Plantar Fasciitis | Plantar Fasciopathy | Diagnosis & Treatment

Plantar Fasciitis | Plantar Fasciopathy | Diagnosis & Treatment
Introduction & Pathomechanism
Plantar fasciitis is a form of plantar heel pain and it is a common problem in adults. It can lead to severe pain, causing significant disability and impairment of daily activities. It is now named plantar fasciopathy to replace the term plantar fasciitis, as inflammation is not the causative factor. We don’t necessarily know which structures lead to pain in a patient’s heel. Only until a diagnosis is confirmed can we use pathognomic terms.
Pathomechanism
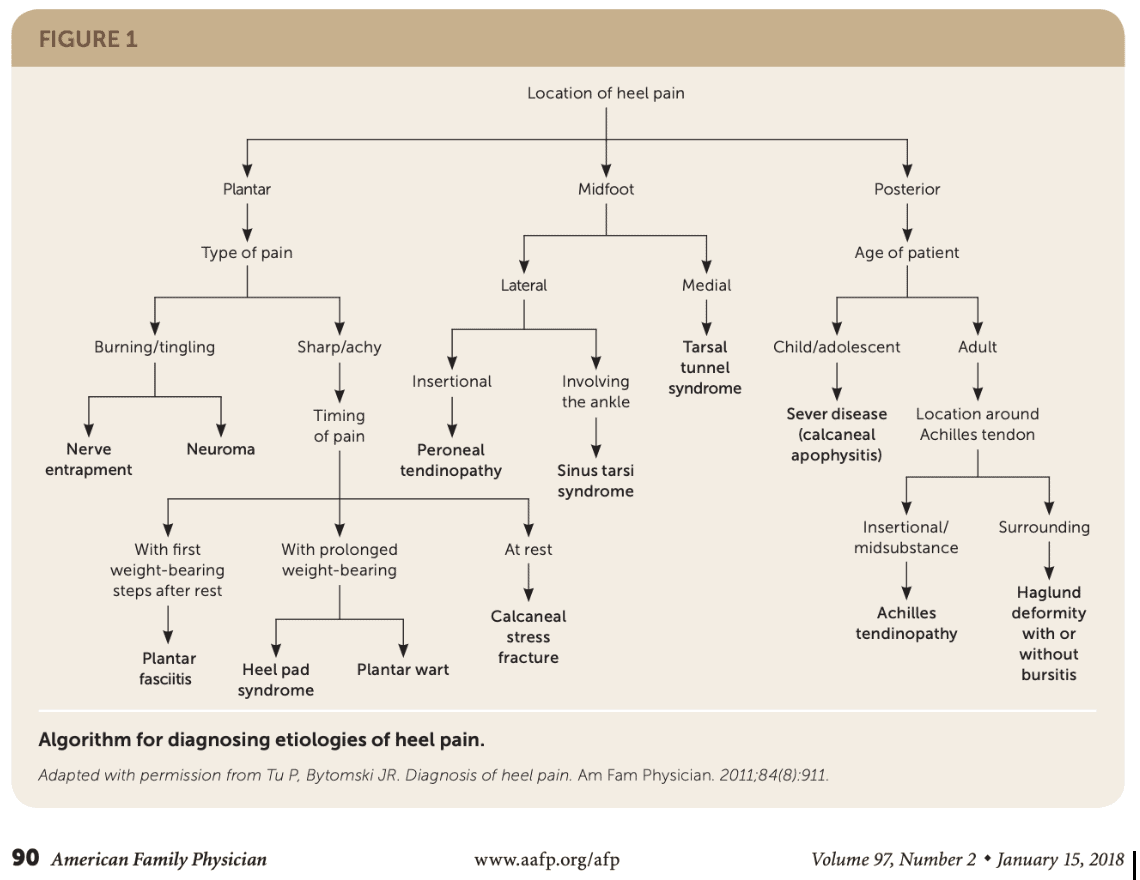
Histological examination and medical imaging in patients with pain under the heel have revealed that multiple tissues may be involved. However, there is a lack of association between imaging findings and symptoms. An algorithmic approach can be used to narrow the possible underlying causes.
