Benign Paroxysmal Positional Vertigo

Body Chart
Background Information
Patient Profile
- Most common form of vertigo (19%)
- 90% posterior canal, 10% horizontal canal
- 1 in 3 affected before 7th decade
- 2/3 female
- Yearly incidence 10-20:100.000
Pathophysiology
Trigger
Otolith particles break off of the macula utriculi and accumulate in the posterior (90%) and horizontal (10%) canal. They accumulate at the lowest point of the canal. Movement of otolith particles during e.g. head rotation cause vertigo and nystagmus
Etiology
- Head trauma (~20%)
- Neurolabyrinthitis (10- 15%)
- Migraine
- Prolonged bedridden period
- Genetic predisposition
Course
Very good prognosis. ~90% symptom free after one maneuver. If strategy is executed properly, success rate of ~100%. If maneuver was done successfully, discomfort subsides within a week. Relapse rate 2-5%
History & Physical Examination
History
Head trauma, migraines, bedridden for extended period, inner ear pathology
- Possibly associated neck pain
- Real vertigo:
- Illusionary sensation of movement (own body, surroundings)
- Tilt of visual surroundings
- Rotational
- Nystagmus with rotation
- Lateropulsion
- Feeling of falling or lifting
- No neurological symptom character
- Associated reactions:
- Vertigo
- Vomiting
- Fainting
- Ataxia
- Hearing problems/Tinnitus
Physical Examination
Active Examination
Neck movement is avoided and leads to AROM limitation
Functional Assessment
Change of head position triggers nystagmus and vertigo
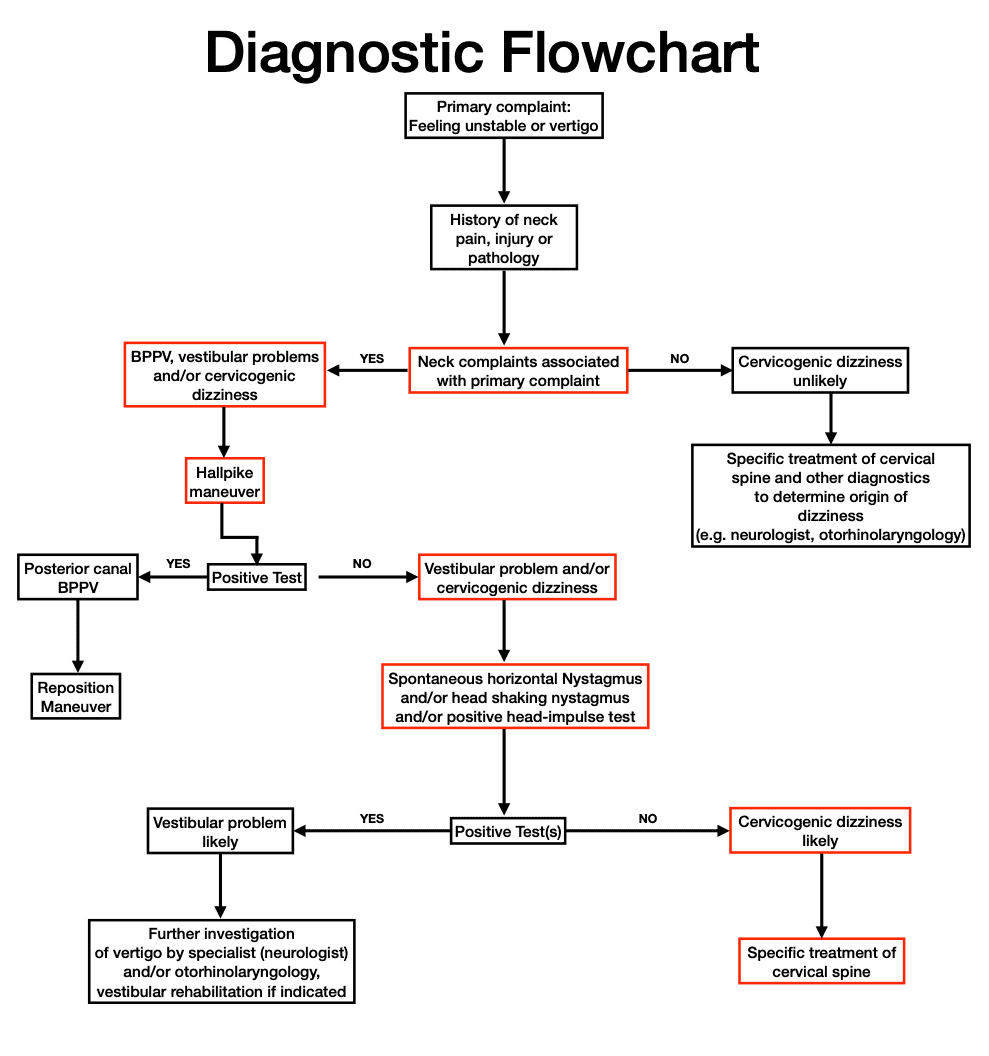
Special Testing
Differential Diagnosis
- Infection
- Intoxication
- Tumor
- Idiopathic
- Psychogenic
- Metabolic
- Phobia
Treatment
Strategy
Maneuvers are very effective. Patient education and instructions on behavior at home are incorporated
Interventions
IMPORTANT
- Maneuver is only then positive if dizziness occurs. Therefore, hold the position.
- After symptoms subside, patients should remain in the end position for ~4min to prevent particles from returning back
- Beware of sudden retropulsion
- In case maneuver fails, wait at least 10 min before trying again
