
Research
Knee
May 26, 2026
Beyond the Clinic: Do Physiotherapy Clinic-Based ACLR Return-to-Sport Test Batteries Capture Full Readiness? A Comparison with the Gold Standard

Introduction
Although widely supported and recommended, a recent survey of physiotherapists concluded that return-to-sport testing is not regularly performed in clinical settings. One of the reasons, therefore, is the lack of equipment available. This is a problematic finding, as passing a return-to-sport test battery consisting of strength, performance-based metrics, and self-reported knee function is associated with reduced anterior cruciate ligament reinjury risk and improved return-to-sport rates. The authors of the current study highlighted that one of the barriers to this discrepancy is the reported use of specialized equipment like expensive isokinetic dynamometers, which are unavailable in physiotherapy practice. To overcome this barrier, several attempts have been made to construct physiotherapy-approved return-to-sport assessments that are applicable for use and effectively implemented in real-life. But to support their use, we must be certain that the clinic-based return-to-sport test batteries are valid when compared to the gold standard examinations. Therefore, this study examined how a clinic-based return-to-sport testing battery performed against a gold standard and whether residual strength or biomechanical deficits remained in those passing the test battery.
Methods
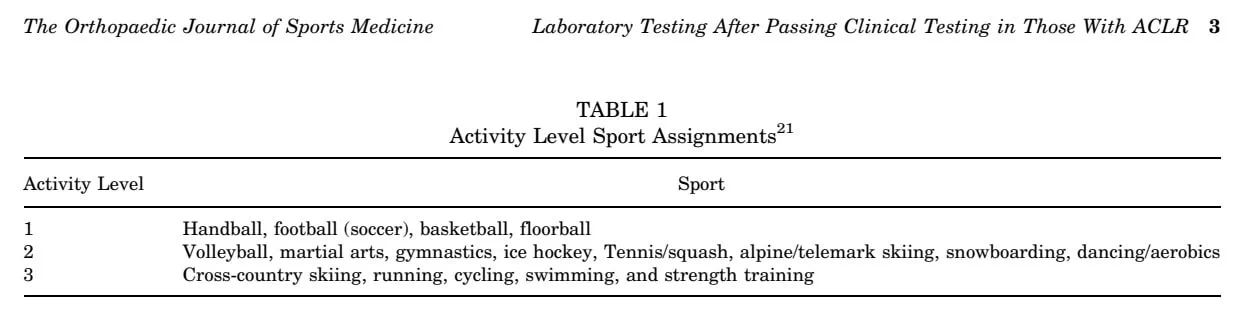
This was a cross-sectional study involving athletes aged 10-25 years who had undergone unilateral ACL reconstruction (ACLR) within the previous 5-15 months. The participants intended to return to cutting-and-pivoting sports (level 1 or 2 sports such as soccer, basketball, volleyball, gymnastics, hockey, martial arts, etc.).
Patients were excluded if they had previous surgery to either knee, multiligament reconstruction, and/or significant additional surgical procedures.
The patients were invited to the clinic-based return-to-sport test battery when either their physiotherapist or the surgeon determined that they were physically capable of performing the tests. The test battery was intentionally designed to be realistic and accessible for physiotherapy clinics. Participants had to pass ALL of the following:
- ≥90% limb symmetry index (LSI) for:
- Isometric quadriceps strength: The clinic-based isometric quadriceps test was designed as a simple, low-cost alternative to laboratory dynamometry. Participants sat in a knee extension machine with the hip flexed to about 80° and the knee fixed at 90° flexion. The chest and thigh were strapped down, while a crane scale attached to the machine arm measured force during a maximal isometric knee extension effort. Participants completed three warm-up efforts followed by three maximal 5-second contractions, with the highest force value recorded.
- 1RM knee extension strength (isotonic): The clinic-based isotonic test used the same knee extension machine setup but assessed dynamic strength through a 1-repetition maximum (1RM) knee extension. Participants extended the knee from 90° flexion to full extension while resistance was progressively increased until they could no longer complete a successful repetition through the full range of motion. The heaviest successful repetition was recorded.
