Lateral Ankle Sprain | Diagnosis & Treatment

Clinical Presentation & Examination
Risk factors
Vuurberg et al (2018) described several risk factors:
Intrinsic:
- Limited dorsiflexion ROM
- Reduced proprioception
- Reduced preseason deficiencies in postural control (positive single-leg balance test)
- BMI (high and/or low, depending on the source)
- High medial plantar pressures during running
- Reduced strength
- Reduced coordination
- Reduced cardio respiratory endurance
- Limited overall ankle joint ROM
- Decreased peroneal reaction time
- Females > males
- Previous ankle injury (although results are conflicting)
Extrinsic:
- Sport: aeroball, basketball, indoor volleyball, field sports, climbing
- Lots of jumping and landing in volleyball
- Playing soccer on natural grass
- Soccer defender
- High heels
- Competition risk is higher in boys compared to girls
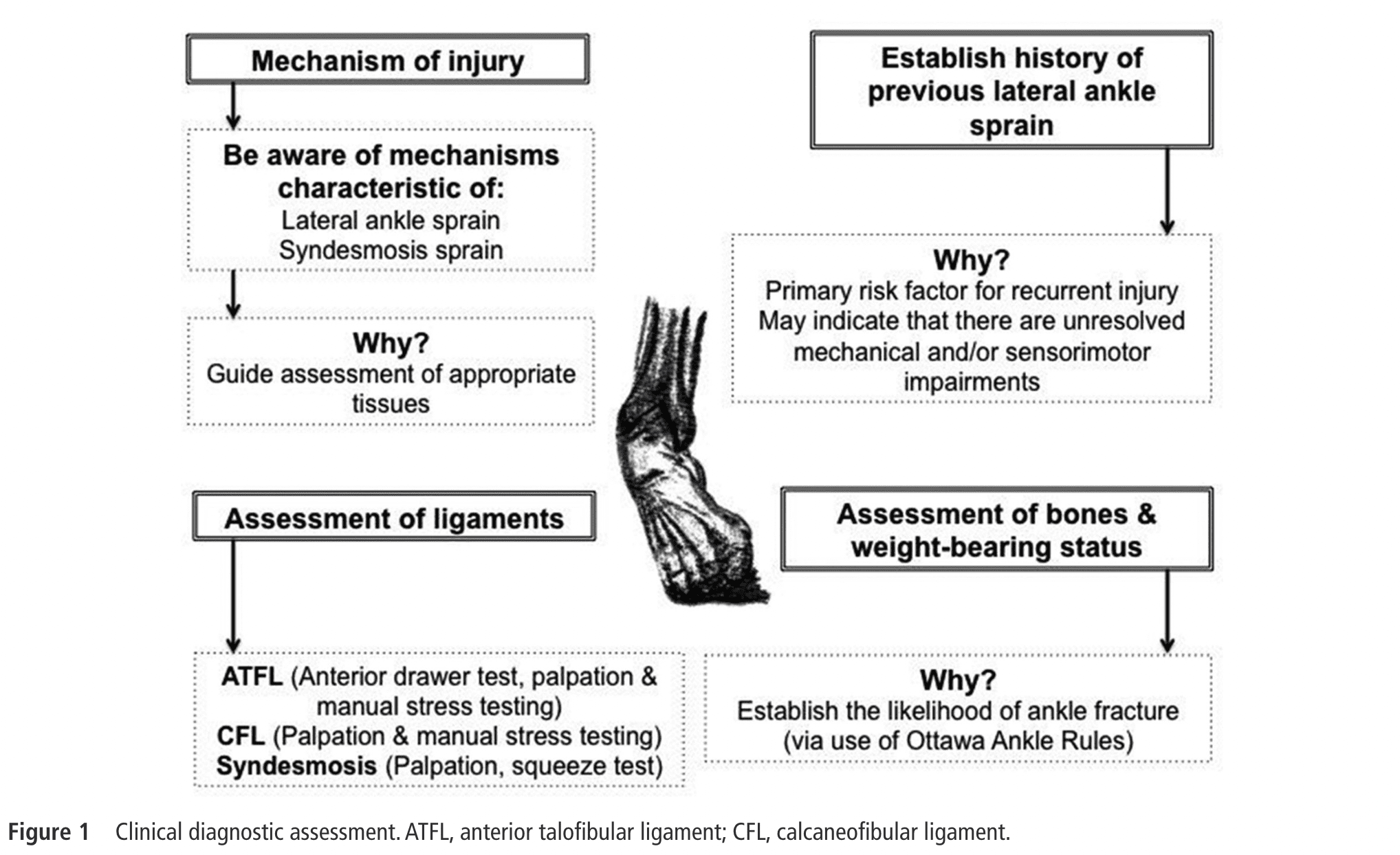
History
Evaluate the severity of the injury and determine the appropriate course of treatment. The examination should begin with a comprehensive history of the injury, including the mechanism of injury, any previous injuries or surgeries, and any associated symptoms such as pain, swelling, or instability (Delahunt et al 2018).