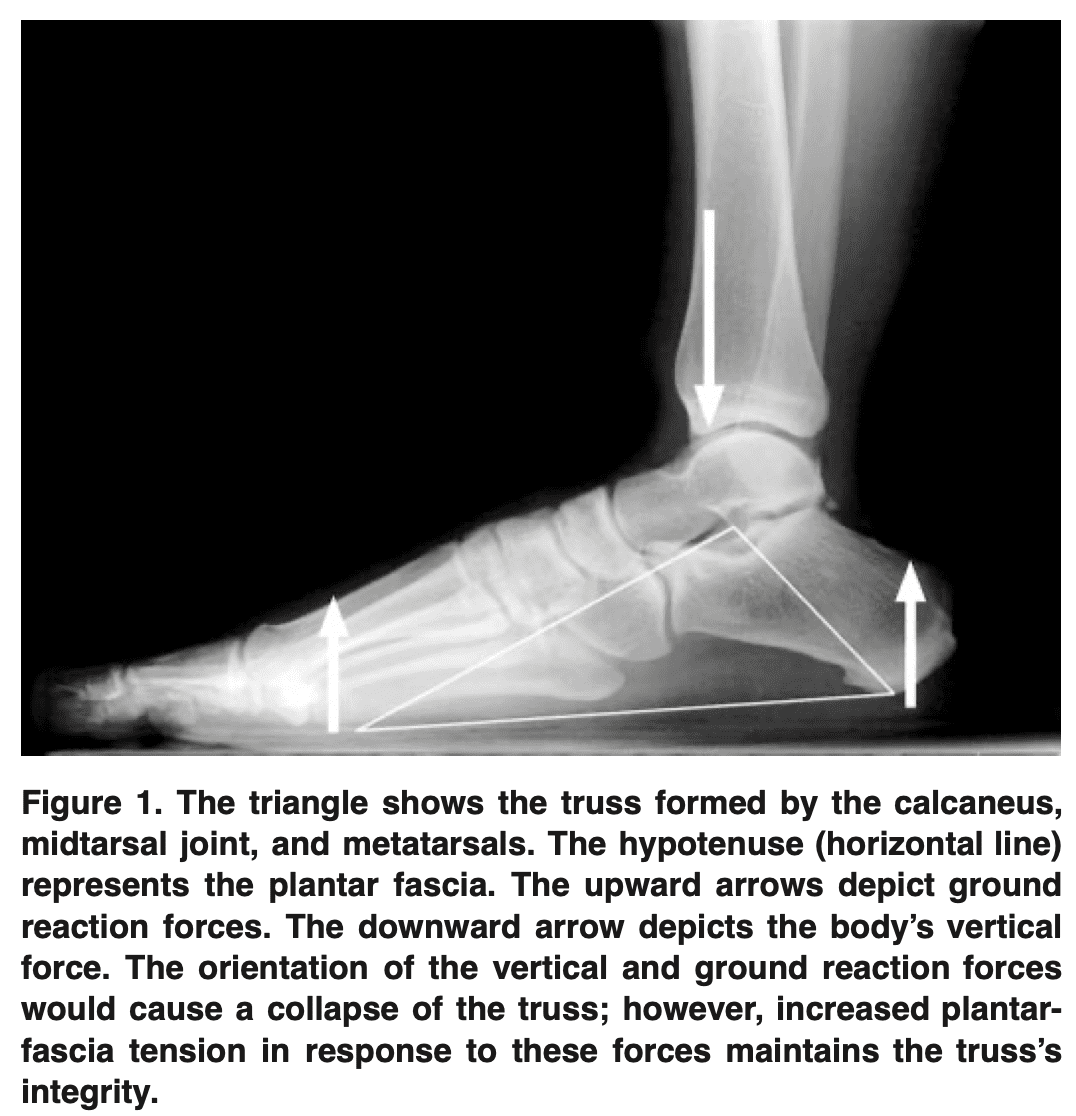
Plantar fasciopathy is one of the most involved causes of plantar heel pain. The plantar fascia arises from the posteromedial calcaneal tuberosity and inserts into each metatarsal head to form the foot’s longitudinal arch. When it is repetitively overloaded, the plantar fascia can become thickened and show degenerative changes.
Epidemiology
Both sedentary people and athletes are affected by plantar heel pain. In the category of plantar fasciopathy, the most affected are middle-aged females who tend to be obese or overweight. Among the possible causes, plantar fasciopathy (previously known as plantar fasciitis) is thought to be responsible for causing plantar heel pain in 1 in 10 of the population.
Clinical Picture
Risk Factors
The following risk factors have been defined:
- Limited ankle dorsiflexion ROM: it is taught to cause overpronation which increases the loads on the medial plantar fascia.
- Rigid foot
- Overpronation or excessive supination
- High foot arch – low arch
- High BMI
- Repetitive overload – (high running volume)
- Wearing spike shoes with running
- Standing for prolonged periods of time
- Intrinsic foot and calf muscle tightness
Signs and Symptoms
The most common symptom is throbbing medial plantar heel pain that worsens with the first steps after rest. The pain usually goes away after a few minutes of ambulation, but it can return if you continue to bear weight. Sharp, stabbing pain is typically felt when palpating the medial calcaneal tuberosity and the medial side of the plantar fascia. This sharp sensation of pain is also typically reported when taking the first step of the day or after prolonged periods of rest. In more severe cases pain may be present during walking and at rest.
