Migraine | Diagnosis & Treatment | All a physio needs to know

Physiotherapy for Migraines | Assessment & Treatment
Introduction & Epidemiology
The word “migraine is derived from the Greek word “hemikrania,” which was eventually translated into Latin as “hemigranea,” which was eventually translated to “migraine” in French. They are characterized by throbbing pain on one side of the head, a migraine is a moderate to severe headache.
Migraine attacks are intricate brain processes that frequently last from several hours to several days. Without an aura, migraines are most frequently encountered (75 percent of cases).
Additionally, a lot of people experience symptoms like feeling or being unwell, as well as increased sensitivity to light or sound.
Around 1 in 5 women and 1 in 15 men suffer from migraines, making it a widespread medical disease. Early adulthood is typically when they start.
Epidemiology
Stovner et al. (2007) found a lifetime prevalence of 14% for migraine. Migraines are about 3 times more prevalent in women compared to men. First episodes often start during puberty and prevalence increases until the ages of 35 to 39 before it decreases, especially after menopause (Lipton et al. 2007). In addition, it is ranked second in terms of the number of years people spend living with a handicap, after back pain.
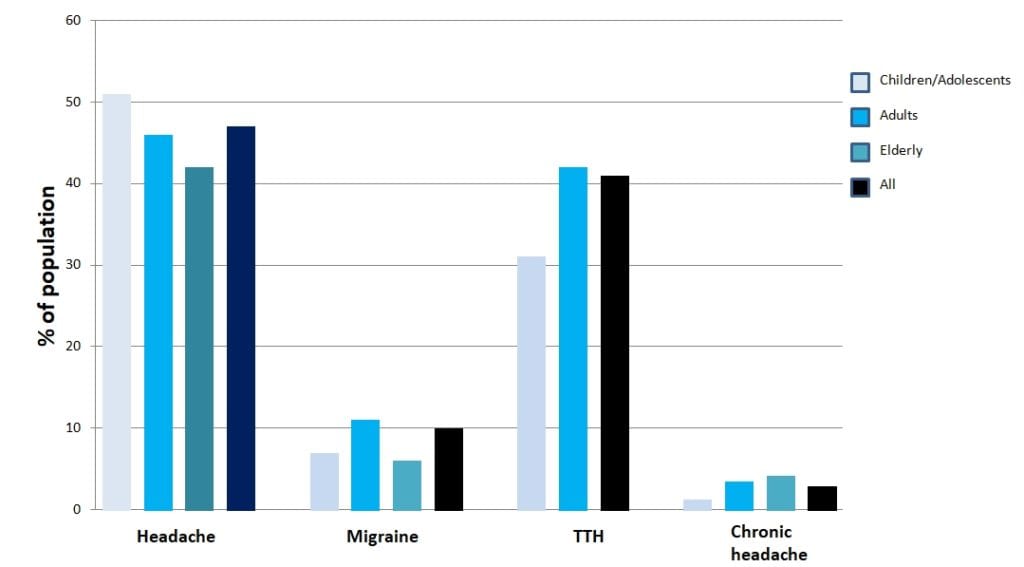
When looking at the current prevalence of different forms of headaches, TTH is the most prevalent form in the adult population worldwide with a mean prevalence of 42%, followed by migraine with 11% (Stovner et al. (2007). The following graph shows the current prevalence of different forms of headaches in different age categories (Stovner et al. (2007):
The following figure shows the prevalence of headaches on different continents around the world: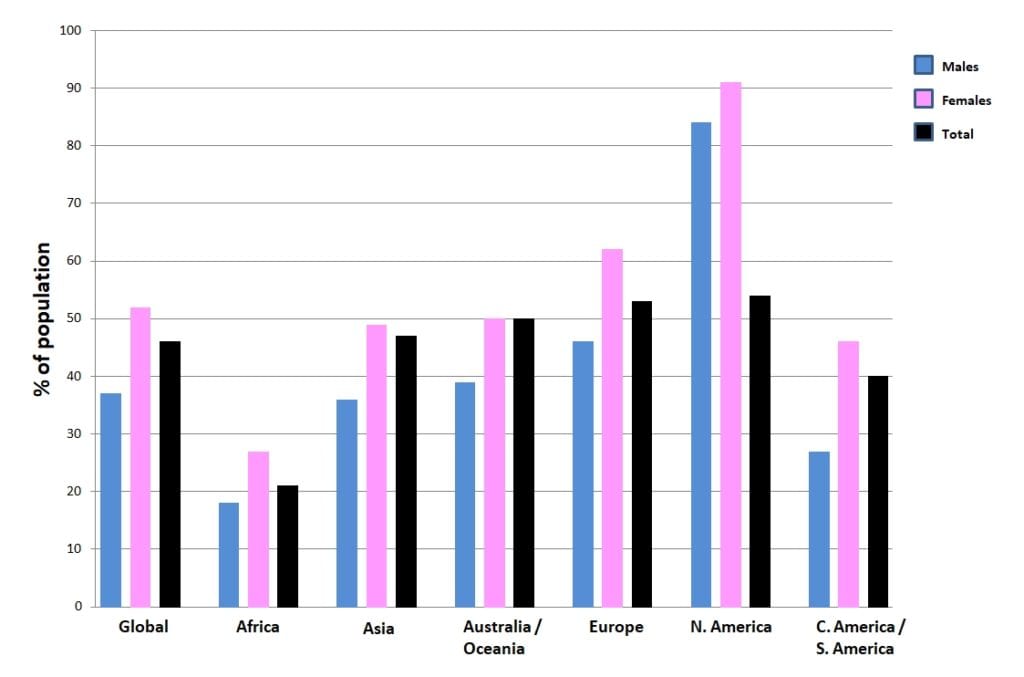
Clinical Picture & Examination
The ICD-H III defines the following criteria to diagnose a migraine headache without aura:
Recurrent headache disorder manifesting in attacks lasting 4-72 hours. Typical characteristics of the headache are unilateral location, pulsating quality, moderate or severe intensity, aggravation by routine physical activity, and association with nausea and/or photophobia and phonophobia.
Diagnostic criteria:
A. At least five attacks1 fulfilling criteria B-D
B. Headache attacks lasting 4-72 hr (untreated or unsuccessfully treated)2;3
C. Headache has at least two of the following four characteristics:
1. unilateral location:
- pulsating quality
- moderate or severe pain intensity
