
Research
Knee
July 25, 2022
Arthroscopic partial meniscectomy versus physical therapy for traumatic meniscal tears in a young study population

Introduction
When you are a young active individual and sustain a traumatic meniscus tear, chances are high that you will be offered arthroscopic surgery. Most often, a partial meniscectomy will be performed. It is believed that surgery is needed in young athletes, but it has never been confirmed in high-quality trials that arthroscopic partial meniscectomy is the preferred option. Since there is no scarcity in this area of research in middle-aged and elderly patients, the persuasion not to undergo meniscectomy is clearly outlined in guidelines for this patient group. Nevertheless, this recommendation cannot simply be extended to other domains. This, together with the belief that surgery is necessary for young active individuals, justifies why this RCT aimed to investigate arthroscopic partial meniscectomy versus physiotherapy for traumatic meniscus tears in this population.
Methods
A multicentre randomized controlled trial was conducted between 2014-2018 in 8 hospitals in the Netherlands. After referral, patients aged 18-45 years with a recent knee trauma (previous 6 months) were recruited from outpatient clinics. Only full meniscus tears, where MRI shows signal changes that reach the articular surface (grade 3) were included.
With a stratified randomization process, participants were allocated to either the arthroscopic partial meniscectomy or physiotherapy for traumatic meniscus tears. Patients in the arthroscopy group were treated within 6 weeks of their randomization, but if this was equally so for the physiotherapy group wasn’t specified.
Not all patients who underwent the arthroscopic partial meniscectomy were referred to physiotherapy post-operatively, but they were allowed to do so. After the arthroscopy, patients were treated according to routine clinical practice and the Dutch national guidelines. Patients randomized to the physiotherapy group participated in a standardized program lasting for at least 3 months where the focus was on reducing knee effusion, optimizing range of motion, and stimulating activities and participation in sport. Next to the supervised sessions, a home exercise program was also given.
The outcomes assessed were the 2-year IKDC score, which measures the patient’s perception of symptoms, knee function, and ability to participate in sports. The score ranges from 0-100, with 100 representing an optimal score.
Results
In total, a hundred patients were randomized to either arthroscopy or physiotherapy for traumatic meniscus tears, 49 and 51 in each group respectively. Data of 91% was available to analyze at follow-up. In total, six patients (12%) of the arthroscopic partial meniscectomy group received no surgical treatment and in four patients (8%) in the surgical group, the surgeon decided during surgery to perform meniscal repair instead of partial meniscectomy, based on arthroscopy findings.
In the physiotherapy group, a median of 8.5 physiotherapy sessions was recorded per patient, while twenty patients in the surgery group (42%) had at least one session in the first 3 months, with a median of 5.0 sessions.
