Research
Exercise
March 13, 2025
Manual Therapy and Exercise on Brain Adaptations in Neck Pain

Introduction
Chronic nonspecific neck pain is a prevalent condition that leads to significant disability and increased healthcare costs. While traditional physical therapy approaches, such as range of motion exercises and passive modalities, are commonly used, emerging evidence suggests that manual therapy combined with therapeutic exercise may offer superior outcomes. However, the underlying brain adaptations in neck pain associated with these interventions remain underexplored.
Chronic pain is widely recognized as being linked to maladaptations in the central nervous system (CNS), contributing to persistent pain and dysfunction. Manual therapy has been shown to modulate pain through neurophysiological effects, while therapeutic exercise may help desensitize the CNS. Understanding how these treatments influence brain adaptations in neck pain and pain processing, is essential for optimizing rehabilitation strategies and improving patient outcomes.
Study Objectives
This randomized controlled trial aimed to:
- Investigate how manual therapy combined with exercise influences brain adaptations in neck pain patients (e.g. cortical thickness and volume) compared to routine physical therapy.
- Assess clinical improvements in pain, disability, psychological symptoms, cervical mobility, and muscle strength.
- Explore brain structure differences between patients with significant pain relief (≥50% reduction) and those with minimal improvement.
- Examine potential correlations between brain changes and clinical outcomes.
It was hypothesized that manual therapy combined with exercise would more effectively alter pain-related brain regions than routine physical therapy, leading to greater clinical improvements.
Methods
This study used a parallel single-blinded randomized controlled trial design.
Participants
Adults (18–59 years) with chronic nonspecific neck pain (≥ 3 months, VAS ≥ 35 mm on a 100 mm VAS) were recruited via hospitals, clinics, and social media. Exclusion criteria included prior neck injury/surgery, neurological or musculoskeletal disorders, metabolic conditions, psychiatric disorders, BMI ≥ 25, MRI contraindications, or physiotherapy in the past year.
Randomization & Blinding
Participants were randomly assigned (1:1) to either an intervention or control group using computer-generated sequences, stratified by age and gender. Independent assessors and MRI analysts were blinded to group allocation.


Interventions
Intervention group: Participants received cervical mobilization and a progressive exercise program targeting neck, shoulder muscles, posture, and function. Manual therapy focused on the most symptomatic cervical segment, determined by the physiotherapist’s assessment. Exercises included cervical flexor/extensor training, axioscapular strengthening, and postural corrections, with progression in repetitions, direction, and load. Sessions occurred twice weekly (30–40 minutes) for 10 weeks, with daily home exercises recorded in a diary. To ensure consistency, physiotherapists underwent a three-day training.
Control group: Received routine physical therapy (modalities, cervical ROM exercises, stretching) twice weekly for 10 weeks.
Outcome Measures
Primary Outcome: Brain structure changes (cortical thickness & volume) assessed via MRI (FreeSurfer analysis). This method automatically identified and mapped different brain structures using two well-established brain atlases (Desikan-Killiany and Destrieux).
Based on previous research, they focused on specific brain regions, including bilaterally:
- Primary motor cortex (M1) – involved in movement control
- Insula – linked to pain perception and emotional processing
- Prefrontal cortex (PFC) – plays a role in decision-making and pain regulation
- Anterior cingulate cortex (ACC) – involved in pain processing and emotional responses
- Precuneus – associated with self-awareness and cognitive functions
- Primary somatosensory cortex (S1) – processes sensory information like touch and pain
- Thalamus – a key relay center for sensory and pain signals
Secondary Outcomes: The study measured different aspects of neck pain and function using the following methods:
Neck Pain Intensity: Measured with a 0–100 mm Visual Analog Scale (VAS), where 0 = no pain and 100 = worst pain imaginable.
Neck Disability: Assessed using the Thai version of the Neck Disability Index (NDI), with higher scores indicating more disability.
Anxiety & Depression: Evaluated with the Thai version of the Hospital Anxiety and Depression Scale (HADS), where higher scores mean worse symptoms.
