
Research
Knee
July 4, 2023
Comparison of two patellofemoral pain exercise modes

Introduction
The best available evidence for patellofemoral pain recommends exercise as a first-line treatment. But uncertainty about the type of exercise remains. Quadriceps-focused exercises and hip-focused exercises or a combination of both have been suggested. However, as not many studies compare both options, this equivalence trial aimed to narrow this gap by investigating two common types of patellofemoral pain exercise.
Methods
This randomized controlled trial was conducted in Denmark and included patients who were referred by a primary care physician to the Institute of Sports Medicine Copenhagen Hospital. They had patellofemoral pain which was clinically diagnosed, and further they had a pain rating of 3 or more on a 10-point scale during ADL activities. The onset of pain was insidious, atraumatic, and persisted for at least 4 weeks. Further, at least three of the following criteria had to be present as well: anterior knee pain that was associated with prolonged sitting, stair ascent or descent, squatting, or pain during or after activities.
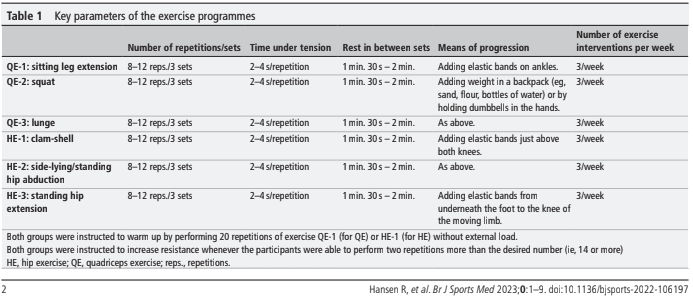
The patellofemoral pain exercise modes were either quadriceps exercises or hip exercises. The first included seated knee extension exercises, squats, and forward lunges. The hip-focused exercises included clam shells, side-lying/standing hip abduction, and prone/standing hip extension. Every participant was instructed individually on how to perform each exercise. Eight to twelve repetitions were performed and the aim was that the last repetitions were difficult, without affecting the movement quality. Therefore, elastic bands, free weights, and body weights were used to individually adapt the exercises to create sufficient loading. Whenever the participants were able to perform 14 repetitions, they received the instruction to increase the resistance.
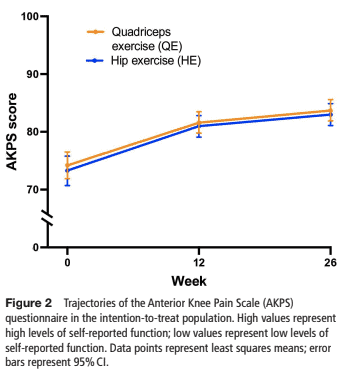
The primary outcome was the change from baseline in the Anterior Knee Pain Scale (Kujala Score – AKPS) at week 12. This score ranges from 0-100 and high scores indicate less patellofemoral symptoms. The minimal clinically important difference is 8-10 points.
Results
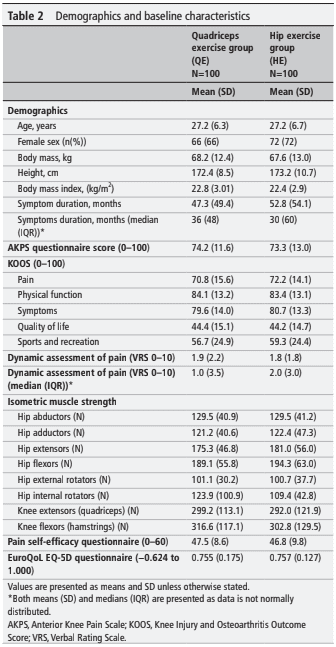
Two-hundred participants were equally randomized to the hip or quadriceps exercises. At baseline, they had similar characteristics. They were on average 27 years old and had a mean BMI of 22.6, 69% were females. The adherence to the programmed exercise sessions was on average 77%.
The primary outcome revealed that the quadriceps exercise group improved by 7.6 points. This was 7.0 points for the hip exercise group. This resulted in a non-significant group difference of 0.6 points. None of the interventions was thus superior to the other. Some exacerbation of symptoms was noted in 14 participants and the number of sets and repetitions or the ROM in weight-bearing exercises was then reduced. The secondary outcomes were in the same trend.
Questions and thoughts
What caused the lack of superiority of one of the exercise programs? Were the exercises of too low load? The authors mention that the loads were individually determined and adjusted when needed accordingly. But no information was provided on the presence or absence of these progressions in the study population. Therefore, it is hard to judge. The participants were instructed to perform 3 exercises only. This may have been too monotonous since ADL activities require more. As a supplemental home exercise program, I would certainly not overcomplicate things, but when this is the only intervention (no supervised sessions), it may have created too little variation. Especially, the quadriceps group only exercised in the sagittal plane. This may be partly the reason for not exceeding the MCID of 8-10 points in the AKPS
In light of these results, it is recommended to continue exercise programs combining the quadriceps, and hip exercises and add variation in movements. Sport- and activity-specific training and exercises along the entire kinetic chain remain the mainstay of patellofemoral pain exercise.
Talk nerdy to me
The baseline characteristics reveal an already high Kujala score in both groups (>70/100). This may partly explain the lack of improvements found, as this may have led to a ceiling effect. Another reason may be the lack of supervision and patient-therapist relation. Also, adherence was self-reported, but as no treatment sessions were supervised, it may have overestimated the true adherence to the exercise program. The intention-to-treat analysis uses the data from all participants respective to their allocation. Here also, non-adherence to the program may bias the results.
Take home messages
12-week quadriceps- and hip-focused exercises are equally effective in patellofemoral pain, although none of both was able to produce clinically meaningful results. The sample had already high scores on the primary outcome at baseline, which may have left no/little room for improvement. Other variables than strength may be decisive factors to obtain meaningful outcomes for patients with patellofemoral pain.
Reference
THE ROLE OF THE VMO & QUADS IN PFP
Watch this FREE 2-PART VIDEO LECTURE by knee pain expert Claire Robertson who dissects the literature on the topic and how it impacts clinical practice.