Examination
Provocation tests
Windlass Test:
Examination of ankle and foot mobility. Especially the range of motion of dorsiflexion and greater toe extension can be impaired (hallux rigidus), limiting the Windlass mechanism.
The windlass mechanism is biomechanically explained as follows:
The windlass mechanism of the plantar fascia is a biomechanical connection between the plantar fascia and the metatarsophalangeal joint (MPJ) that aids in arch support and deforms to absorb some of the impact energy from the foot hitting the ground. The ideal windlass mechanism presupposes that the plantar fascia has a length that is almost constant to be able to directly associate toe dorsiflexion with a change in arch form. The toe moves to dorsiflexion and depresses the metatarsal head during the push-off phase of locomotion, which tightens the plantar fascia. As the arch-spring collects and releases energy during walking, the plantar fascia likewise extends and then shortens.
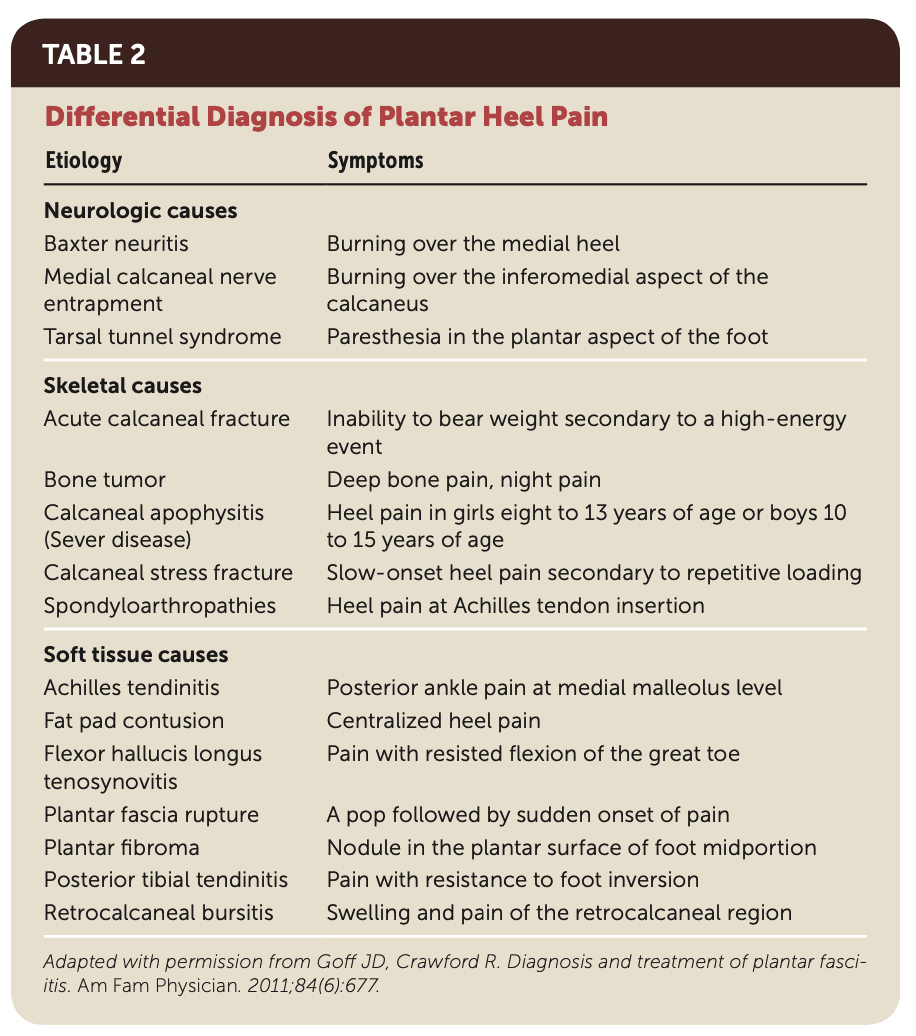
Differential Diagnoses
- Calcaneal stress fractures may cause diffuse plantar heel pain and occur with repetitive overloading, so more in for example runners, soldiers, etc. A positive squeeze test may reveal tenderness on the medial and lateral sides of the calcaneus.
- Heel fat pad atrophy: central plantar heel pain, located at the middle part of the calcaneus, more with barefoot walking and on hard surfaces.
