
Research
Diagnosis & Imaging
May 17, 2026
Associations between Muscle Morphology and Lumbopelvic Control in Unilateral Lumbar Spondylolysis? A Study of Adolescent Soccer Players

Introduction
Back pain in young people who play sports should prompt you to look into the matter more closely, rather than simply assuming it is just a case of temporary growing pains, as adolescent athletes are at risk for significant structural injuries. It has been observed that adolescent athletes presenting with low back pain are more likely to have structural injuries like spondylolysis. Spondylolysis is a stress reaction or fracture of the pars interarticularis of the lumbar vertebrae. It is a type of specific low back pain commonly seen in young active adolescents participating in sports involving many (hyper)extension and rotational movements. In this research review, we dive a little deeper into recognizing spondylolysis and linking it to clinical tests of lumbopelvic control commonly used in practice.
Methods
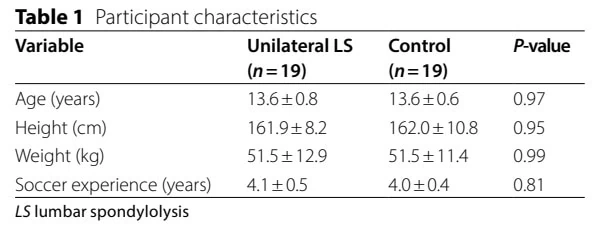
This was a cross-sectional observational study involving adolescent male soccer players from the same competitive academy environment. The investigators screened male soccer players aged 12–14 years using MRI. Affected athletes were matched with controls using propensity score matching based on age, height, and weight. All players were recruited from the same club, played 2–3 hours/session, and 5 days per week after school and on weekends.
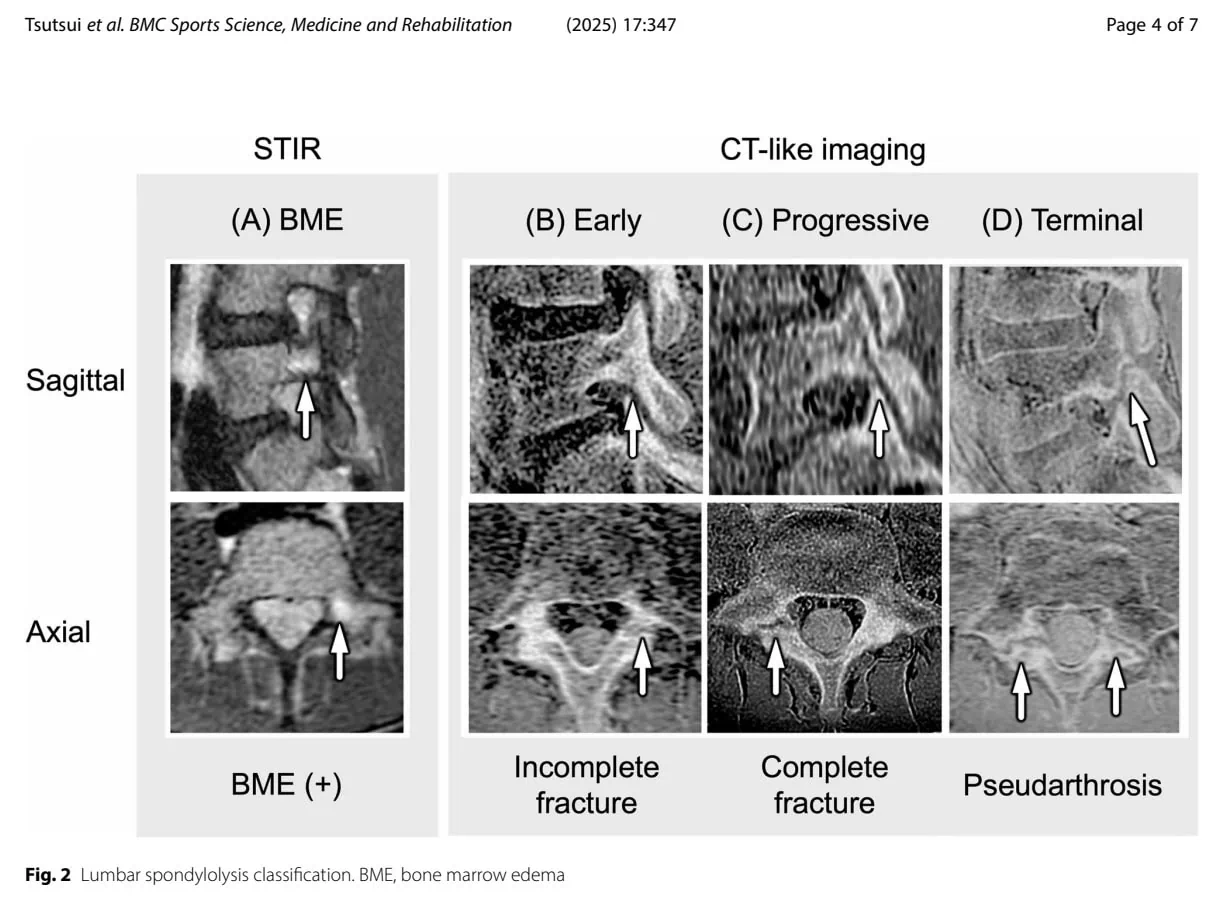
MRI was performed using a 3.0 Tesla scanner, and two imaging sequences were used: STIR imaging for bone marrow edema, and 3D LAVA imaging for fracture staging.
