Research
Exercise
June 15, 2026
Exploring partial rotator cuff tear management: A systematic review and meta-analysis comparing the efficacy of surgical intervention versus conservative care

Introduction
Rotator cuff disease (RCD) is one of the leading causes of shoulder pain and disability, encompassing a spectrum of conditions ranging from tendinopathy to full-thickness tears. Partial-thickness rotator cuff tears account for a substantial proportion of these cases, yet the optimal approach to management remains unclear. This large-scale review is the first to comprehensively synthesize the available evidence on treatment options for partial rotator cuff tear management, aiming to help clinicians identify the most effective management strategies.
Methods
This systematic review follows the PRISMA, PRISMA-S, and TRACiS guidelines.
Inclusion and exclusion criteria
This review included English-language clinical studies involving adults (≥18 years) with confirmed partial-thickness rotator cuff tears diagnosed through clinical examination or imaging. Both surgical and non-surgical intervention studies were eligible, including comparative and single-arm designs. Studies involving asymptomatic individuals, animal or cadaveric models, and in vitro research were excluded.
Study identification
Medical databases were systematically screened. To ensure a comprehensive overview, the authors included studies evaluating either treatment approach independently, enabling indirect comparisons across a broad body of evidence. Non-surgical interventions were combined into a single category despite the heterogeneity of approaches described in the literature. This approach increased inclusiveness and minimized the risk of selection bias, while the authors acknowledged that it may also increase clinical heterogeneity and affect the interpretation of the results.
Screening and data collection
Two independent investigators screened titles, abstracts, and full texts, and extracted data according to predefined inclusion and exclusion criteria. Any discrepancies were resolved through discussion with a third author. For each study, outcome data were extracted from the final follow-up assessment, using the Constant Score (CS), the American Shoulder and Elbow Surgeons (ASES) Shoulder Score, and the Visual Analog Scale (VAS) as primary outcome measures.
Data analysis
The authors used weighted means to compare overall outcomes between surgical and non-surgical groups, allowing an absolute comparison across studies. Mean differences were calculated only within surgical subgroups when direct comparisons were available.