Cervical Range of Motion (ROM): Measured in all directions (flexion, extension, lateral flexion, and rotation) using a CROM goniometer. Each movement was recorded three times, and the average was used.
Cervical Muscle Strength: Tested with a handheld dynamometer, measuring cranio-cervical muscle strength three times, with the highest value recorded.
Statistical Analysis
Descriptive statistics were used to summarize participant demographics and baseline/post-treatment data.
Brain structure analysis: Differences in cortical volume and thickness were assessed with FreeSurfer software, using corrections for multiple comparisons (FDR and TFCE methods), with statistical significance set at p < 0.05.
Group comparisons:
- ANCOVA (adjusted for baseline values) tested differences between groups in brain regions of interest (ROIs) and other outcomes.
- General linear mixed model analyzed changes within each group.
- Effect sizes were reported using partial eta squared (η²p), with thresholds of 0.01 (small), 0.06 (moderate), and 0.14 (large).
Responder analysis: Participants with ≥ 50% pain reduction were classified as responders, and those with < 50% reduction as non-responders. Brain changes were compared between these groups using the Mann-Whitney U test.
Correlations: Relationships between brain changes and clinical characteristics (pain, disability, psychological symptoms) were analyzed using Pearson’s correlation.
Further details on the statistical methods used in this study can be found in the “Talk nerdy to me” section.
Results
Participants and Interventions
The study ran from November 2022 to February 2024, enrolling 52 participants from 367 volunteers, with no loss to follow-up.
Intervention group: Completed 20 sessions over 10 weeks (one participant completed 19 sessions). Over 80% adherence to home exercises, and no additional treatments reported.
Control group: Received routine physical therapy. Three participants (11.54%) used NSAIDs, and two (7.69%) received massages. No significant adverse events occurred.
Primary Outcomes
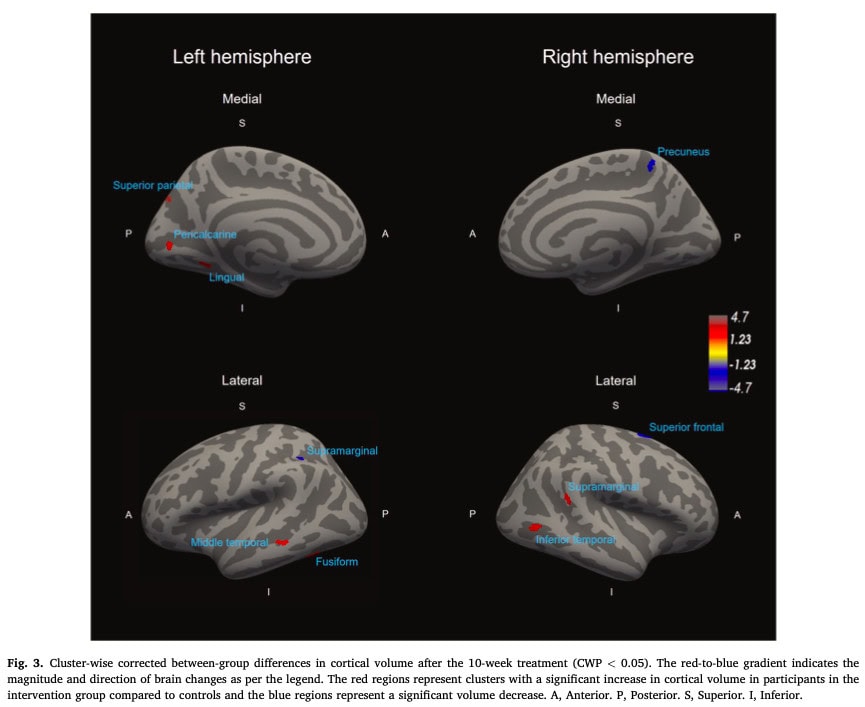
Brain structure changes :
Intervention group: Increased cortical thickness and volume in some brain areas compared to controls (except for specific regions with decreases).