- Single hop
- Triple hop
- Crossover hop
- 6-meter timed hop
- ≥90% score on:
- IKDC
- Global Rating Scale (GRS)
If athletes failed, they received additional rehabilitation and were retested 4-6 weeks later. When they passed, they proceeded to the laboratory testing within two weeks.
Laboratory Testing
Isometric Quadriceps Testing
In the laboratory, participants were tested using a Biodex isokinetic dynamometer. They sat upright with the hips flexed to 90° while straps stabilized the trunk, pelvis, and thigh. For isometric testing, the knee was fixed at 90° flexion, and participants performed maximal contractions while being instructed to kick “as hard and fast as possible,” allowing the researchers to assess both maximal torque and rate of torque development (RTD).
Isotonic Quadriceps Testing
The laboratory isotonic testing used the same setup, but the dynamometer controlled knee movement at a constant speed of 60°/second. Participants completed five maximal repetitions of knee extension and flexion, allowing the researchers to measure quadriceps and hamstring torque under standardized conditions.
Drop Jump Testing
Participants performed bilateral and unilateral drop vertical jump tasks while their movement patterns were analyzed using a 3D motion capture system with force plates. Sixteen motion-capture cameras and two force plates were used to track the movements of the reflective markers placed on the participants. They performed bilateral drop vertical jumps (BDVJ) and unilateral drop vertical jumps (UDVJ), and from this data, the researchers analyzed:
- Knee flexion moments (KFM)
- Ground reaction forces (GRF)
- Knee extension power (KEP)
- Jump height
- Reactive strength index (RSI)
Results
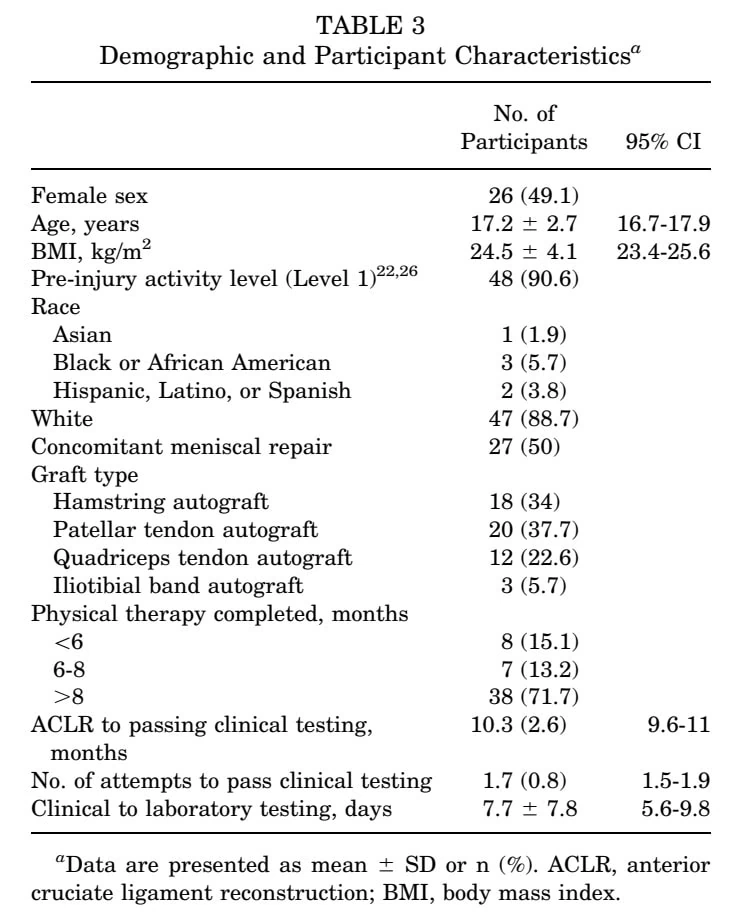
A total of 69 athletes were enrolled, but only 53 successfully passed the clinic-based RTS battery and proceeded to laboratory testing. The average participant was 17 years old, had undergone ACLR 10 months ago, and had completed more than 8 months of physical therapy.
