Research
Head/Neck
December 19, 2022
Predicting Positive Outcome After Multidisciplinary Orofacial Treatment in Patients With Somatosensory Tinnitus

Introduction
A while ago, we posted this research review on an RCT examining the effects of orofacial physical therapy treatment on tinnitus. This trial showed significant decreases in tinnitus annoyance after multidisciplinary orofacial physical therapy treatment (as can be seen from the within-group analysis), however, this reduction in the primary outcome measure did not reach the clinically meaningful threshold. But there’s more to it, as you can read in our review. This study was based on this RCT and sought to find factors predicting a positive outcome in tinnitus (that was classified as temporomandibular-related somatic tinnitus) after multidisciplinary orofacial treatment.
Methods
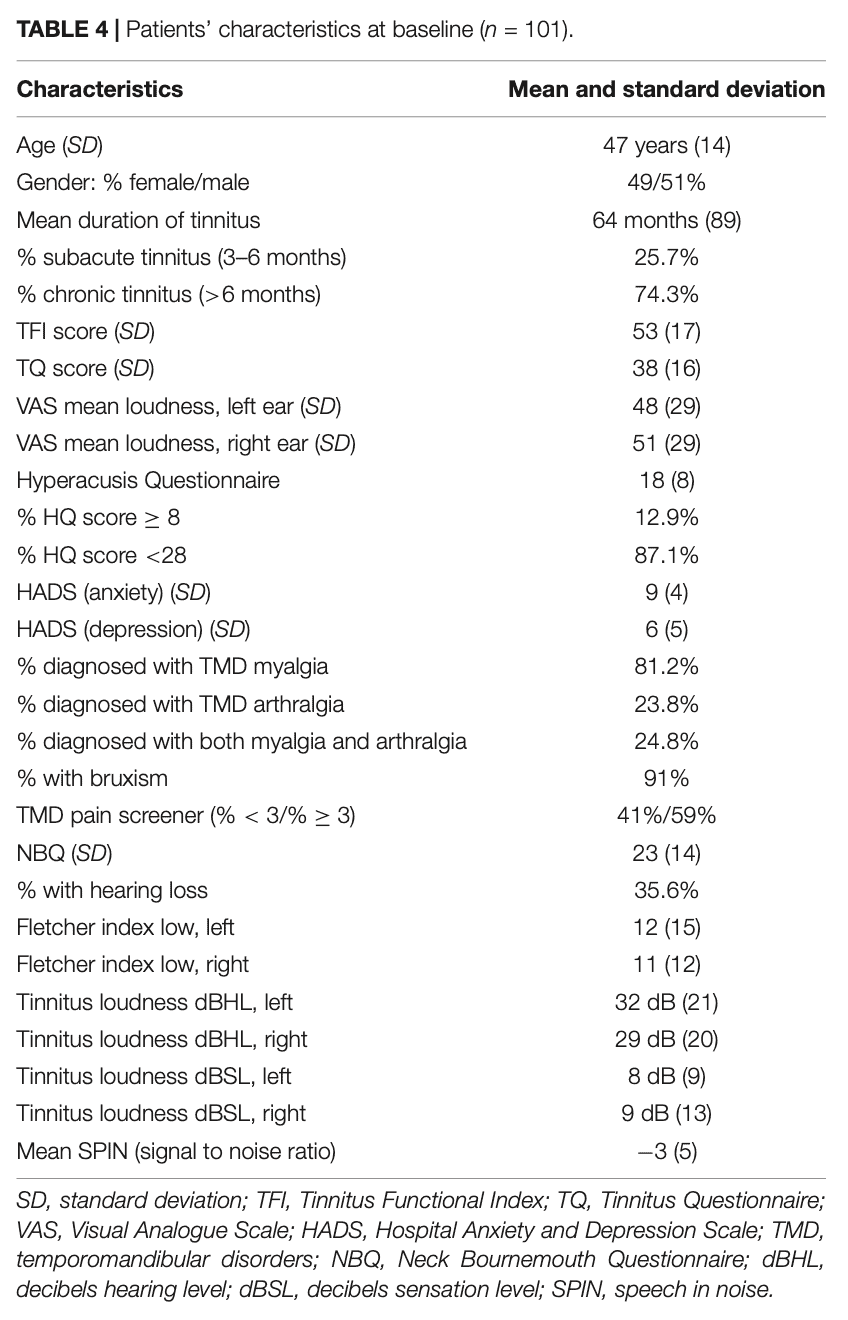
This study included adult patients with moderate to severe (Tinnitus Functional Index score between 25 and 90) chronic subjective tinnitus that was attributed to the temporomandibular area. This was confirmed by the presence of a painful temporomandibular disorder, as diagnosed with the Diagnostic Criteria for TMD (DC-TMD). The complaints had to be stable for at least 3 months.