Twenty-one patients (41%) of the physiotherapy group underwent a delayed arthroscopic partial meniscectomy during the follow-up period in consultation with the orthopedic surgeon, because of persistent complaints. The time between randomization and delayed arthroscopic partial meniscectomy ranged from 3 to 21 months with a median duration of 5.5 months.
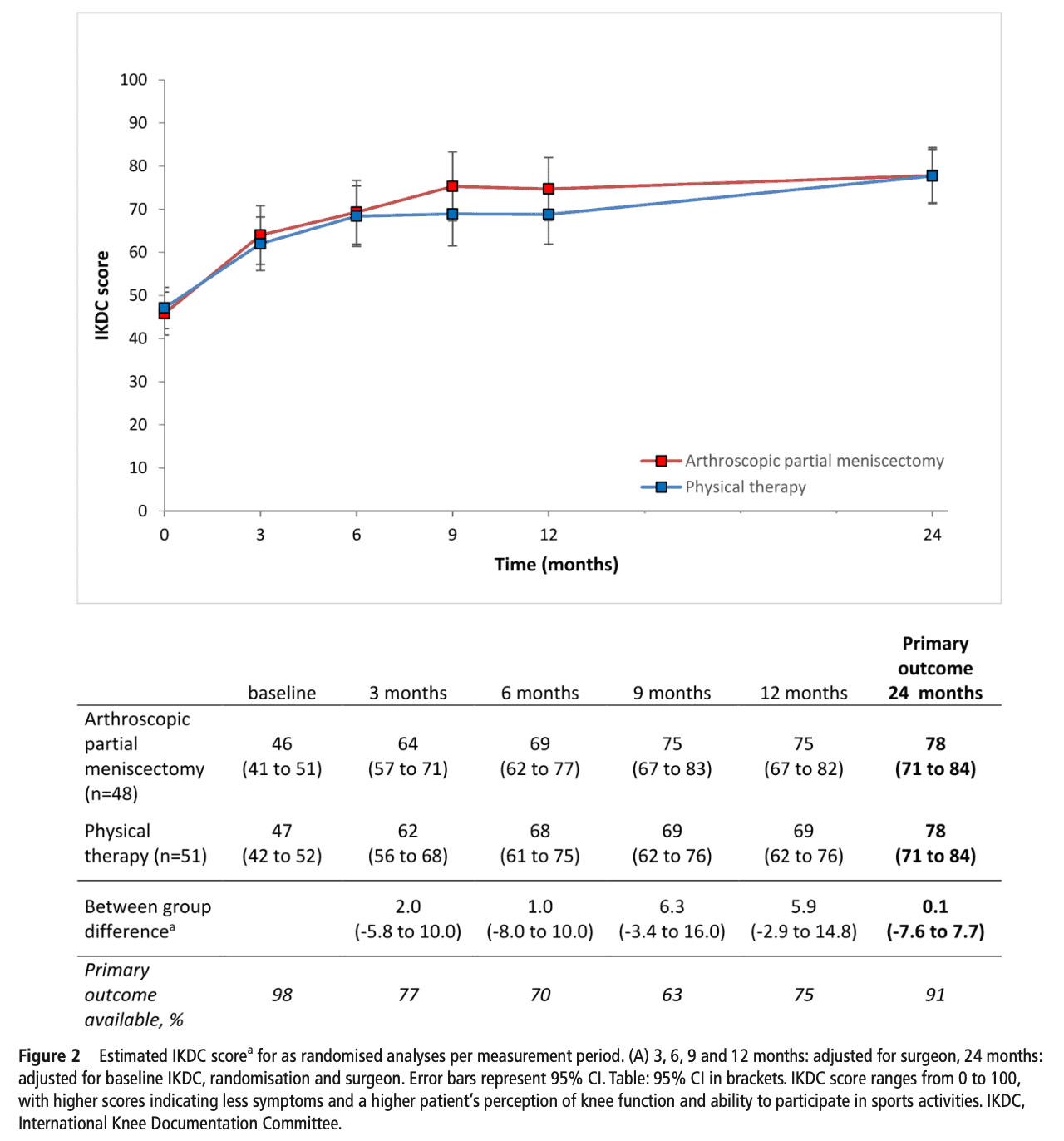
At 24 months, the IKDC showed no significant difference between the arthroscopic partial meniscectomy and the physiotherapy group. Both groups improved with nearly 30 points on the IKDC, which exceeded the minimal important difference of 13.9 points. The same was true when looking at the secondary outcomes, also no difference existed between the arthroscopy and physiotherapy groups.
Questions and thoughts
In none of the groups, a maximum IKDC score was obtained. This leads us to conclude that there may still be some room for improvement with more targeted rehabilitation. Perhaps if the physiotherapy sessions would have been held more frequently. As you read earlier, in the physiotherapy group, a median of 8.5 sessions were held over a period of 3 months. This is less than 3 per month and may have been insufficient. Of course, the program was supplemented with a home exercise program, but neither adherence nor compliance to the program was measured (or mentioned). Therefore, the exercise dose cannot be evaluated and this leaves us with some lingering questions. Also regarding the tailoring of the program to the individual. Though the authors mentioned that the physiotherapy program was standardized, it was individualized to the patient based on their functional level and knee status. However, no more details were given by the authors on how this tailoring was done.
Patients with a locked knee or with a concurrent rupture of the posterior or anterior cruciate ligament, and radiographic signs of OA (Kellgren Lawrence grade 2 or higher) were excluded from the trial. This is actually a good thing because it allowed the researchers to assemble a homogeneous group to compare both treatment options. Conversely, in real-life settings, patients may experience more than a meniscus tear alone, and therefore, the generalization of these results is limited. Also, meniscal tears that were suitable for suture repair based on MRI findings were excluded, which is a good choice of the authors as sparing the meniscus seems important to avoid early degenerative changes. On the other hand, patients could have minor cartilage damage accompanying the meniscus tear that wasn’t seen on MRI.
More than one-third of the included patients were competitive or elite athletes, having a Tegner score of at least 8, meaning participation in competitive high-intensity sports like for example hockey, squash, alpine skiing, football, etc… This is especially important because these patients are often the first to receive arthroscopic management as it is thought that this will increase their chances to return to their previous level of sports participation. So it appears not necessary to immediately treat high-level athletes arthroscopically! Yet, in high-level athletes, the urge to return to the highest level as soon as possible can be very high. The IKDC did not reach maximum values in any of the groups but evolved similarly in time. So maybe also in high-level athletes, higher-dosed physiotherapy for traumatic meniscus tears may do?
