
Research
December 29, 2025
Knee osteoarthritis rehabilitation: integrated exercises, nutrition and biomechanics framework insights from a large-scale narrative review.

Introduction
Conservative management is widely recognized as the first-line treatment for knee osteoarthritis rehabilitation, particularly in the context of a rising global burden, with projections suggesting a 74% increase in incidence by 2050. Exercise-based interventions—including resistance training, mobility and flexibility exercises, aerobic conditioning, and task-specific training targeting coordination, balance, proprioception, and neuromuscular control—have consistently demonstrated effectiveness in reducing pain and improving physical function and muscle strength.
Despite this strong evidence base, clinical implementation remains challenging. Physiotherapists often face uncertainty regarding when and how to progress exercises, which clinical or performance criteria should be achieved before advancing task complexity, and what constitutes an “advanced” exercise within the context of knee osteoarthritis. This narrative review aims to guide exercise progression in knee osteoarthritis rehabilitation, while also exploring the role of dietary strategies as a complementary component of conservative management.
Methods
A comprehensive literature search was conducted in PEDro, Web of Science, Embase, PubMed, and the Cochrane Library from database inception to June 1, 2025. Search strategies combined terms related to knee osteoarthritis (knee osteoarthritis) and therapeutic interventions, including exercise therapy, physical therapy, rehabilitation, strength training, kinesiotherapy, and dietary interventions, using both controlled vocabulary and free-text terms adapted for each database.
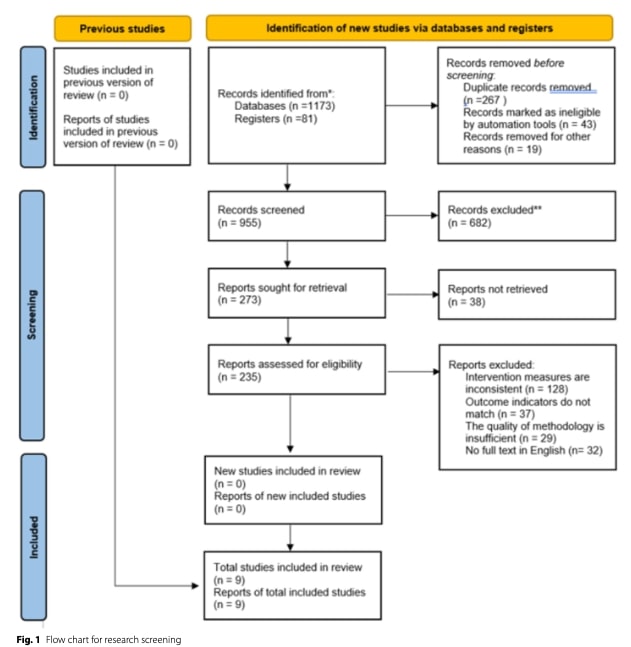
Two independent reviewers screened titles and abstracts, followed by full-text assessment of eligible studies according to predefined inclusion and exclusion criteria. Disagreements were resolved through consensus or consultation with a third reviewer. The selection process followed PRISMA 2020 guidelines.
Eligible studies were randomized controlled trials involving participants diagnosed with knee osteoarthritis according to American College of Rheumatology criteria and evaluating non-pharmacological interventions such as exercise, physical therapy, dietary approaches, or patient education. Studies were excluded if they were non-English, non-human, lacked full-text access, focused on pharmacological treatments, or used unreliable outcome measures.
Results

Pathophysiology
Knee osteoarthritis is characterized by progressive articular cartilage degeneration, including fibrillation, softening, and eventual loss of cartilage tissue, accompanied by subchondral bone alterations such as sclerosis and cyst formation. In parallel, soft tissue impairments, particularly low-grade synovial inflammation, further compromise the knee joint’s ability to provide smooth articulation and effective shock absorption. These changes result in pain during movement, weight-bearing activities, and tasks involving high force absorption.
As knee osteoarthritis progresses, joint space narrowing becomes more pronounced, contributing to increased joint stiffness. Persistent low-grade synovitis may lead to joint effusion, which induces arthrogenic muscle inhibition, commonly resulting in quadriceps weakness and atrophy. These structural and neuromuscular alterations are closely associated with functional and psychosocial consequences, including impaired balance, increased fall risk, reduced social participation, and diminished quality of life.