A history of previous sprains is associated with mechanical and sensorimotor impairments and heightens the risk of reinjury (Delahunt et al 2019).
Examination
Next, a physical examination should be performed to assess the extent of the injury. This should include an assessment of ankle range of motion, strength, and stability. Specific tests should also be performed to evaluate the integrity of the ligaments, such as the anterior drawer test, the talar tilt test, and the external rotation stress test. These are described below.
Anterior drawer test
The anterior talofibular ligament is most often injured. Replication of the known pain when palpating or stressing the ligament with passive plantar flexion and inversion is indicative of injury. The anterior drawer test to assess for complete disruption are best performed after 4 to 6 days. A positive test results in a sulcus sign (van Dijk et al 1996).
Talar tilt test
This test can stress the anterior talofibular ligament and/or calcaneofibular ligament, depending on the execution.
External rotation stress test
This test will stress the syndesmosis. It is important to rule out or rule in concomitant or isolated syndesmotic injuries with ankle sprains.
Calcaneofibular Ligament
Assessing the calcaneofibular ligament is possible with palpation or stressing the ligament in passive dorsiflexion with inversion. Do note that the ligament is crossed by the peroneal tendons and sheaths, making it directly palpable for approximately 1 cm. The stress tests should replicate the known pain to be positive.
Ottawa Ankle Rules
To exclude possible fractures we can trust the Ottawa ankle rules. An inability to weight-bear four steps after injury or pain on palpation on the posterior edge of the distal 6 cm of the medial or lateral malleolus should increase your suspicion of a possible fracture. If this is the case, an X-ray is warranted (Gomes et al 2022).
In addition to the physical examination, validated outcome measures can be used to assess the functional status of the ankle and monitor progress during rehabilitation. Examples of these measures include the Foot and Ankle Ability Measure (FAAM) and the Lower Extremity Functional Scale (LEFS).
A full list of things to evaluate can be seen in the table down below:
Other
Static postural balance, dynamic postural balance and gait should be assessed with for example the foot lift test and the star excursion balance test, respectively (Delahunt et al. 2019).
Imaging
Depending on the severity of the injury, imaging studies such as X-rays, ultrasound, or MRI may be ordered to evaluate the extent of the damage and rule out other injuries such as fractures or dislocations. Overall, a thorough examination that considers both physical and functional aspects of the injury is important to accurately diagnose and manage acute lateral ankle sprains (Delahunt et al 2018).
High Ankle Sprain/Syndesmosis Injury
The prevalence of ankle joint syndesmosis ligament injury, with or without the involvement of the lateral ligaments, has been reported to be 20% (Roemer et al. 2014). Tenderness on palpation of the syndesmosis ligaments is the most sensitive test while the squeeze test is the most specific (Sman et al 2015). Both being positive results in a high probability of injury to the syndesmosis ligaments.
Palpation Syndesmosis Ligaments
Squeeze test
External rotation stress test
LEVEL UP YOUR ROTATOR CUFF DISORDER KNOWLEDGE – FOR FREE!