Talk nerdy to me
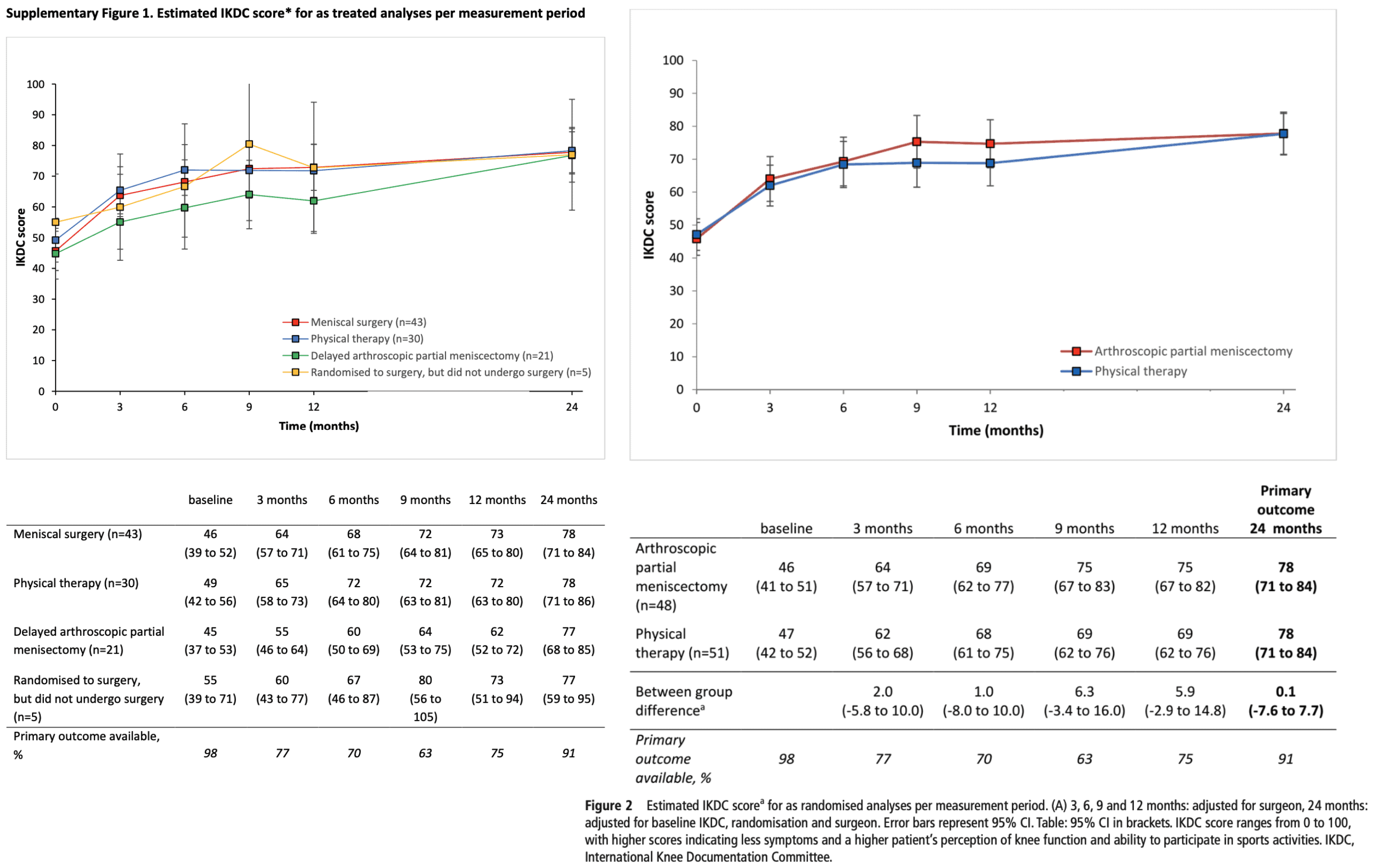
Many participants switched from the physical therapy group in which they were assigned to arthroscopy. Twenty-one in total! Therefore it is interesting to compare the intention-to-treat analysis with the as-treated analysis. Both analyses show no differences (as you can see in the underlying graphs, presented next to each other), so we can conclude that the cross-over of participants to surgery did not affect the primary outcome.
Whether the patient underwent arthroscopic meniscectomy or was treated with physiotherapy for traumatic meniscus tears, the IKDC score after 2 years reached the same level. Also in those who had neither arthroscopy nor physiotherapy (5 participants), and even in those who switched from the physiotherapy to arthroscopy group (delayed arthroscopy, 21 patients). This is quite remarkable and suggests that a much higher improvement could possibly have been achieved. Who knows, if the physiotherapy would have been better dosed…
Take home messages
Important to note that the meniscus tears studied here were all full tears grade 3 and that patients experiencing locked knee symptoms were excluded. At present, these results can thus only be extrapolated to grade 3 meniscus tears without joint locking symptoms. No difference was seen between arthroscopy or physiotherapy for traumatic meniscus tears, even in this sample where one-third of participants had a Tegner score of 8 or more, meaning they participated in high-level sports at baseline. A side note is that the mean Tegner score in both groups declined by 1 point in both groups at the 24-month follow-up. Confirming again the potential to do better in future trials!
Reference
Other of our relevant research reviews
https://www.physiotutors.com/research/9-in-10-degenerative-meniscus-tears-get-better-after-2-years/
Additional references
LEARN TO OPTIMIZE REHAB & RTS DECISION MAKING AFTER ACL RECONSTRUCTION
Sign up for this FREE webinar and top leading expert in ACL rehab Bart Dingenen will show you exactly how you can do better in ACL rehab and return to sport decision making
