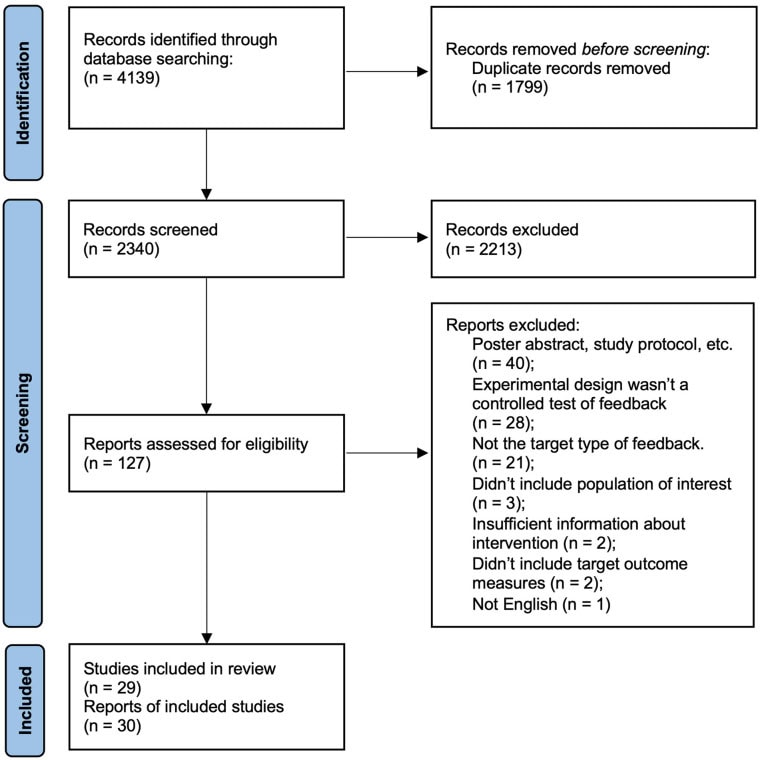
Search and Screening Process:
Out of 4,139 records, 1,799 duplicates were removed, and 2,213 records were excluded during initial screening. 127 full-text articles were reviewed, resulting in 30 included studies. Two publications were grouped as a single study for analysis.
Study Characteristics:
Fifteen studies utilized between-group designs, with 13 of them being randomized controlled trials (RCTs). The sample sizes in these studies ranged from 11 to 45 participants. Additionally, thirteen studies employed within-participant designs, with sample sizes ranging from 5 to 43. The majority of participants in these studies were stroke patients, including individuals with ischemic, hemorrhagic, or unspecified types of stroke.
Clinical Characteristics:
The clinical characteristics of participants across the studies varied. Two studies focused exclusively on ischemic stroke, while 14 included both ischemic and hemorrhagic stroke patients. Thirteen studies did not specify the type of stroke, and 22 studies did not report the vascular territory of the stroke. For those that did, affected areas included the middle cerebral artery, anterior cerebral artery, anterior and posterior circulations, and lacunar strokes. Seven studies included both cortical and subcortical lesions, while 22 did not specify the lesion type. No study examined the relationship between lesion characteristics and feedback effects.
Stroke duration varied from acute (less than two weeks) in four studies, early subacute (2 weeks to 3 months) in 12 studies, late subacute (3 to 6 months) in 10 studies, and chronic (greater than 6 months) in 20 studies. One study did not specify stroke duration, and no studies analysed how chronicity might relate to outcomes.
Regarding cognitive impairment, 12 studies excluded participants with cognitive function below a certain threshold (MMSE or MoCA), and 13 excluded those with aphasia. Nine studies excluded participants with neglect, and only two studies included cognitive function as part of the analysis. Cirstea et al. found that greater cognitive impairment was associated with worse motor learning, particularly in tasks involving verbal feedback. Quattrocchi et al. controlled for cognitive function but did not report its impact on the results.