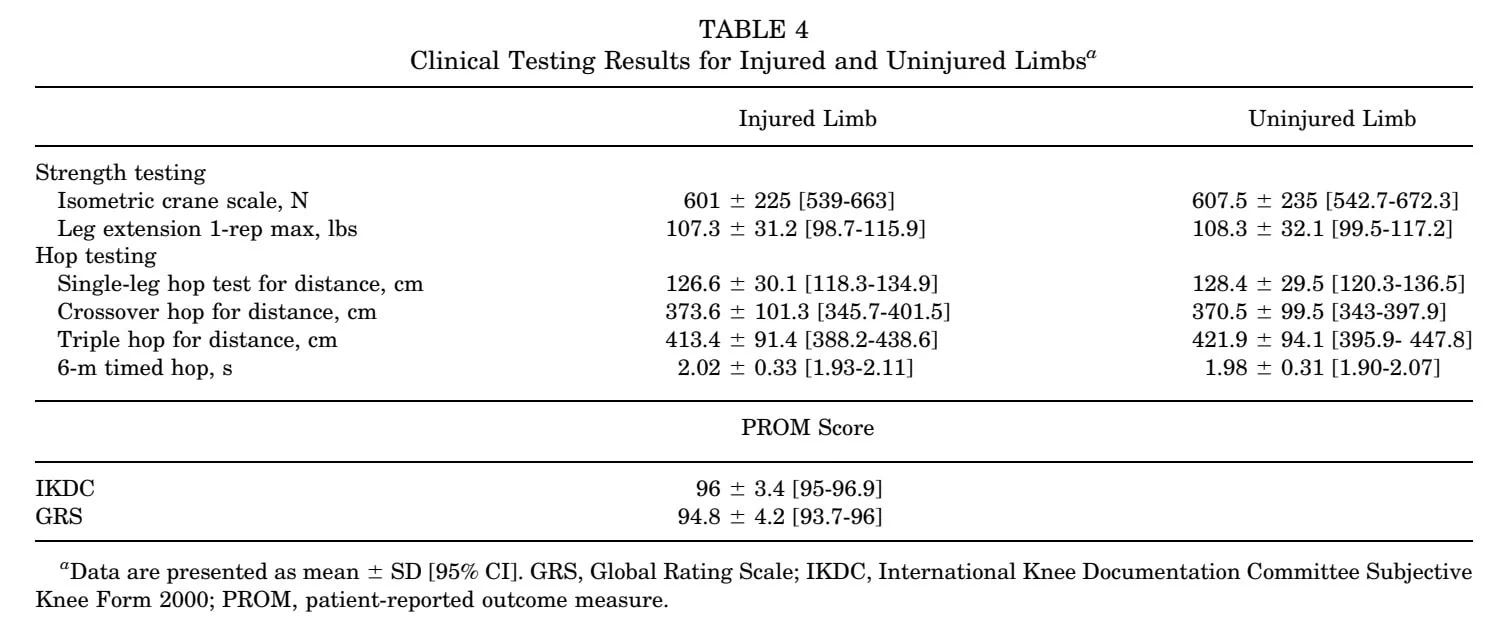
The physiotherapy clinic-based test results revealed that the injured limb had achieved similar strength levels and hop test performance to the noninjured limb, as shown in the table below.
The laboratory testing revealed that despite passing clinical RTS criteria, important deficits remained. Isometric quadriceps strength in the injured limb was, on average, 7.6% lower, and isotonic quadriceps strength was, on average, 4.9% lower compared to the uninvolved limb.
Moreover, nearly 30% of participants still had <80% LSI on isometric testing, and 11% achieved LSI between 85-90%, which is still below the proposed threshold of >90%. Almost half of the patients failed to achieve the proposed 3 Nm/kg isometric knee extension torque normalized to body mass. Although clinic-based test results appeared acceptable, many individuals still had meaningful deficits when gold-standard laboratory testing was examined.