A random-effects model was applied to account for between-study heterogeneity, which was assessed using I², τ², and chi-square statistics. Heterogeneity levels were interpreted using standard thresholds ranging from low to considerable. Forest plots were used to visually present pooled estimates and variability across studies.
Statistical significance was set at p < 0.05. When data were insufficient for meta-analysis, descriptive statistics were used instead. Overall, the authors explicitly accounted for heterogeneity and its potential impact on the interpretation of pooled results.
Results
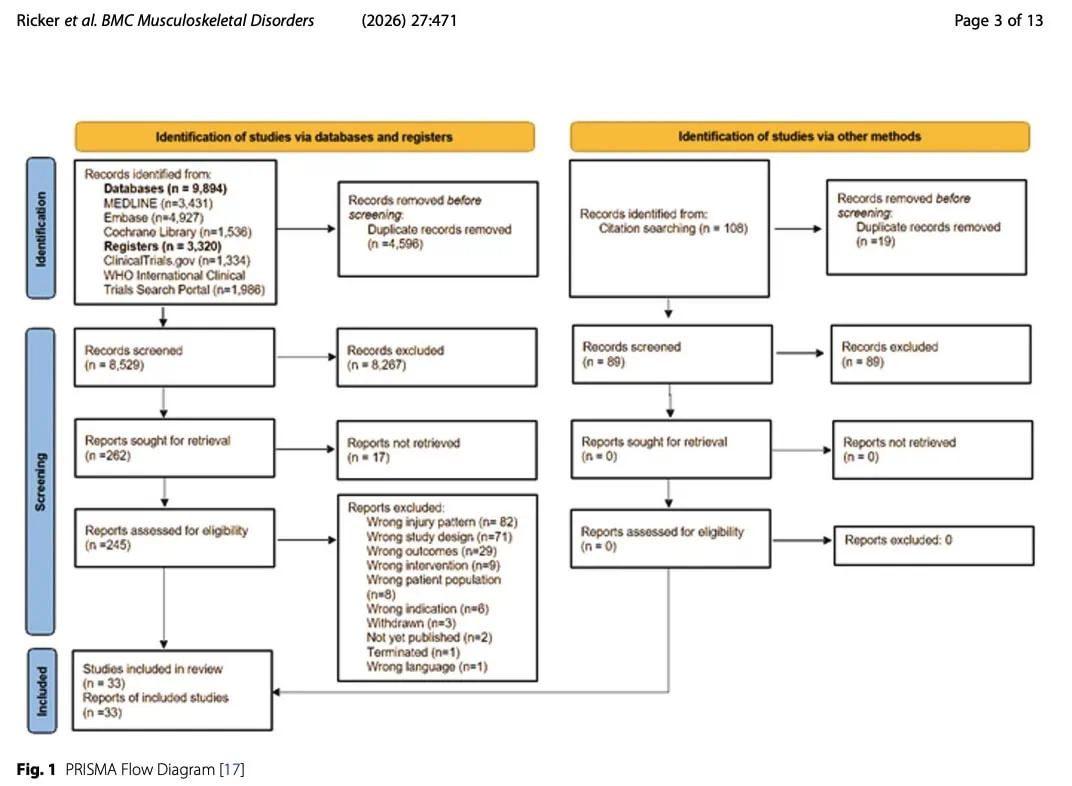
33 studies were included in the systematic review, with a total of 1818 participants
Arthroscopy vs. non-surgical management
A Level IIc study including 127 patients compared arthroscopic surgery (n = 50) with non-surgical treatment (n = 77) for rotator cuff ruptures, with data specifically extracted for partial-thickness tears.
Using the ASES score, surgical treatment showed significantly greater improvement than the non-surgical approach for partial rotator cuff tear management. A greater proportion of patients in the surgical group experienced substantial improvements in shoulder pain and function compared to the non-surgical group. Specifically, 88% of surgical patients improved by more than 30% from baseline versus 61% in the non-surgical group, while 86% of surgical patients achieved more than 50% improvement compared with 44% of non-surgical patients.
Overall, arthroscopic treatment demonstrated superior outcomes compared with conservative care in this study, based on functional and pain measures.
Arthroscopy
One Level II RCT including 78 patients compared immediate arthroscopic rotator cuff repair with delayed repair after six months of non-surgical treatment for partial rotator cuff tear management. Outcomes included the Constant Score (CS), ASES score, and VAS.
Both groups showed significant improvements in all outcomes compared with baseline. At six months, the group that underwent initial non-surgical treatment had better ASES and lower VAS scores; however, this difference disappeared by the twelve-month follow-up, with both groups showing comparable results.
This is an important timepoint-related limitation: concluding that one strategy is “superior” based on the six-month results would be misleading, because the apparent between-group difference was no longer present at twelve months. In this case, the findings suggest a difference in the speed or timing of recovery rather than a clearly superior outcome.