In the RCT, the participants received a maximum of 18 physiotherapy sessions over a 9-week course. This treatment was multidisciplinary and targeted bruxism, sleep, lifestyle advice, biofeedback, relaxation, and stretching of the masticatory muscles. Counseling to reverse parafunctional mouth habits was also provided. Participants with teeth grinding were offered an occlusal splint. In case the cervical spine was involved in the complaints, this was addressed as well.
The primary outcome of the RCT was the Tinnitus Questionnaire (TQ) and a secondary outcome was registered through the Tinnitus Functional Index (TFI). The TQ measures tinnitus annoyance and the TFI measures the severity of tinnitus. Clinically relevant improvements are achieved when the TQ decreases by 8.72 points and the TFI by 13 points.
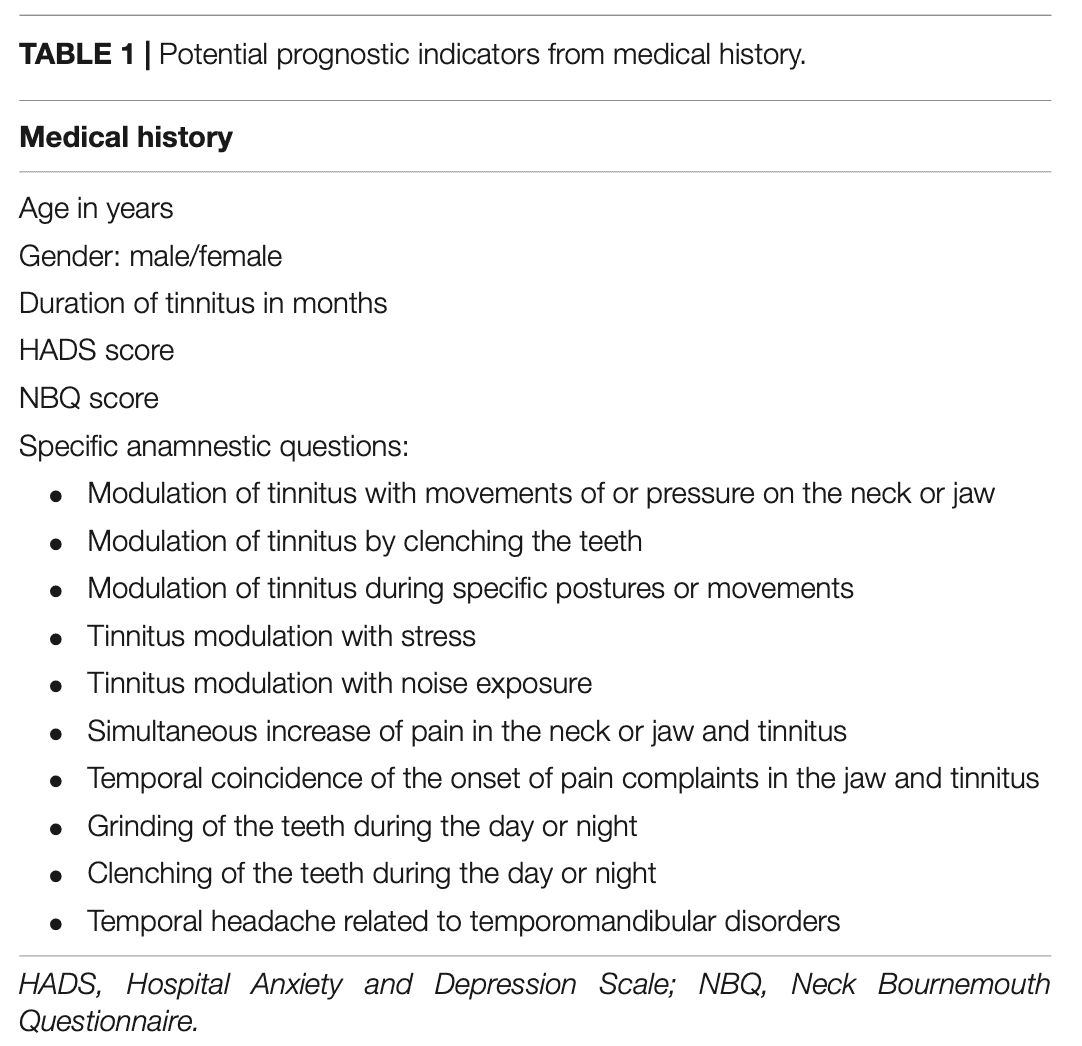
Factors predicting a positive outcome in tinnitus after multidisciplinary orofacial treatment were selected from medical history, temporomandibular assessment, audiological assessment. The choice for these factors was based on the existing knowledge about their possible influence on the course of the temporomandibular symptoms. The following table displays the medical history factors that had been selected for their prognostic ability.