Effects of Feedback:
Clinical Outcomes: Nine studies reported significant effects of feedback on clinical outcomes. According to the ICF model eight studies showed effects on body functions and structures, seven on activities, and three on participation. The movements performed during rehabilitation tasks were diverse, ranging from 3- dimensional reaching to more complex functional tasks such as pouring water or combing hair. Feedback typically targeted specific aspects of movement, including accuracy, speed, range of motion, upper limb kinematics, trunk kinematics, and force production.
However, the effect sizes varied, with only four studies showing benefits that exceeded established thresholds for minimal clinically important differences. The lack of consistent effect sizes may be attributed to the small sample sizes, heterogeneity of interventions, and the absence of minimal clinically important difference estimates for several outcome measures.
Performance: Five studies reported that feedback improved motor performance, specifically enhancing the speed, accuracy, and quality of movements during reaching tasks. These improvements were immediate but did not always persist after feedback was removed. Cruz et al. found that feedback based on movement rate and amplitude improved both factors. Durham et al. discovered that feedback inducing an external focus of attention improved movement duration, velocity, and acceleration. Rizzo et al. showed that gaze position feedback improved accuracy and reaction time.
Motor Learning: Four studies explored the effects of feedback on motor learning, defined as improvements in task performance assessed post-practice without feedback. Three studies focused on 3D reaching movements. Maulucci and Eckhouse found that feedback on trajectory deviation improved adherence to the ideal path and reduced hand oscillations. Cirstea and Levin, along with Cirstea et al., showed that feedback on shoulder and elbow extension improved joint range of motion and coordination, while hand location feedback improved endpoint precision. Subramanian et al. found that feedback in a gamefied virtual reality improved shoulder range of motion, but not in a physical environment. Quattrocchi et al. discovered that feedback linked to monetary rewards and punishments enhanced learning, with rewards only supporting retention during a 2D reaching task.
Action Selection: Five studies explored the effects of feedback on action selection, defined as changes in movement patterns. Four studies reported that feedback led to immediate and short-term reductions in compensatory movements during simple reaching tasks. For example, Cai et al. found that audio-visual feedback in virtual reality reduced compensatory trunk movements. Similarly, Douglass-Kirk et al. used musical feedback to stop whenever compensatory movements were detected, leading to reduced compensation. Other studies found that both visual and haptic feedback reduced trunk displacement. Overall, feedback consistently reduced compensatory movements by about 40-50%. However, one study by Fruchter et al. did not find reductions, likely due to the task’s complexity and manual control of the feedback. Schwerz de Lucena et al. found that wearable feedback increased hand use but showed no differences in clinical outcomes or hand use at follow-up.
Characteristics of Feedback:
Modality: Sixteen studies used non-verbal auditory feedback, 18 studies used non- verbal visual feedback, 4 studies employed haptic feedback, and 4 studies used verbal feedback (either by therapists or automated systems). Only one study compared the effects of feedback with similar informational content delivered through different sensory modalities and found that visual and haptic feedback led to similar reductions in compensatory movements.
Valence: Nineteen studies included feedback indicating unsuccessful task performance (negative valence), 14 studies used feedback indicating successful task performance (positive valence), and 8 studies delivered performance feedback with neutral valence, such as a point score without framing it as good or bad. One study directly compared positive versus negative valence feedback, finding that while both improved motor learning acquisition, only positive feedback enhanced retention.
Timing: Fifteen studies provided continuous feedback during movements, while another 15 studies delivered terminal feedback at the end of movements. One study did not specify the timing of feedback. Only two studies mentioned the delay of terminal feedback: Fruchter et al. reported a 3-4 second delay, and Widmer et al. imposed a 1- second delay in the control condition to reduce feedback efficacy. No study specifically varied the timing of feedback while controlling for other feedback characteristics.
Scheduling: Twenty-two studies provided feedback for every movement or the possibility of feedback with each movement. Three studies used faded feedback, gradually reducing the frequency of feedback over time. Two studies provided intermittent summary feedback on upper extremity use during daily life. One study used a decision tree algorithm to determine when feedback was delivered. Two studies did not specify the frequency of feedback. No study specifically varied the scheduling of feedback while controlling for other factors.