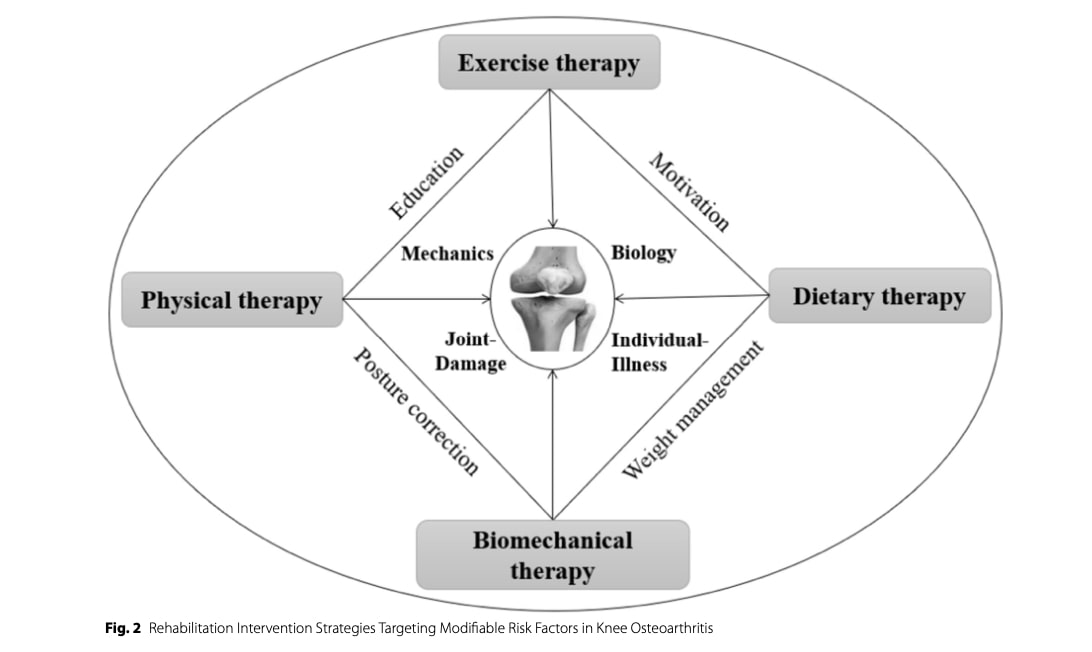
Risk factors and conservative management
Numerous risk factors for knee osteoarthritis have been identified, including biomechanical factors, physical inactivity, obesity, abnormal limb alignment, and prior joint injury or trauma. Conservative management for knee osteoarthritis rehabilitation should aim to mitigate these modifiable risk factors. In addition to therapeutic exercise, interventions such as bracing, orthopedic insoles, mobility aids, and selected physical modalities (e.g., ultrasound, extracorporeal shockwave therapy, pulsed electromagnetic fields, and low-level laser therapy) have been proposed by some authors as potentially relevant adjuncts, although their effectiveness varies and should be considered secondary to exercise-based rehabilitation.
Role of exercise in osteoarthritis
Knee osteoarthritis is commonly associated with arthrogenic muscle inhibition, leading to functional impairments, particularly during ambulation. Exercise therapy plays a central role in reducing muscle inhibition, restoring muscle strength, and normalizing gait patterns.
While exercise was initially thought to have no direct structural effect on articular cartilage, emerging evidence suggests that it may positively influence synovial fluid circulation, thereby enhancing cartilage nutrient delivery and waste product removal. These physiological effects may contribute to reductions in inflammatory markers observed in patients undergoing regular exercise therapy, even in the absence of clear structural cartilage regeneration.
Despite strong evidence supporting exercise for symptom relief, the optimal exercise modalities and progression strategies for knee osteoarthritis rehabilitation remain incompletely defined.