Analysis of the reconstructed limb revealed significant discrepancies in explosive capacity:
- A 6.3% deficit in the early rate of torque development (0-100 ms)
- A 20.9% deficit in the late rate of torque development (100-200 ms)
The magnitude of the late RTD deficit was particularly striking, highlighting a persistent physiological gap. These findings underscore that even when peak force production meets clinical symmetry standards, the ability to generate that force rapidly, needed for athletic readiness, remains substantially compromised.
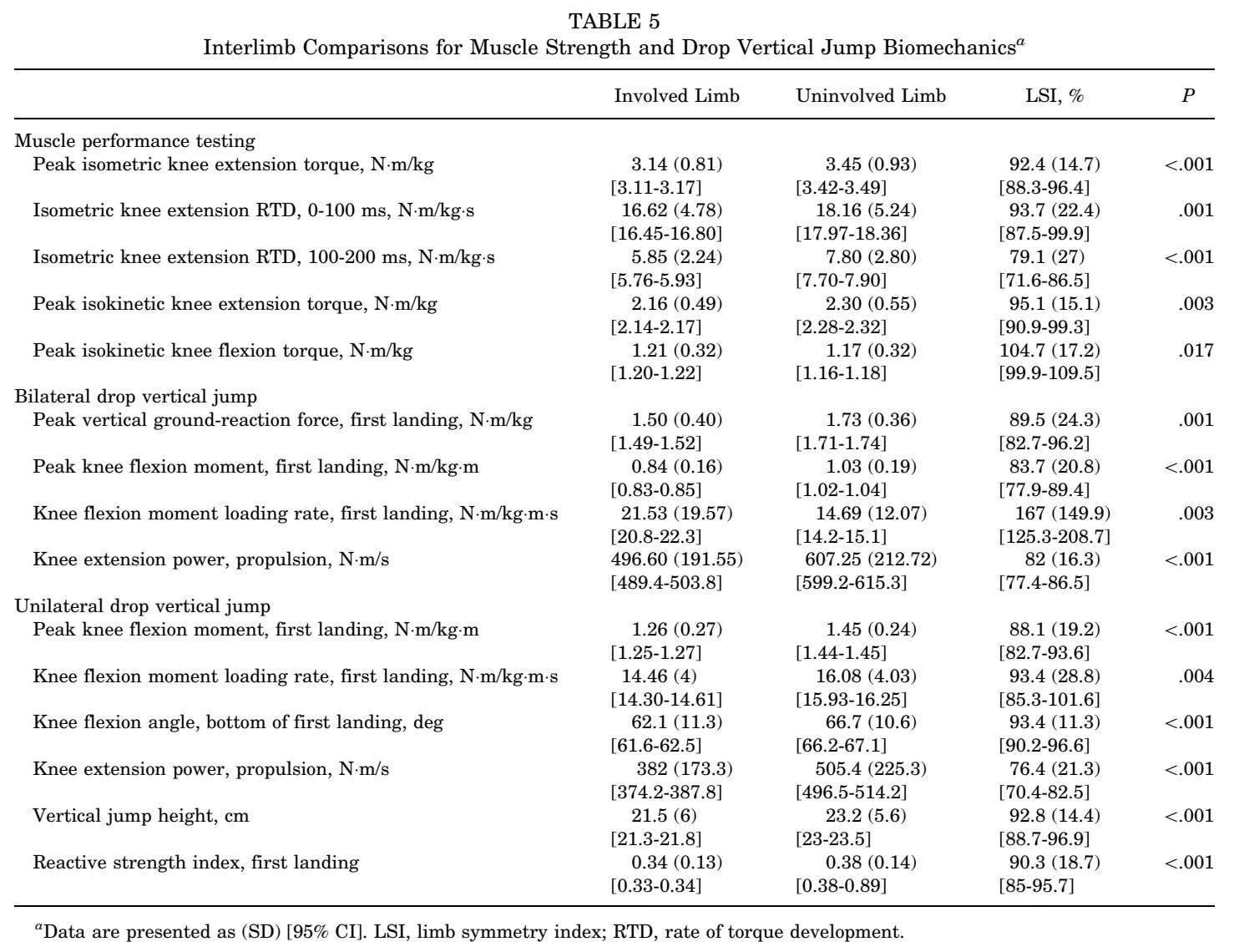
The findings derived from the motion analysis revealed that the injured limb consistently demonstrated underloading patterns when compared to the uninvolved side. The ACLR limb had:
- Lower vertical ground reaction force
- Lower knee flexion moments
- Lower knee extension power
- Lower jump height
- Lower reactive strength index
Questions and thoughts
The test battery was performed within 5 to 15 months after ACLR, and this may reflect a wide variation in physical readiness. Furthermore, no background information was given to understand the components of the patients’ rehabilitation background. When the rate of torque development (RTD) and landing mechanics are insufficiently restored, we can question whether or not these had been components of the rehabilitation program.