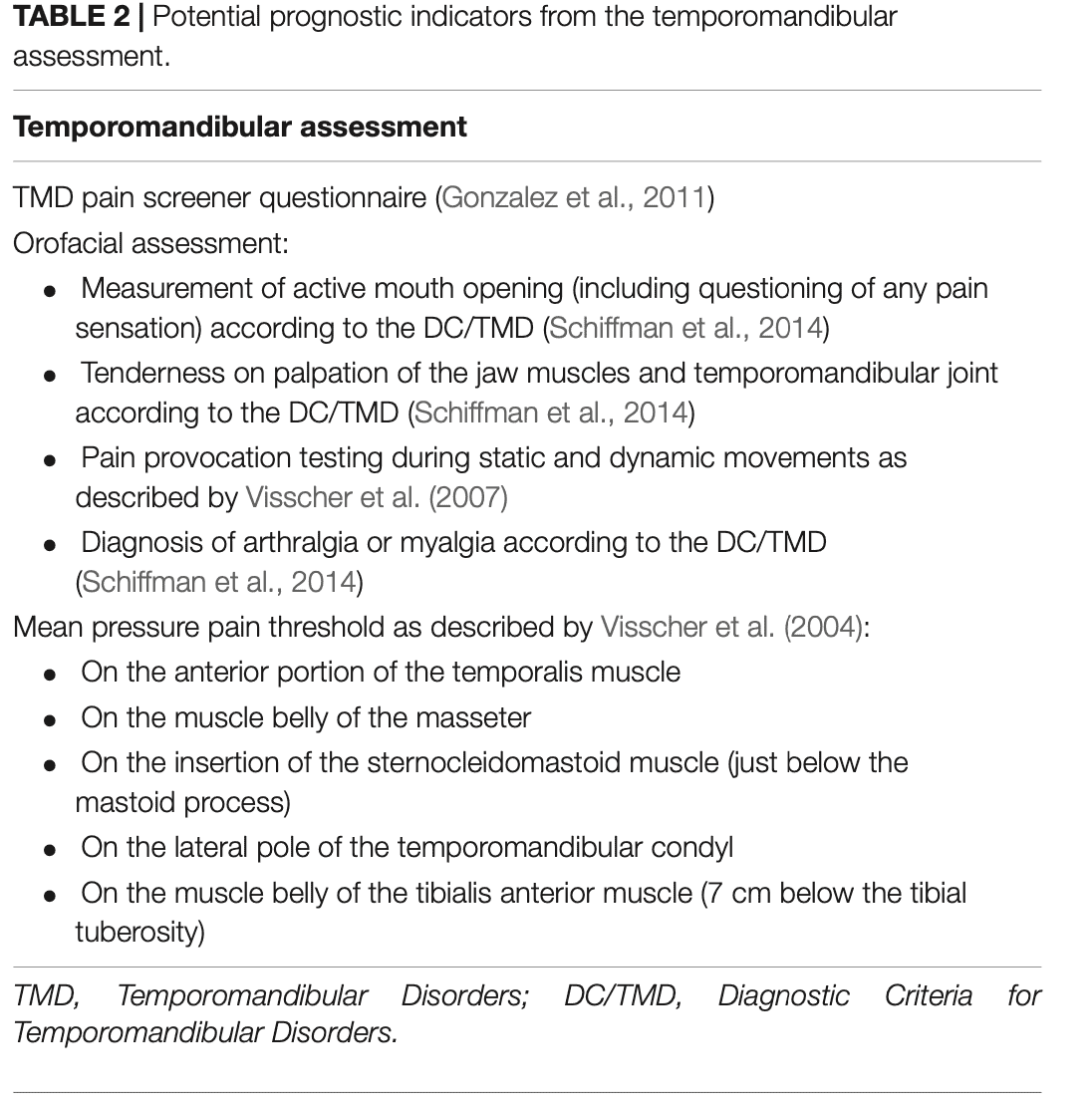
Hereunder, you can find the selected potential prognostic indicators for the temporomandibular assessment.