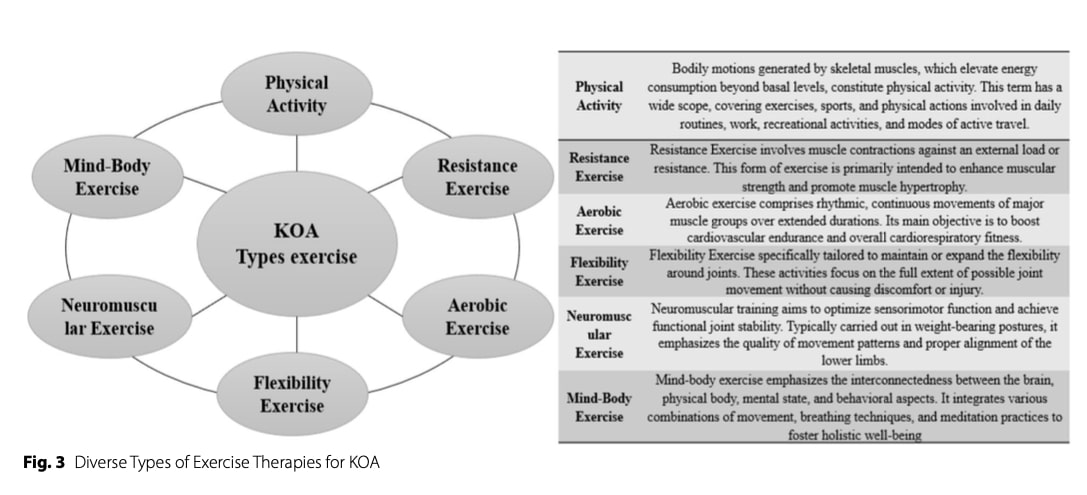
Aerobic exercises
Exercise modality:
Low-impact aerobic activities such as cycling and swimming are traditionally recommended due to lower joint loading. However, emerging evidence indicates that higher-impact activities such as running are not necessarily associated with increased structural knee damage in individuals with knee osteoarthritis, provided symptoms are appropriately monitored and progression is gradual.
Parameters:
- ≥150 minutes per week of moderate-intensity aerobic exercise, accumulated over multiple sessions.
Resistance training
Exercise modality:
Resistance training may begin with isometric exercises in cases of significant pain or inhibition, progressing toward dynamic, multi-joint strengthening exercises targeting the quadriceps, hamstrings, and gluteal muscles.
Parameters:
- Initial loading allowing 15–20 repetitions (approximately ~10% 1RM)
- Progressive loading toward 40–60% 1RM, with 1–3 sets of 10–15 repetitions
- Performed 2–3 times per week, with adequate recovery between sessions
Biopsychosocial approach
Knee osteoarthritis rehabilitation requires an evidence-based, individualized and patient-centred approach. A comprehensive assessment is therefore essential to evaluate not only physical impairments but also psychological and social domains that influence pain, function, and treatment adherence.
Psychological domains
Psychological factors such as kinesiophobia, pain catastrophizing, anxiety, depressive symptoms, and self-efficacy for symptom management are highly relevant in knee osteoarthritis and should be routinely explored. These factors can amplify pain perception, limit physical activity, and negatively affect rehabilitation outcomes.
Cognitive behavioural therapy (CBT) has demonstrated benefits in improving pain, physical function, and self-efficacy, and may be an effective adjunct to physiotherapy when maladaptive beliefs or psychological distress are identified.
Monitoring and outcome measures
Validated patient-reported outcome measures such as the Western Ontario and McMaster Universities Arthritis Index (WOMAC) and the 36-Item Short Form Health Survey (SF-36) are valuable tools for assessing baseline symptoms, functional status, and changes over time, supporting both clinical decision-making and treatment monitoring.
Dietary Intervention
Weight management plays a central role in knee osteoarthritis rehabilitation. A 5–10% reduction in body weight has been shown to significantly reduce pain and improve function. Weight loss is also associated with reductions in systemic inflammatory markers, including tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and C-reactive protein (CRP), which are implicated in cartilage degradation.
Beyond caloric restriction, nutritional quality should be considered. Diets rich in omega-3 fatty acids exhibit anti-inflammatory properties through modulation of inflammatory pathways, contributing to pain reduction and functional improvement. Fiber-rich diets, commonly derived from fruits and vegetables, are associated with lower systemic inflammation and also provide antioxidants such as vitamins C and E, which may reduce oxidative stress and inflammatory activity.