The study classified lumbar spondylolysis into:
- bone marrow edema only,
- early-stage hairline fracture,
- progressive fracture,
- terminal pseudoarthrosis.
Only athletes with unilateral findings were included in the study group.
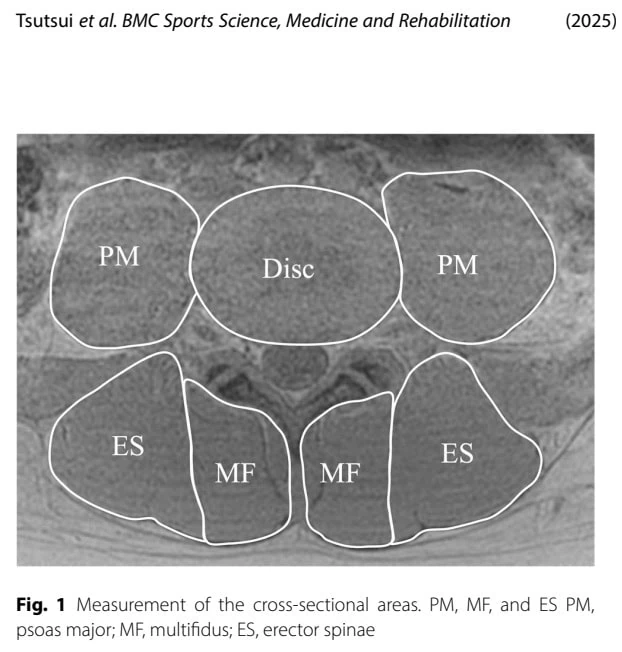
Regarding muscle morphology, the researchers measured MRI-derived cross-sectional area (CSA) at the L4/L5 level for the psoas major (PM), multifidus (MF), and erector spinae (ES) muscles. Measurements were taken bilaterally.