Regions of Interest (ROIs) Analysis:
- Increased thickness in both ACC hemispheres.
- Decreased thickness in left PFC, left/right S1, and left/right precuneus.
- Control group showed cortical thinning in left S1, left M1, and right precuneus.
- No significant changes in cortical volume in either group.
ANCOVA analysis: Intervention group showed greater cortical thickening in left/right ACC and left M1 compared to controls.



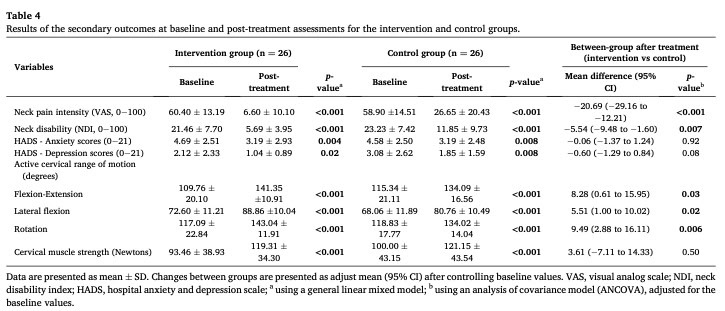
Secondary Outcomes
Both groups showed improvements in neck pain intensity, neck disability, psychological symptoms, cervical ROM, and muscle strength. (p < 0.05, η2p = 0.10 – 0.84).
The ANCOVA analysis showed that the intervention group had significantly greater improvements in neck pain intensity, disability, and cervical range of motion (all directions) compared to the control group (p < 0.05), with effect sizes (η2p) ranging from moderate to large (0.09 to 0.33).
No significant differences between groups in psychological symptoms (anxiety/depression) or cervical muscle strength. (p > 0.05).
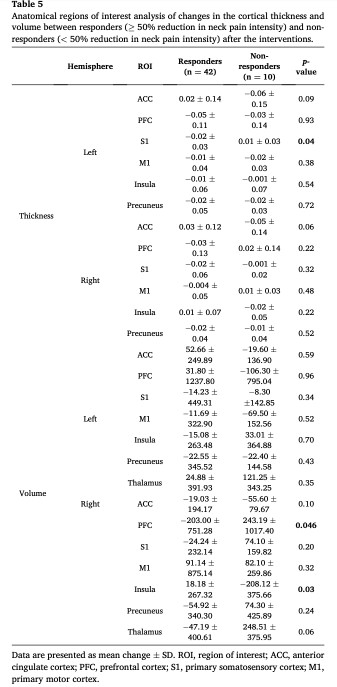
Brain Changes and clinical improvement in neck pain intensity
80.77% (42 participants) had ≥50% improvement in pain intensity (25 intervention vs. 17 control). More responders in the intervention group (p = 0.01).
Responders ( ≥50% improvement in pain intensity) showed:
Decreased left S1 thickness & right PFC volume.Increased right insular volume.Non-responders (<50% improvement in pain intensity) showed:
Increased left S1 thickness & right PFC volume.Decreased right insular volume.Pain intensity reduction was negatively correlated with cortical thickness in left ACC, PFC, M1 and volume in left S1, left M1, right insular.
Disability reduction correlated with right thalamus volume changes.
No correlation between psychological changes and brain structure changes.
Key findings
- The intervention led to significant brain structure changes and better clinical outcomes (pain reduction, function improvement).
- Greater cortical thickening in key regions correlated with pain processing.
- Responders had distinct brain structure changes compared to non-responders.
- Neck pain and disability improvements were linked to specific brain changes, but psychological improvements were not.
Questions and Thoughts
Pain assessment is inherently complex due to its subjective nature. According to the Toussignant-Laflamme pain model, pain is multifactorial, influenced by a combination of biological, psychological, social, and environmental factors. However, the study relies heavily on the Visual Analog Scale (VAS) for pain measurement, which is highly subjective and may not fully capture the complexity of pain. The proposed classification of patients into those with <50% or >50% pain reduction oversimplifies the pain experience and may not adequately reflect the diverse drivers of pain.