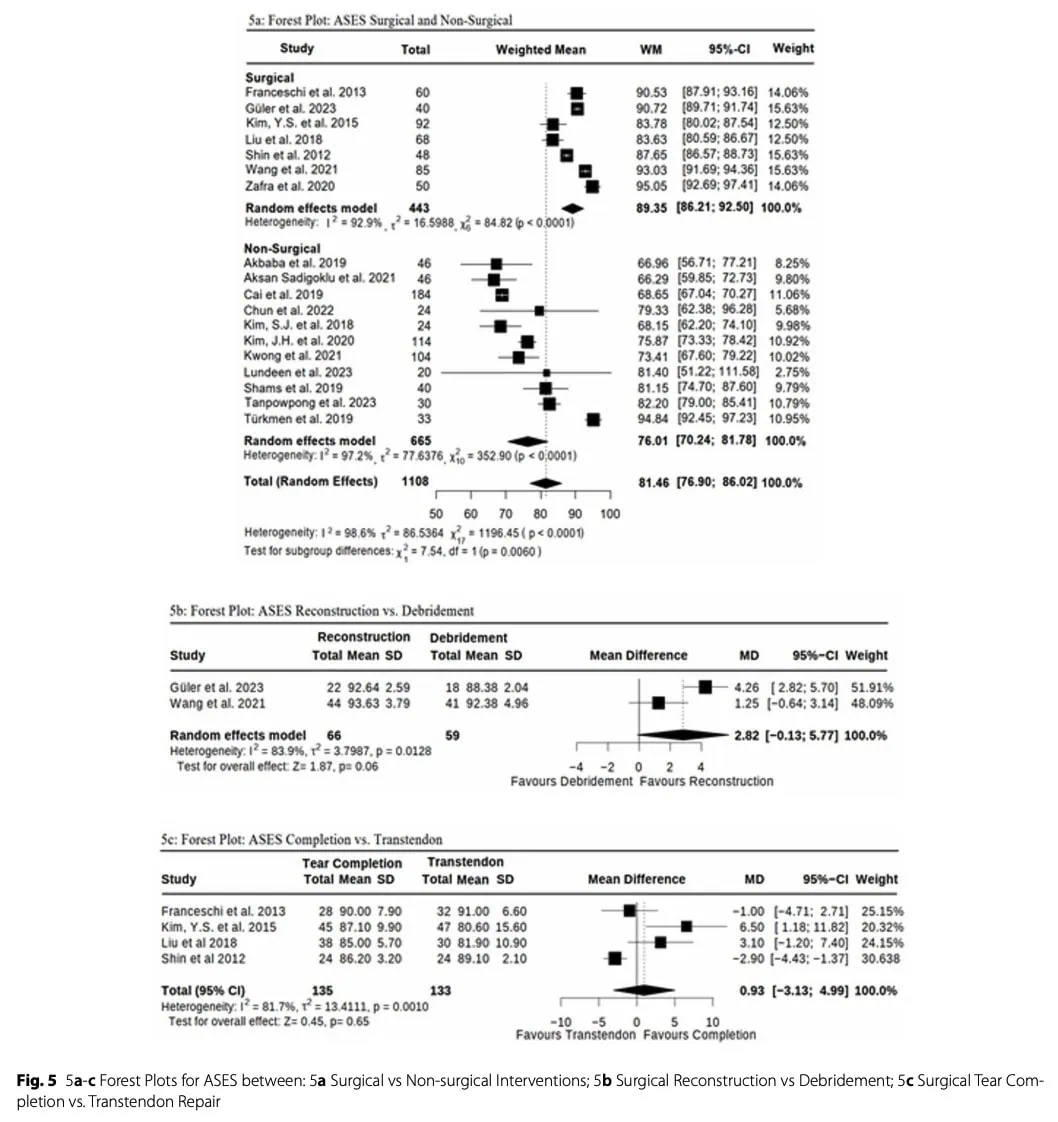
Debridement vs reconstruction
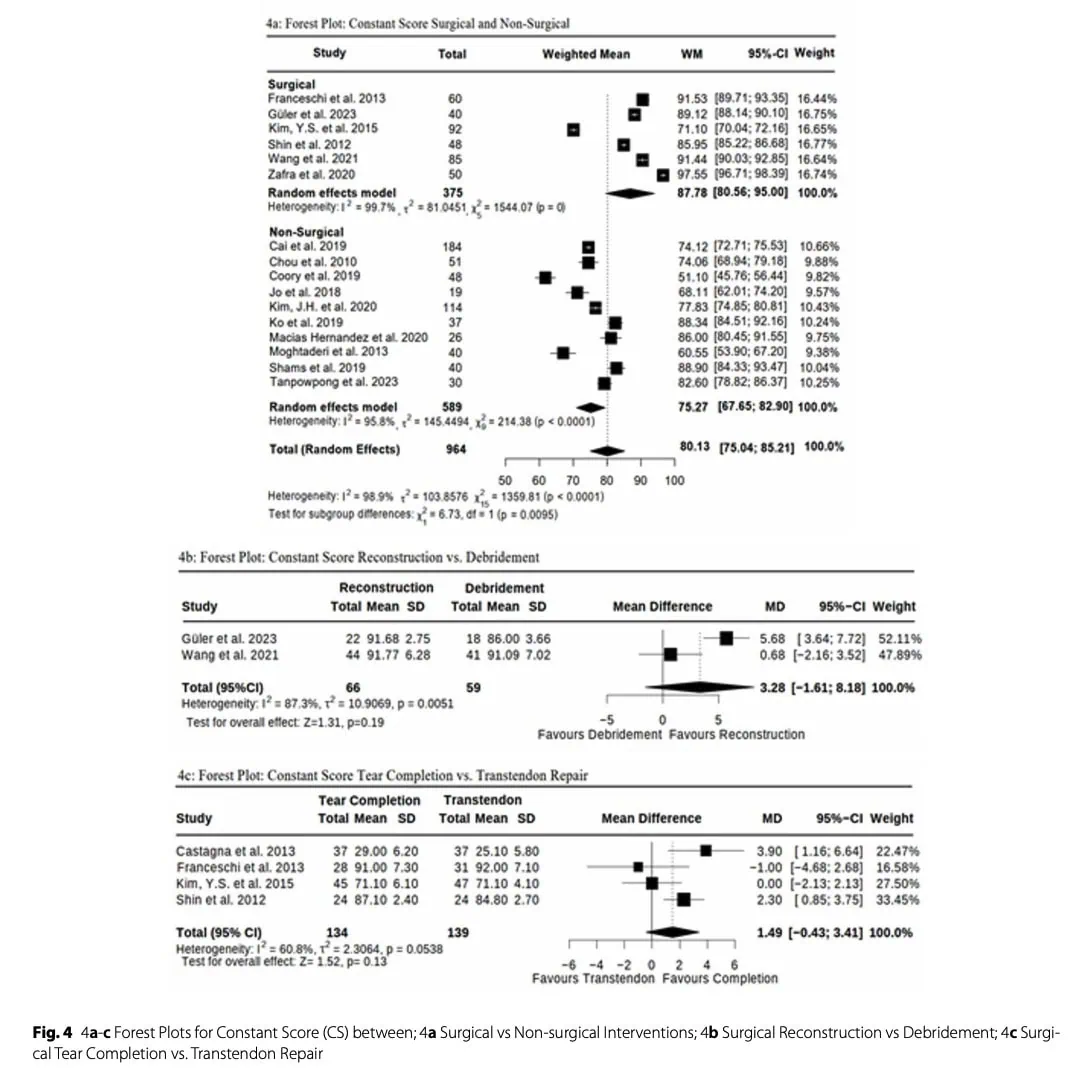
Two studies (n = 125) compared debridement (n = 59) versus reconstruction (n = 66) for partial rotator cuff tears, with follow-up at 18 months. Outcomes included the Constant Score (CS), ASES score, and VAS.
Both studies showed significant within-group improvements from pre- to post-operative assessment. However, results differed across studies in their between-group comparisons. In one of the studies, the reconstruction group demonstrated significantly greater improvements than the debridement group across all outcomes. In contrast, the second one found no statistically significant differences between the two treatment groups.
Transtendon vs tear completion
A transtendon repair preserves the intact part of the tendon and repairs the partial tear in situ. In contrast, a tear completion repair first converts the partial-thickness tear into a full-thickness tear before repairing it. The theoretical advantage of transtendon repair is preservation of the native tendon tissue, while tear completion may provide better visualization and easier access for repair.
This analysis included five studies (n = 342) comparing transtendon repair (n = 170) and tear completion repair (n = 172), most of which were RCTs (Level II evidence), with one Level III study. Outcomes included the Constant Score (CS), ASES score, and VAS, with follow-up ranging from at least six months up to three years.