Two clinical lumbopelvic control tests were used:
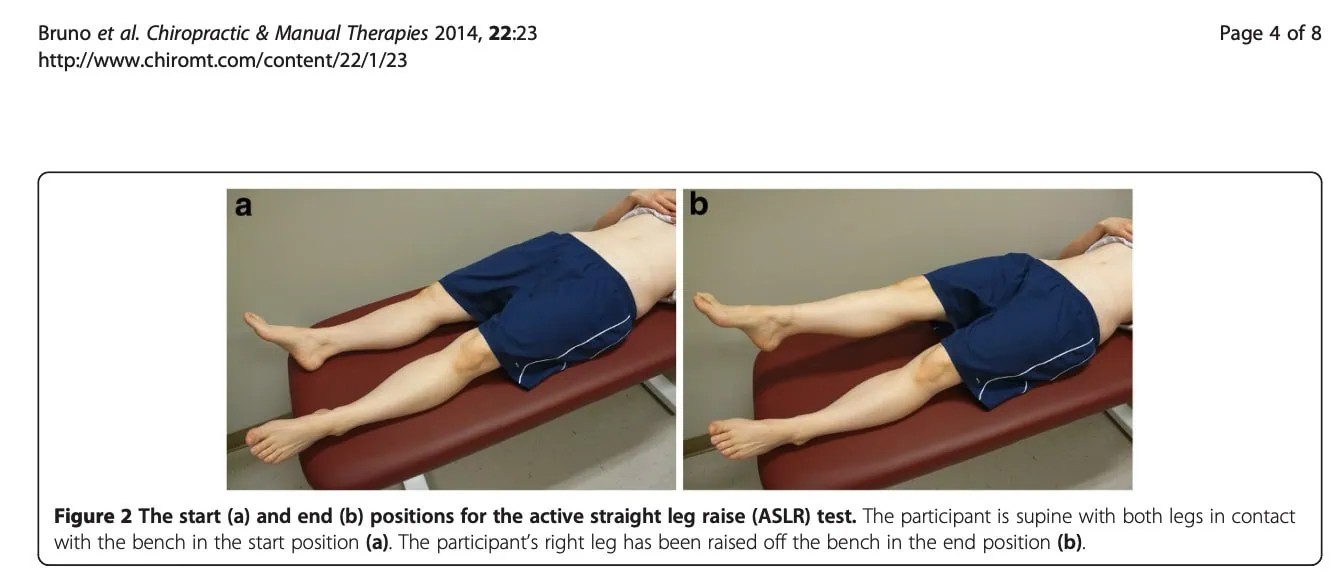
1. Active Straight Leg Raise (ASLR)
With the athlete in a supine position with both legs straight and relaxed, the athlete raised one leg with the knee extended to approximately 30° of hip flexion while the examiner palpated the anterior superior iliac spine (ASIS) for pelvic depression/rotation. A positive test indicated visible or palpable pelvic depression/rotation on the side of the moving limb. In this study, pelvic depression referred to an observable downward displacement or rotational drop of the pelvis in the horizontal plane. For example, during a right-leg raise, excessive rotation or depression of the right pelvis was considered abnormal.
This test was performed a little differently than the ASLR for pelvic girdle pain or sacroiliac joint pain; however, the following video might be useful.
The test outcome was scored as:
- Positive = visible/palpable loss of lumbopelvic control (pelvic depression/rotation),
- Negative = stable pelvic control during the movement.
https://pubmed.ncbi.nlm.nih.gov/24982755/
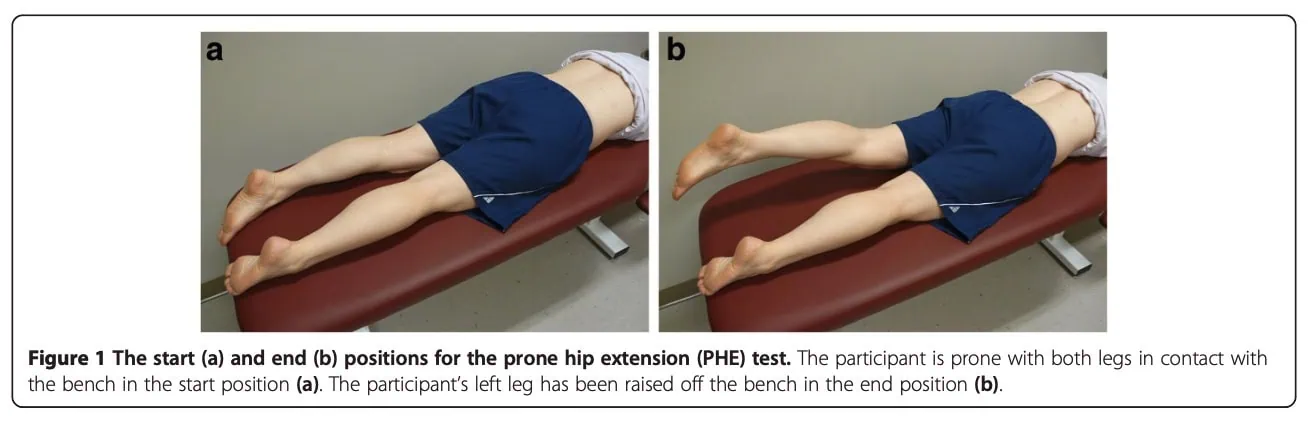
2. Hip Extension (HE) Test
Performed prone, the athlete actively raised his hip to approximately 15° of hip extension while monitoring pelvic control. The examiner observed for excessive pelvic depression or rotation occurring as the limb was lifted. For example, during right hip extension, excessive rotation or dropping of the left side of the pelvis was considered a positive finding, reflecting impaired lumbopelvic stability.