- aggravation by or causing avoidance of routine physical activity (eg, walking or climbing stairs)
2. During headache at least one of the following:
-
- nausea and/or vomiting
- photophobia and phonophobia
Migraines with aura are defined as follows:
Recurrent attacks, lasting minutes, of unilateral fully-reversible visual, sensory or other central nervous system symptoms that usually develop gradually and are usually followed by headache and associated migraine symptoms.
Diagnostic criteria:
A. At least two attacks fulfilling criteria B and CB. One or more of the following fully reversible aura symptoms:
- visual
- sensory
- speech and/or language
- motor
- brainstem
- retinal
C. At least three of the following six characteristics:
- at least one aura symptom spreads gradually over ≥5 minutes
- two or more aura symptoms occur in succession
- each individual aura symptom lasts 5-60 minutes1
- at least one aura symptom is unilateral2
- at least one aura symptom is positive3
- the aura is accompanied, or followed within 60 minutes, by headache
D. Not better accounted for by another ICHD-3 diagnosis.
Examination
In comparison with healthy controls, migraineurs differ on provocation testing as well as neck endurance testing.
In comparison, Szikszay et al. (2019) conducted a systematic review and meta-analysis on the differences between MSK impairments in migraineurs and healthy people.
They recommend including testing for limited cervical ROM including the flexion-rotation test, forward head position, and pressure pain thresholds.
The goal of provocation tests is to recreate the patient’s familiar pain. This way, you are able to confirm the location of nociception in the cervical structures, possibly leading to referred pain to the head. While provocative testing for CGH can be done with the techniques shown in the following tab, the phenomenon of referred pain to the head for tension-type headaches and migraine can be provoked with the Watson test:
Although no clear cut-off values are given, the performance time can give an indication about neck flexor endurance:
Upper cervical range of motion in the direction of rotation can be reliably and accurately assessed with the Flexion-Rotation Test (Hall et al. 2010a, Ogince et al. 2007, Hall et al 2010b). This test – if positive – can give you an indication of limited rotation on segments C1/C2. In turn, hypomobility on C0/C1 or C2/C3 can lead to this limitation in rotation on C1/C2.So in case of a positive test, we still need to perform intervertebral motion assessment of all upper cervical segments in order to find the dysfunctional segment.
100% Free Headache Home Exercise Program