Motivational Elements: Two studies linked monetary rewards to performance feedback, and one study used monetary punishment. Eleven studies incorporated gamified scoring, while five studies used virtual or augmented reality. Two studies delivered feedback through musical stimuli, and one study used social comparison in the form of a high score list. Four studies compared feedback conditions with different motivational elements, such as monetary incentives, gamified scoring, and complex multisensory stimuli. These studies found that adding motivational elements improved motor learning and stroke recovery. Simple game scoring and virtual reality stimuli improved reaching kinematics, while a more elaborate gamified experience combined with monetary rewards led to clinical gains well above minimum clinically important differences.
Questions and Thoughts
The reviewed studies lack consistent criteria for participant selection, particularly regarding cognitive impairments. Most excluded individuals with cognitive disorders, leaving critical gaps in understanding how these impairments influence feedback interventions. Given the diversity in cognitive and stroke characteristics (e.g., ischemic vs. hemorrhagic, lesion location), future research should stratify participants based on these factors to improve generalizability and explore whether feedback interventions need tailoring to specific profiles.
Many studies focus solely on short-term feedback effects, often within a single session, neglecting the evaluation of retention and transfer of motor learning to real- world contexts. Assessing long-term efficacy, such as the ability to perform motor tasks independently in daily life, remains crucial. Future studies should prioritize retention testing beyond the clinical setting to better capture meaningful, lasting outcomes.
While visual and proprioceptive feedback show promise, their long-term effects and ability to transfer to functional, everyday tasks are underexplored. Improvements in task-specific performance (e.g., grasping or reaching) may not necessarily translate into broader functional recovery. Rehabilitation protocols should emphasize tasks aligned with patients’ real-life goals to maximize functional relevance.
Extrinsic feedback enhances short-term motor performance but risks fostering dependency, hindering long-term stroke recovery. Strategies to prevent over-reliance on feedback are necessary to foster autonomous motor control. We can hypothesize that a phased approach integrating both extrinsic and intrinsic feedback could promote autonomy while providing initial support. Future research should examine how to balance these systems for sustainable rehabilitation outcomes.
Talk Nerdy to Me
The generalizability of findings is limited by inconsistent participant criteria. Many studies excluded individuals with cognitive impairments or failed to account for stroke severity, lesion location, or type (ischemic vs. hemorrhagic). This oversight restricts understanding of how these factors influence feedback efficacy. Only two studies incorporated cognitive measures, highlighting a significant gap in addressing how cognitive deficits interact with feedback mechanisms.
The studies employed varied statistical approaches (e.g., repeated measures ANOVA, t-tests, regression models), but small sample sizes often compromised statistical power. When studies are underpowered, there is a greater likelihood of type II errors, which occur when a study fails to detect a real effect despite one existing. For example, an intervention that genuinely improves motor learning might appear ineffective simply because the sample size was too small to reveal statistically significant differences. Additionally, many analyses did not sufficiently account for moderators such as baseline motor function or cognitive capacity, which are critical for understanding feedback effectiveness. Effect sizes varied widely across studies, likely reflecting methodological diversity rather than consistent evidence of feedback efficacy.
Take-home messages
Extrinsic feedback, delivered through various modalities (visual, auditory, haptic), shows promise in enhancing motor performance and reducing compensatory movements in stroke rehabilitation. It can immediately improve task performance, such as speed, accuracy, and joint range of motion. However, the long-term impact on motor learning and functional recovery outside the clinical setting remains unclear. Feedback can help encourage proper limb use, but over-reliance may hinder the development of autonomous motor control. Incorporating motivational elements, such as gamification and rewards, seems to improve motor learning, yet the underlying mechanisms remain poorly understood. Clinicians should choose therapeutic activities that closely align with the patient’s functional goals to enhance the transferability of skills and optimize the effectiveness of extrinsic feedback. Future research should focus on personalized interventions, consider cognitive impairments, and evaluate the long-term sustainability of feedback interventions to maximize stroke recovery outcomes.
Reference
Learn more
CHALLENGE: TAKE THE QUIZ THAT 75% OF PHYSIOTHERAPISTS FAIL
Answer these 10 short questions on essential knowledge each physiotherapist should know and find out if you score better