Results
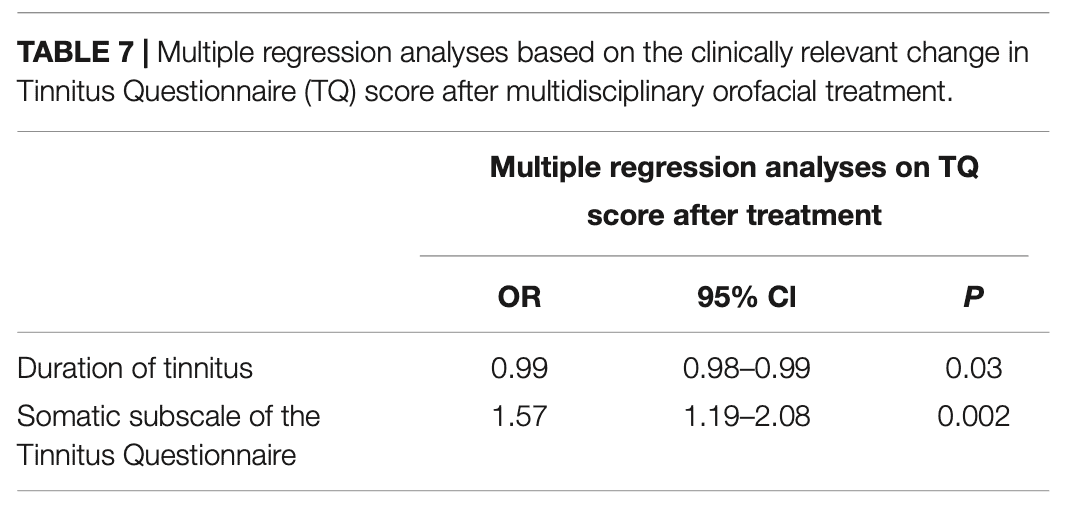
The sample was composed of the RCT (80 patients) and 21 patients were added from an additional cohort to have data on 101 participants in total. It seems that the duration of the tinnitus complaints and the score on the somatic subscale of the TQ were predictive for obtaining a clinically relevant improvement on the TQ. A shorter duration of the complaints and a higher initial score on this subscale of the TQ were predictive and this model could correctly predict the outcome of the TQ in 68.5% of the individuals.
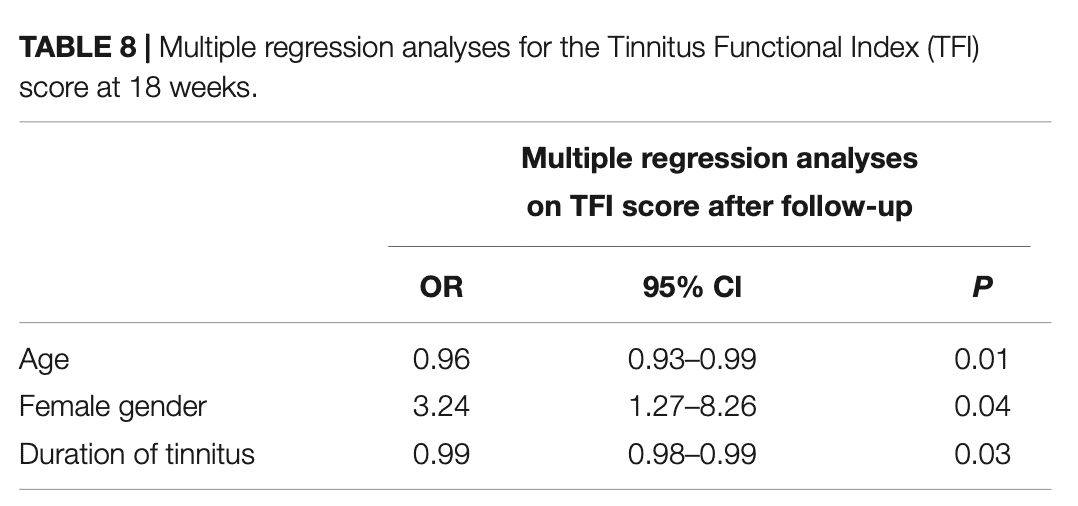
Considering the TFI, age, gender, and the duration of tinnitus were identified as factors predicting a positive outcome in tinnitus. A younger age, a shorter duration of the tinnitus complaints, and being female could predict a clinically significant decrease in the TFI in 68.1%.