The examiner again classified the test as:
- Positive = loss of pelvic stability/control,
- Negative = controlled movement without pelvic displacement.
https://pubmed.ncbi.nlm.nih.gov/24982755/
Results
A total of 107 male soccer players from the same competitive club were enrolled in the study. Of these, MRIs revealed unilateral lumbar spondylolysis in 19 players. The 19 affected individuals were included in the study and matched to 19 controls, and no significant difference appeared between the two groups.
Of the 19 players who had unilateral lumbar spondylolysis, 15 had their non-dominant side affected, and 4 had their dominant side affected. Four players had bone marrow edema, 12 were in the early stage, and 3 were in the progressive stage of spondylolysis.
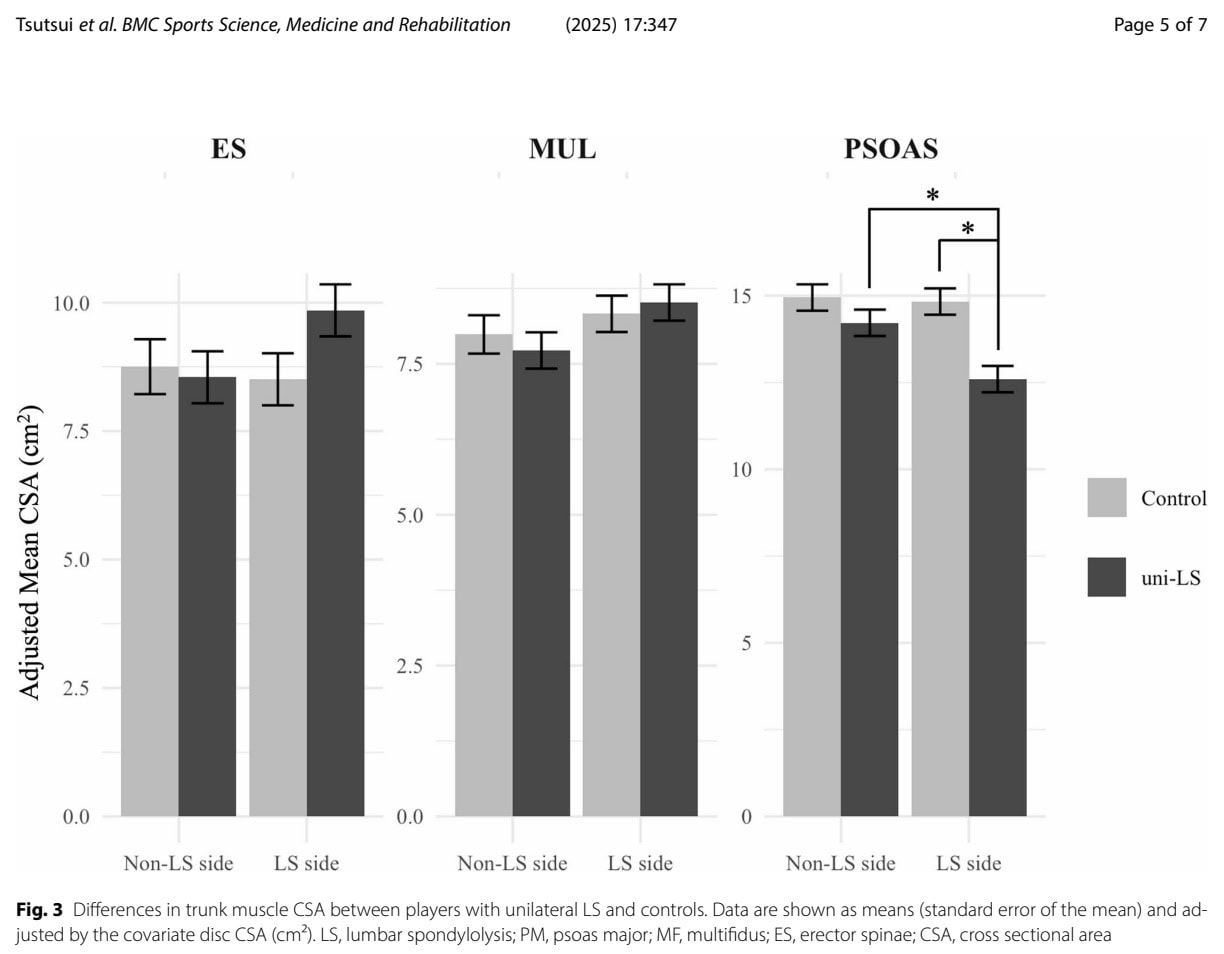
The analysis of players with unilateral lumbar spondylolysis and control players revealed differences in the cross-sectional area of the Psoas Major muscle on the affected side. This was observed by a significant main effect of group and an interaction effect.