The Toussignant-Laflamme model emphasizes that environmental, contextual, and cognitive factors play significant roles in pain perception, yet these factors were poorly assessed in this study. For example, factors such as patient beliefs, social context, and environmental stressors could have influenced outcomes but were not systematically evaluated. Psychological or psychosocial factors, often referred to as “yellow flags” (e.g., fear of movement, anxiety, or depression), are known to influence pain perception and recovery but were not adequately explored. This lack of consideration for confounding variables limits the study’s ability to fully explain the mechanisms behind pain relief or treatment responsiveness.
Additionally, for patients suffering from chronic pain, central sensitization is a well-known mechanism that perpetuates pain. Central sensitization involves heightened sensitivity of the central nervous system to pain signals, often leading to amplified pain responses. Including an assessment of central sensitization, such as the Central Sensitization Inventory (CSI), would have provided valuable clinical insights into its potential correlation with structural brain changes.
Talk nerdy to me
The study employed a robust statistical framework to analyze structural brain changes and their relationship with clinical symptoms. Researchers measured cortical thickness and brain volume across thousands of voxels (small 3D units used in brain imagery), applying False Discovery Rate (FDR) correction to control the proportion of false positives. FDR ranks p-values and adjusts the significance threshold, ensuring a low rate of false positives while maintaining sensitivity. To enhance detection of spatially extended effects, Threshold-Free Cluster Enhancement (TFCE) was used, which identifies clusters of voxels without requiring arbitrary thresholds, refining the results by focusing on meaningful patterns in the data. For additional rigor, Family-Wise Error (FWE) correction was applied, ensuring a very low probability of any false positives across the entire dataset. This combination of methods (FDR, TFCE, and FWE) provided high confidence in the findings.
Between-group differences in brain structure and secondary outcomes (e.g., pain intensity, range of motion) were analyzed using Analysis of Covariance (ANCOVA), with baseline values as covariates. Changes within groups over time were assessed using a General Linear Mixed Model (GLMM), which accounted for repeated measurements. The magnitude of intervention effects was quantified using Partial Eta Squared (η2ₚ), with thresholds for small (0.01), moderate (0.06), and large effects (0.14+). Participants were classified as responders (≥50% pain reduction) or non-responders, and Mann-Whitney U tests compared brain structure changes between these groups. Finally, Pearson’s correlation coefficients were used to examine associations between structural brain changes and clinical outcomes (e.g., pain intensity, disability, psychological symptoms).
While the statistical methods were rigorous, it’s important to note that the study only explored correlations, not causation. Further research is needed to investigate the mechanisms underlying central nervous system (CNS) adaptations resulting from manual therapy and specific exercise interventions.
Take home messages
Brain Structure and Pain – Alterations in cortical thickness and volume were linked to changes in pain intensity and disability, suggesting that central mechanisms contribute to musculoskeletal pain.
Responder vs. Non-Responder Differences – Patients who achieved significant pain reduction (≥50%) also displayed distinct brain structure changes, reinforcing the idea that effective rehabilitation extends beyond physical improvements.
Optimizing Treatment Approach – The study suggests that combining manual therapy and exercise is more effective for nonspecific chronic neck pain than conventional physiotherapy. The Maitland manual therapy framework provides a solid starting point, while exercise prescription should be individualized based on a thorough patient evaluation.
Comprehensive Patient Assessment – Therapists should assess psychosocial contributors to pain (yellow flags) using tools such as the StarT Back Questionnaire, the Tampa Scale for Kinesiophobia, or the Pain Catastrophizing Scale. Additionally, considering environmental factors during the subjective evaluation may help refine treatment strategies.
Reference
5 ESSENTIAL MOBILIZATION / MANIPULATION TECHNIQUES EVERY PHYSIO SHOULD MASTER
Learn 5 essential mobilization / manipulation techniques in 5 days that will skyrocket your manual therapy skills immediately – 100% For Free!