RTD reflects how fast force can be produced, not just how much force is produced.
The authors divided RTD into:
- Early RTD: 0-100 ms
- Late RTD: 100-200 ms
Early RTD (0-100 ms) reflects how quickly the nervous system can activate the muscle, making it especially important for rapid reactions like landing, cutting, or decelerating. Late RTD (100-200 ms) reflects how quickly the muscle can continue building force after activation and is influenced more by actual muscle strength capacity. In this study, athletes showed much larger deficits in late RTD than in peak strength, suggesting that they could produce force, but not rapidly enough for sport-specific demands.
This matters because cutting, landing, and deceleration tasks occur extremely rapidly in sport. An athlete may eventually produce high force but still fail to produce it quickly enough during sport-specific tasks.
As landing, pivoting, and cutting mechanics are especially important in these level 1 and 2 sports, we can propose that the RTD is maybe a more important criterion than peak strength, but then, this would not be possible in a regular physiotherapy clinic. These findings raise the question of whether some higher-risk athletes may benefit from additional laboratory-based assessment before RTS. That way, (subtle) differences can still be identified and worked on in the clinic before “clearing” someone who might not be truly ready yet, without us knowing.
Future investigations should explore whether plyometric interventions or velocity-based resistance training would more effectively address these persistent RTD deficits; such research remains a necessary and clinically relevant step in refining rehabilitation protocols.
Talk nerdy to me
The authors used paired t-tests to compare involved and uninvolved limbs and applied a Benjamini-Hochberg false discovery rate correction to reduce the risk of false-positive findings due to multiple comparisons.
This was a cross-sectional study, and this methodology has an inherent limitation, as it captures only a single measurement in time without any long-term follow-up to track progress. Furthermore, we must consider the possibility that a seemingly excellent LSI was merely the result of a relative strength decrease in the noninjured limb, rather than true recovery of the reconstructed side.
This paper highlights a critical discrepancy that clinicians must consider:
- Peak force capacity versus
- Neuromuscular explosiveness and movement quality
While the clinic-based battery effectively captured peak outputs and symmetry during relatively controlled or slower tasks, it may fail to represent the chaotic nature of sport. Athletic participation demands performance under high velocity, in short reaction timeframes with rapid transitions between eccentric and concentric phases. As such, the importance of the rate of torque development cannot be overstated, as ACL injury mechanisms typically occur within milliseconds of initial contact. An inability to generate force rapidly often forces the athlete into compensatory loading strategies. Notably, the observed movement asymmetries were proportionally larger than peak strength deficits, suggesting that restoring maximal strength alone is insufficient to normalize biomechanical behavior.
Take-home messages
This study suggests that physiotherapy clinic-based return-to-sport testing batteries are useful and clinically valuable, but they may not tell the whole story. This study observed that athletes who “pass” common clinical criteria can still demonstrate reduced explosive quadriceps function, altered landing mechanics, and persistent underloading of the surgical limb. The biggest clinical implication is that symmetry in simple strength and hop tests does not necessarily equal restoration of high-level neuromuscular function. Thus, clinic-based test batteries may not tell the whole truth for athletes post-ACLR.
Reference
LEARN TO OPTIMIZE REHAB & RTS DECISION MAKING AFTER ACL RECONSTRUCTION
Sign up for this FREE webinar and top leading expert in ACL rehab Bart Dingenen will show you exactly how you can do better in ACL rehab and return to sport decision making