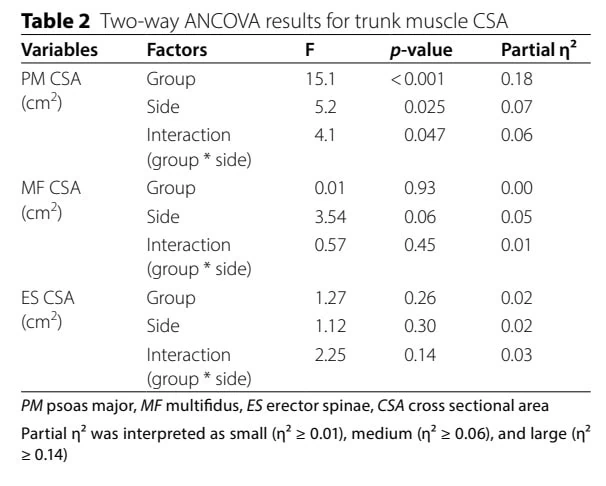
The significance of the main group effect means that the players with unilateral lumbar spondylolysis had different psoas major muscle sizes compared to the healthy controls. When both sides were compared, the unilateral lumbar spondylolysis group generally had smaller Psoas Major muscles. The interaction effect is more specific and clinically interesting: it means the difference between the left and right sides was not the same in both groups. In the unilateral lumbar spondylolysis players, the Psoas Major muscle was especially smaller on the injured side, whereas the control players did not show this asymmetry. So, the interaction effect suggests that the muscle difference is linked specifically to the side of the lumbar injury, rather than just being a general characteristic of soccer players.
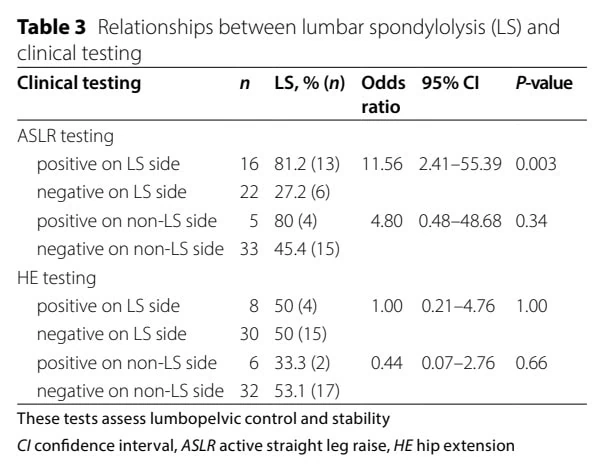
When the associations between the presence of unilateral lumbar spondylolysis and clinical test results were investigated, it revealed that 81% of the players who tested positive on the ASLR on the side of the injury belonged to the spondylolysis group.