Across all studies, both surgical techniques led to significant improvements from baseline in all reported outcome measures. However, when comparing transtendon and tear completion approaches, no statistically significant differences were found between the groups.
An additional two studies focusing exclusively on transtendinous repair (n = 85) also showed postoperative improvement, but without statistically significant findings. Overall, both techniques appear similarly effective, with consistent within-group improvements but no clear superiority of one approach over the other for partial rotator cuff tear management.
Non-surgical management
A total of 22 studies, including 1146 patients, investigated non-surgical treatments for partial rotator cuff tears. Most were RCTs (Level II evidence), with one Level III and one Level IV study. For analysis purposes, all non-surgical interventions were grouped into a single category, despite wide variability in treatment types (e.g., injections, physical therapy, shockwave therapy, and biologic treatments). This introduces significant clinical heterogeneity and may limit direct comparisons between individual interventions.
Overall, most studies reported significant within-group improvements in pain and function over time. However, between-group comparisons showed mixed results. Some interventions demonstrated superiority over others or placebo, such as PRP, sodium hyaluronate, nerve blocks, adipose-derived stem cell therapies, and extracorporeal shockwave therapy, which in several studies outperformed corticosteroid injections or sham treatments.
Nevertheless, many studies found no statistically significant differences between treatment groups, highlighting inconsistent evidence across non-surgical modalities. Overall, while non-surgical management generally improves outcomes, no single conservative intervention consistently outperformed others across studies.
Retear as the main complication
Among ten studies on surgical treatment for partial rotator cuff tears, five assessed retear rate as an outcome, most commonly using postoperative imaging with the Sugaya classification.
Overall, retear rates were low (6.3%) across studies. Most analyses showed no statistically significant differences between surgical techniques. However, some patterns emerged: one study reported a higher retear rate in tear completion repair compared to transtendon repair, particularly for bursal-sided tears, while another observed retears only in the tear completion group. Other studies reported either no retears or no significant between-group differences.