Questions and thoughts
Diagnosis of painful TMD was based on the DC-TMD with or without oral parafunction (like bruxism). It was stated that: “Apart from tinnitus, the patients had to have a painful TMD, diagnosed according to the Diagnostic Criteria for TMD (DC-TMD) and/or oral parafunction.” The way I see it is that the temporomandibular involvement was diagnosed through either the DC-TMD OR the presence of parafunctions. Here it must be acknowledged that the presence of oral parafunctions itself does not mean there is a temporomandibular disorder, so I find it a bit strange at least. Of course, these parafunctions can be contributors to temporomandibular complaints but they cannot be viewed as a diagnostic unicum for temporomandibular disorders.
Predicting a positive outcome in tinnitus was possible considering 2 and 3 factors only for tinnitus annoyance and severity, respectively. This is particularly useful as we do not need to assess a ton of factors to have an idea of how this patient will respond. This promotes the uptake of the prediction model in clinical practice. However, the validity of the prediction model should further be analyzed in a distinct sample.
Talk nerdy to me
The fact that this model was developed based on the outcomes of participants included in a randomized controlled trial limits the generalizability of the results. The reason therefore is that RCTs use very strict criteria and generally consist of a limited number of participants. Patients in your general practice do not always fit the strict criteria that the study population had prior to being included in the RCT. For example, you will get a referral from a general practitioner for someone with tinnitus. The doctor may know that you are in fact interested in such pathologies and may directly refer the patient to you, without having him checked audiologically. Here in the present study, you know from the audiological examination that the patient did not have problems with hearing for example. The patient that gets referred to you however has not been checked audiologically and you have no idea about the possible contribution of the auditory system to the tinnitus complaints. I hope this example shows you that RCTs have very little generalizability to the wider population in general. The best thing you can do is to check the characteristics of the included patients and compare them to the patients you see in your clinic. Are their baseline characteristics quite similar? Then you can have an idea of the possibility that your patient may respond equally to therapy procedures as described by a trial. Patients from this trial were also screened by an audiological assessment, which is beyond the competencies of a physiotherapist. Yet, this assessment confirmed that the tinnitus was not attributable to hearing problems. This is important to consider when you get a referral for such a patient.
Another point to note was that it was possible for the patients to have similar neck problems and therapy could also address them. Patients often suffer from more than 1 issue and that this was possible resembles general practice. Yet, the fact that they were offered cervical spine treatment may have had an influence on the outcome. The same counts for the use of an occlusal splint in those with teeth grinding. It is therefore plausible that the benefits from the treatment are not attributable to the temporomandibular joint therapy only. Yet, I acclaim the use of personalized care rather than investigating standardized treatments as this resembles the way we care for people more. It was further shown that there was no difference in the use of occlusal splints between males and females so the better outcome in females was not influenced by splint use. Something that may be relevant in this light is that females are more likely to develop temporomandibular disorders than males, and this may have influenced why gender is a prognostic factor for improvement. However, the male-to-female ratio was similar in this study, we do not know whether they had more initial complaints. This could for example be relevant as higher initial complaints give more room for improvement and thus also a larger number of patients responding to treatment, thus a better prognosis for those people with higher baseline scores.
Patients had high scores for the presence of somatic complaints. This will likely respond to musculoskeletal treatment. In case more anxiety and depression features had been present, it may have been very likely that these good outcomes were not evident – as they need more counseling and pain education and management than people with a more musculoskeletal origin of their complaints do.
Take home messages
Factors predicting a positive outcome in tinnitus severity include younger age, being female, and having a shorter duration of the tinnitus complaints. Considering tinnitus annoyance, the factors predicting a clinically significant outcome are a shorter duration of the complaints and a higher initial TQ score. These factors could correctly predict the outcome of the TQ and TFI in 68.5% and 68.1% of patients, respectively.
Reference
100% FREE HEADACHE HOME EXERCISE PROGRAM
Download this FREE home exercise program for your patients suffering from headaches. Just print it out and hand it to them for them to perform these exercises at home