Questions and thoughts
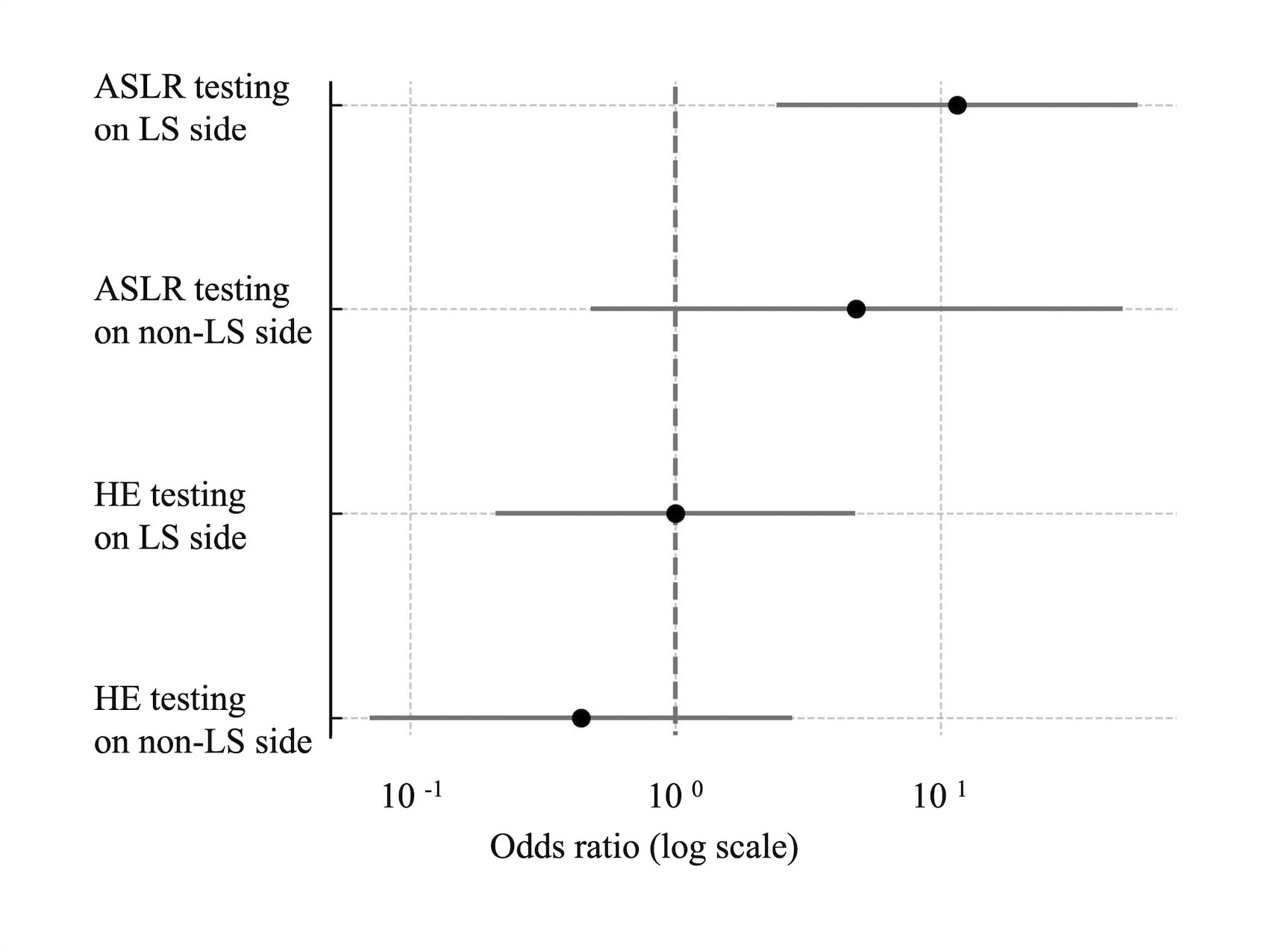
The forest plot shows the relationship between positive clinical tests and the presence of unilateral lumbar spondylolysis. The black dots represent the odds ratios (ORs), while the horizontal lines represent the 95% confidence intervals. The dashed vertical line 10^0 equals OR = 1 and means no relationship. If the confidence interval crosses this line, the finding is not statistically significant.
The strongest finding is the ASLR testing on the unilateral spondylolysis side. The odds ratio is exceeding 11, indicating that players with a positive ASLR on the injured side were more than 11 times as likely to have unilateral lumbar spondylolysis as controls. Importantly, the confidence interval does not include 1, indicating a statistically significant result. Clinically, this suggests that poor lumbopelvic control during ASLR is strongly associated with unilateral lumbar spondylolysis.
The ASLR on the non-affected side also trends toward higher odds (OR 4.8), but the confidence interval crosses 1, which means the relationship may simply be due to chance, so we cannot confidently say there is a true association.
For the hip extension (HE) tests, both the spondylolysis and the non-affected sides have confidence intervals crossing 1. This indicates no significant relationship between hip extension test findings and lumbar spondylolysis in this sample. So, hip extension testing did not meaningfully distinguish players with unilateral lumbar spondylolysis from healthy players.