Several studies did not report retear rates at all or only mentioned them in the discussion, highlighting inconsistency in reporting. Overall, due to the low number of events, variability in surgical techniques, and heterogeneity in reporting, conclusions regarding differences in retear rates between surgical approaches remain limited.
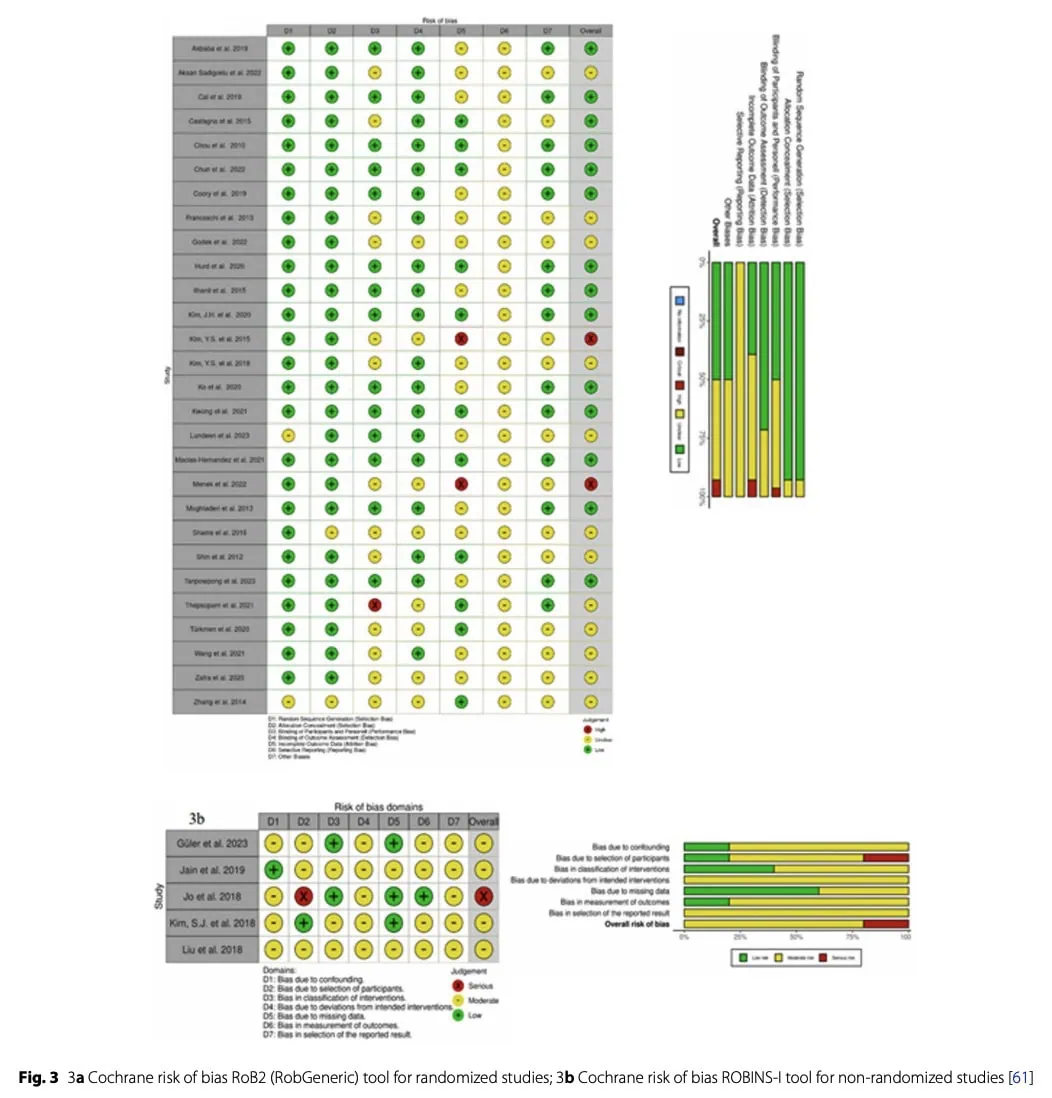
Methodological quality assessment
Risk of bias was assessed using the Cochrane Risk of Bias Tool for both randomized and non-randomized studies. Of the 33 included studies, 28 were RCTs with generally robust randomization procedures, which helped reduce selection bias.
Overall, performance and selection bias were low to moderate, largely due to frequent use of blinding. Attrition and detection bias were also generally well controlled. However, reporting bias was identified as a notable concern across studies.
In summary, the overall methodological quality was mixed, ranging from well-conducted studies with low risk of bias to others with higher risk across multiple domains.
Meta analysis
Due to methodological differences and variability in outcome reporting, only 25 studies were included in the statistical comparison. Some studies were excluded for specific reasons: Two studies due to missing standard deviation values, and one because it lacked an appropriate comparison group.
Additionally, four studies that only reported VAS outcomes were excluded from the statistical analysis, as the focus was on ASES and Constant Score (CS).
Questions and thoughts
The conservative treatment group encompassed a broad spectrum of interventions, including physiotherapy, corticosteroid injections, platelet-rich plasma (PRP), and other non-operative approaches. These modalities differ substantially in their mechanisms of action and in the strength of evidence supporting their use. By grouping them into a single “conservative care” category, the analysis implicitly assumes a level of clinical equivalence that may not reflect real-world practice.
This heterogeneity complicates the interpretation of the findings. A favourable outcome observed within the conservative group may be driven predominantly by one effective intervention, while others contribute minimally or not at all. Conversely, pooling highly effective and less effective treatments may attenuate observable differences between conservative and surgical management. Consequently, the study primarily addresses the broad question of whether surgery is superior to conservative care, but provides limited insight into which specific interventions are most effective.