- Tarsal tunnel syndrome: pain, tingling, and numbness in the plantar foot.
- S1 radiculopathy
- Systemic causes
Treatment
The initial stages of treatment focus on relative rest, avoiding aggravating activities, and strengthening exercises. Stretching of the plantar fascia is commonly reported along with the use of anti-inflammatory drugs and ice. Prefabricated or custom-made orthotics, arch taping, night splinting, and physical therapy are all effective treatments that can be combined with more conservative methods. You can educate the patient about the self-limiting nature of the pathology.
Plantar fascia stretching was more effective than Achilles tendon stretching in 1 RCT by DiGiovanni in 2003. However, a more recent trial by Rathleff et al. in 2015 found that high-load strengthening led to faster improvement in pain and function, although both groups improved.
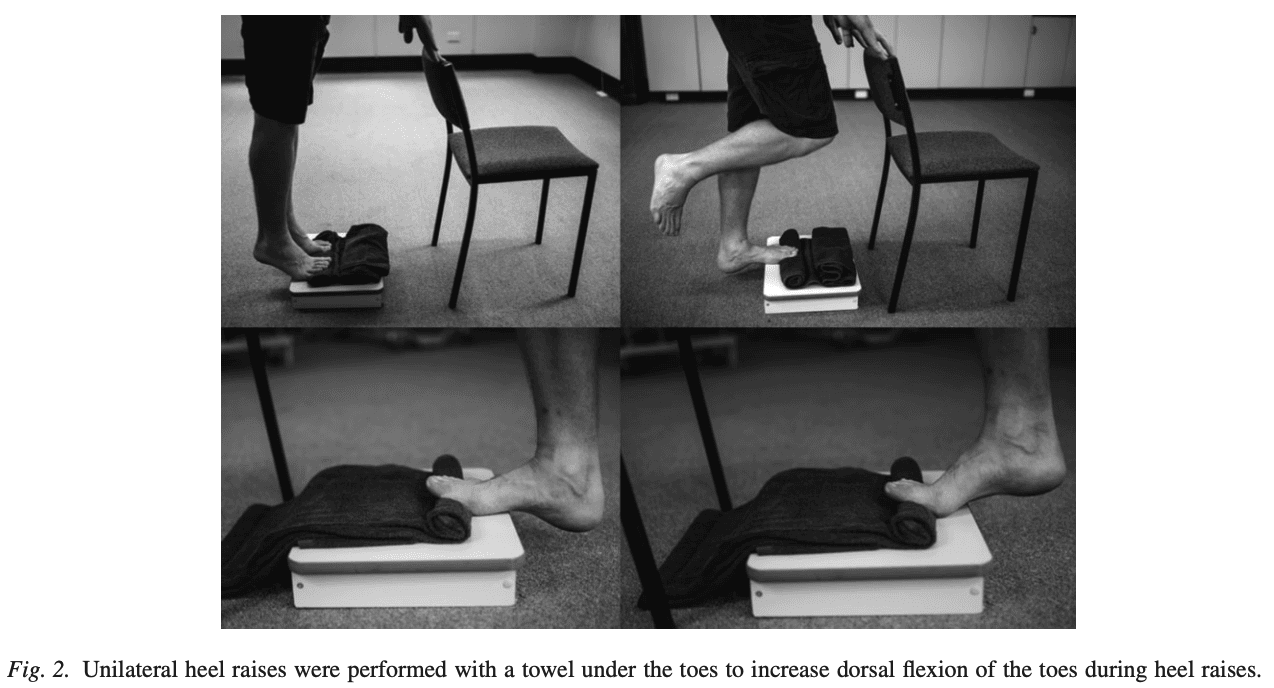
Patients were told to do the exercises every other day for three months. Every heel rise included a 3-second concentric phase (going up) and a 3-second eccentric phase (coming down), followed by a 2-second isometric pause at the top. The high-load strengthening was done gradually. They began with three sets of 12 repetitions maximum (RM). The maximum amount of weight that the patient can lift 12 times through the full range of motion while maintaining proper form is defined as the 12RM. After two weeks, the load was increased by carrying books in a backpack and reducing the number of repetitions to 10RM while increasing the number of sets to four.
Other conservative approaches include
- Orthoses for medial arch support: both over-the-counter or customized insoles are effective
- Taping for medial arch support
- Extracorporeal shock wave therapy (ESWT)
- Corticosteroids are frequently prescribed to treat pain and inflammation. Although plantar fasciitis is a degenerative rather than an inflammatory process, corticosteroids have been shown to have a short-term therapeutic effect. It can however lead to fat pad atrophy which is another cause of plantar heel pain.
References