What happens during the ASLR test? According to the EMG study by Hu et al. (2012) in healthy subjects, this is what is happening:
“Hip flexion causes an unwanted forward pull on the ipsilateral ilium, which is counteracted by contralateral BF activity. To transfer this contralateral force toward the ipsilateral, the lateral abdominal muscles press the ilia against the sacrum (“force closure”). Thus, problems with the ASLR may derive from problems with force closure. Also, abdominal wall activity counteracts the forward rotation of the ilium. Moreover, contralateral Biceps Femoris activity causes transverse plane rotation of the pelvis, often visible as an upward movement of the contralateral anterior superior iliac spine. Such transverse plane rotation is countered by the ipsilateral Transversus Abdominis and Obliquus Abdominis Internus.”
So, in healthy individuals, the ASLR requires efficient force closure of the pelvis and coordinated transfer of load between the trunk and lower limbs. During hip flexion, the ilium on the moving side tends to rotate anteriorly and translate forward. Normally, this is stabilized through:
- contralateral biceps femoris tension,
- compression of the SIJ/pelvis by the abdominal wall,
- and anti-rotational control from the ipsilateral deep abdominal muscles (especially Transversus Abdominis and Internal Oblique).
In the players with unilateral lumbar spondylolysis, a positive ASLR likely reflects a failure of this rotational load-transfer system. If force closure and anti-rotation control are insufficient:
- The pelvis may excessively rotate or depress,
- Lumbar rotation may increase,
- Mechanical stress through the pars interarticularis may rise.
Because spondylolysis is strongly associated with repeated lumbar extension combined with rotation, a reduced ability to control transverse-plane motion during ASLR may therefore reflect the same deficient rotational control strategy that contributes to repetitive pars loading during soccer activities such as kicking, pivoting, cutting, and acceleration.
The smaller psoas major on the lumbar spondylolysis side may further contribute to this problem. The psoas major muscle assists not only with hip flexion, but also with lumbar segmental stabilization and rotational control. If the psoas major muscle provides less stiffness or stabilization on the injured side, the athlete may rely on compensatory pelvic rotation during limb movement, making the ASLR appear positive. Furthermore, Wagner et al. (2018) found that the iliopsoas cross-sectional area differentiates mild-to-moderate from severe degenerative spondylolysthesis. This strengthens the observed association between the smaller cross-sectional area of the psoas major muscle on the affected side in the unilateral spondylolysis-affected players, as spondylolysis is a precursor of spondylolisthesis.
Clinically, the positive ASLR in these athletes may therefore indicate:
- impaired force closure,
- deficient anti-rotation control,
- altered trunk–pelvis load transfer,
- and increased rotational stress exposure at the pars interarticularis.
These aspects could be trained in your clinic.
Talk nerdy to me
A very important aspect to bear in mind is the cross-sectional nature of this research. This implies that the measurements were obtained at one specific moment in time. Because this was a cross-sectional study, the findings cannot establish cause-and-effect relationships. We do not know whether reduced psoas major muscle size and impaired ASLR performance contributed to the development of unilateral lumbar spondylolysis, or whether they developed as adaptations after the injury occurred. Additionally, although the authors matched participants for several characteristics, other important confounding variables, such as training load, playing position, maturation status, and previous injury history, were not fully controlled and may have influenced the results.
The fact that all players were recruited in the same club may limit generalizability to other clubs and formation academies. Nonetheless, it is important because it reduces variability in training exposure across the individuals included.
Strengths of this study included the use of high-definition MRI, conducted with a 3.0 Tesla scanner. The use of such high-resolution technology represents a significant methodological strength, as it enhances the sensitivity required to detect early-stage bone marrow edema and stress injuries.
To normalize for individual variations in body size during the muscle morphology analysis, the researchers utilized the cross-sectional area (CSA) of the vertebral disc as a covariate. Furthermore, the measurement process demonstrated robust intrarater reliability, with intraclass correlation coefficients (ICC) ranging from 0.82 to 0.89. This level of reliability is clinically vital, ensuring that observed side-to-side asymmetries are likely representative of true morphological changes rather than mere measurement error.
An additional noteworthy methodological strength of this study was that the examining physiotherapist was blinded to the MRI results during clinical testing.