- Max. 3 consecutive tries
Home instructions
- Patients may experience discomfort within the next 24h (normal reaction of CNS)
- No sudden head movements
- Avoid lying on affected side
- In supine, use a pillow under neck to avoid hyper extension
- Lying prone and on unaffected side is permitted
- Adapted Epley maneuver as self-help tool

References
- Epley, J. M. (1992). The canalith repositioning procedure: for treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg, 107(3), 399-404.
- Hauswirth, J. (2008). zervikogener Schwindel: Diagnose und manualtherapeutische Behandlung. (12), 80-93. doi:10.1055/s-2008- 1027384
- Oostendorp, Eupen, v., Erp, v. (1999). Dizziness following whiplash injury: a neurootological study in manual therapy practice and therapeutic implication. The Journal of Manual and Manipulative Therapy, 7, 123-130.
- Reid, S. A., Rivett, D. A., Katekar, M. G., Callister, R. (2014). Comparison of mulligan sustained natural apophyseal glides and maitland mobilizations for treatment of cervicogenic dizziness: a randomized controlled trial. Phys Ther, 94(4), 466-476. doi:10.2522/ptj.20120483
- Schmäl, F. (2005). Benigner paroxysmaler Lagerungsschwindel. In W. M (Ed.), Vestibularfunktion: Brücke zwischen Forschung und Praxis.
- Semont, A., Freyss, G., Vitte, E. (1988). Curing the BPPV with a liberatory maneuver. Adv Otorhinolaryngol, 42, 290-293.
- Sloane, P. D., Coeytaux, R. R., Beck, R. S., Dallara, J. (2001). Dizziness: state of the science. Ann Intern Med, 134(9 Pt 2), 823-832.
- Stoll, W., Most, E., Tegenthoff, M. (2004). Benigner Paroxysmaler Lagerungsschwindel. In W. Stoll (Ed.), Schwindel und Gleichgewichtsstörungen (Vol. 4, pp. 141-146). Stuttgard: Thieme Verlag.
- Wiemer, M. (2011). Benigner paroxysmaler Lagerungsschwindel (BPLS). Manuelle Therapie, 15, 172-177. doi:dx.doi.org/10.1055/s-0031- 1281694Wrisley, D. M., Sparto, P. J., Whitney, S. L., & Furman, J. M. (2000). Cervicogenic dizziness: a review of diagnosis and treatment. J Orthop Sports Phys Ther, 30(12), 755-766. doi:10.2519/jospt.2000.30.12.755