The Ellman classification categorizes partial-thickness rotator cuff tears according to their depth and location, ranging from low-grade (<3 mm) to high-grade (>6 mm) lesions. Although previous research suggests that tear severity may be associated with symptom burden and treatment response, the reliability and clinical utility of this classification have been questioned. In the present analysis, this factor was not meaningfully accounted for, underscoring the need for future research to better identify which patients are most likely to benefit from surgical versus conservative care for partial rotator cuff tear management. In this context, tear severity classification may represent an important variable for stratifying patients and guiding more individualized treatment pathways.
Talk nerdy to me
This systematic review and meta-analysis combined, or “pooled,” outcome data from multiple studies evaluating either surgical or conservative management of partial-thickness rotator cuff tears. Pooling data in this manner increases statistical power and can provide more precise estimates of treatment effects than individual studies alone. However, because few studies directly compared surgery and conservative care within the same trial, treatment effects were estimated through indirect comparisons across separate patient cohorts. Such analyses are inherently more susceptible to bias, as differences in baseline characteristics, tear severity, and study design may influence outcomes independently of the interventions themselves.
A particularly important limitation is that the pooled comparison between surgical and non-surgical care was based mainly on final follow-up values rather than standardized timepoint-specific comparisons. This means that studies assessing outcomes at different moments in recovery may have been combined, even though treatment effects can change substantially over time. As a result, the conclusion that “surgery is superior to non-surgical care” may overstate the evidence: the apparent advantage may partly reflect differences in follow-up timing, and the observed differences remained below clinically important thresholds.
A notable limitation of the analysis was the considerable statistical heterogeneity reported by the authors. According to the investigators, this heterogeneity likely stemmed from variations in study design, patient demographics, and tear characteristics across the included studies. Such variability makes it difficult to determine whether the observed differences in outcomes truly reflect treatment efficacy or are influenced by differences in the populations being compared.
Interestingly, heterogeneity appears to be particularly pronounced in analyses comparing surgical and conservative approaches. This is likely attributable to the wide range of interventions encompassed within the conservative treatment category. In contrast, heterogeneity was lower in comparisons between surgical techniques, suggesting greater methodological and clinical homogeneity across these studies, and potentially more robust and reliable pooled estimates in this subgroup.
The use of more advanced statistical approaches, such as mixed-effects models incorporating tear severity and other relevant patient characteristics, could potentially have reduced heterogeneity and helped identify subgroups more likely to benefit from either surgical or conservative management.
Take-home messages
- Surgical management shows slightly better outcomes than conservative care, but the differences are generally below clinically important thresholds, suggesting limited real-world superiority.
- Early between-group differences should not automatically be interpreted as true treatment superiority, because at least one comparison showed that a significant difference at six months disappeared by twelve months.
- The statement that surgery is superior to conservative care should be interpreted cautiously, because the pooled analysis relied largely on indirect final-follow-up comparisons across studies with different follow-up durations, and the differences remained below clinically meaningful thresholds
- Conservative management remains a valid first-line approach for partial rotator cuff tear management, with most patients experiencing meaningful improvements in pain and function.
- “Conservative care” is highly heterogeneous (physiotherapy, injections, PRP, etc.), meaning results cannot be attributed to a single intervention.
- Overall conclusions support that partial rotator cuff tears management should not be reduced to a simple “surgery vs rehab” dichotomy.
- Current evidence suggests a need for individualized decision-making, rather than a one-size-fits-all approach.
- Patient factors such as tear severity, symptom profile, and functional limitation are likely key determinants of outcomes, but are not consistently integrated into current evidence.
- The Ellman classification may be relevant for stratification, but its clinical utility and reliability remain limited, highlighting the need for better predictive tools.
- Future research should focus on identifying which patients benefit most from specific conservative or surgical interventions, rather than comparing broad treatment categories.
Reference
Watch two 100% Free Webinars on Shoulder Pain and Ulna-Side Wrist Pain
Improve your Clinical Reasoning for Exercise Prescription in the Active Person with Shoulder pain with Andrew Cuff and Navigate Clinical Diagnosis & Management featuring a Case Study of Golfer with Thomas Mitchell