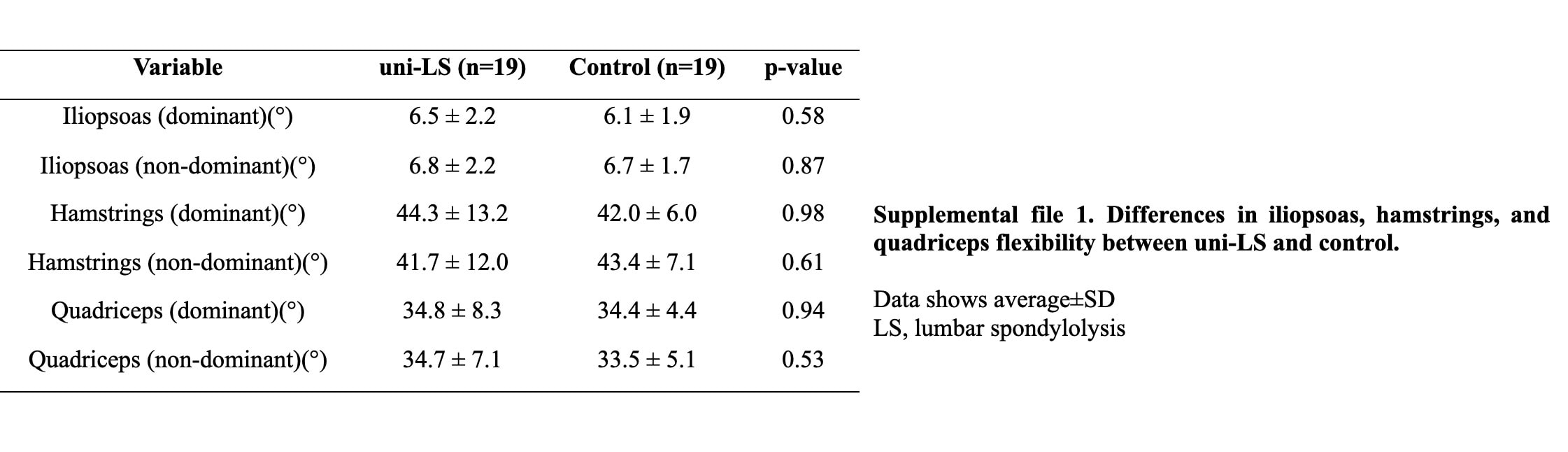
The authors screened for participants with sufficient mobility before they were enrolled in the study. They also ensured to evaluate the passive flexibility of the iliopsoas, hamstrings, and quadriceps muscles, which may influence the clinical tests. It revealed no significant differences between the adolescents affected by unilateral lumbar spondylolysis and the controls.
Take-home messages
A positive ASLR in an adolescent soccer player may warrant further screening for lumbar spondylolysis, especially when combined with other clinical indicators such as extension-related low back pain, unilateral symptoms, reduced rotation control, or a history of repetitive loading. Since the study found a strong association between positive ASLR findings and unilateral lumbar spondylolysis, the ASLR may serve as a practical clinical screening tool to help identify athletes who could benefit from further imaging evaluation. However, ASLR alone is not diagnostic and should be interpreted within the broader clinical picture.
Also, the findings suggest that rehabilitation targeting both lumbopelvic control and the psoas major may be relevant in athletes with unilateral lumbar spondylolysis. The injured side demonstrated a smaller psoas major muscle cross-sectional area alongside impaired ASLR performance, which may indicate altered stabilizing function around the lumbar spine. Although causality cannot be established from this study, incorporating side-specific psoas strengthening, anti-rotation control exercises, and lumbopelvic stability training appears clinically justifiable until further interventional research becomes available.
A key limitation of this study is the cross-sectional design, meaning that these findings should be interpreted as associations rather than causal mechanisms. While the authors controlled for several variables, unmeasured confounders may partly explain the observed differences in psoas morphology and lumbopelvic control.
The study’s moderate statistical power (0.67) represents an important limitation. Because the sample size was relatively small, the study may have been underpowered to detect smaller but clinically relevant differences, particularly for the multifidus and erector spinae muscles. Therefore, the findings should be interpreted cautiously and considered exploratory until replicated in larger cohorts.
Learn more
Reference
MASSIVELY IMPROVE YOUR KNOWLEDGE ABOUT LOW BACK PAIN FOR FREE
5 absolutely crucial lessons you won’t learn at university that will improve your care for patients with low back pain immediately without paying a single cent