Biomechanical approach
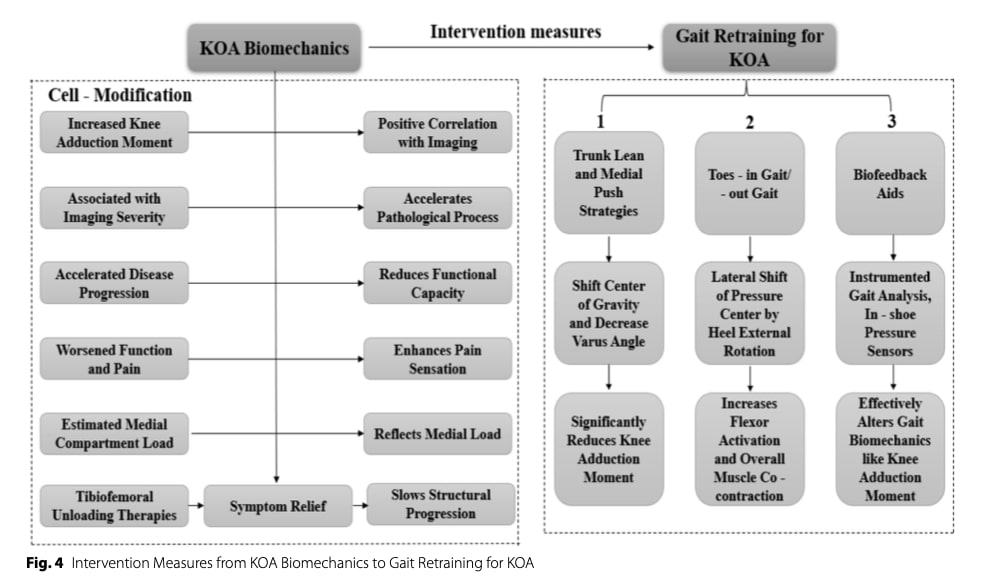
Altered load distribution across the knee joint increases mechanical stress on articular cartilage and contributes to symptom progression. Interventions aiming to optimize lower-limb alignment and reduce excessive joint loading may therefore improve pain and function. Notably, an association has been identified between an increased knee adduction moment during gait and pain severity, disease progression, and medial compartment degeneration.
Orthoses, including insoles, knee braces, and walking aids, may reduce mechanical constraints on the knee. Lateral wedge insoles can decrease the knee adduction moment by laterally shifting the ground reaction force and may be particularly relevant for individuals with varus alignment and medial knee osteoarthritis. However, current evidence supporting insole use for knee osteoarthritis rehabilitation remains weak and inconsistent, possibly due to heterogeneity in patient presentation and biomechanical response.
Gait retraining
Gait retraining strategies aim to reduce the knee adduction moment, which has been linked to medial knee osteoarthritis severity and progression. Biofeedback-based interventions, such as in-shoe pressure sensors, have shown effectiveness in modifying gait mechanics, while visual feedback using mirrors may offer a low-cost alternative.
Specific strategies—including trunk lean, medial knee thrust (“medial push”), reduced stride length, and toe-out gait—have been shown to reduce knee adduction moment by altering lower-limb alignment and loading patterns. However, these strategies may increase loading at adjacent joints (hip or ankle) or increase muscle co-contraction, potentially raising compressive forces and symptoms.
Physiotherapist intervention
Physiotherapists play a central role in implementing a biopsychosocial approach to knee osteoarthritis. A thorough assessment should include evaluation of joint mechanics, range of motion, muscle strength, proprioception, and gait, supported by clinical history and validated outcome measures such as WOMAC and SF-36.
Psychological factors—including kinesiophobia, catastrophizing, anxiety, and depressive symptoms—should be systematically screened. When indicated, referral for psychological interventions such as CBT may enhance outcomes, particularly by improving self-efficacy.
As exercise therapy is the cornerstone of knee osteoarthritis management, treatment adherence represents a major challenge. Barriers such as beliefs, social support, educational level, and financial constraints may hinder long-term engagement in self-management strategies.
To address these barriers, physiotherapists should adopt flexible and patient-centered strategies, including education, shared decision-making, and where appropriate, involvement of the patient’s family or social environment to support sustained behavior change.
Manipulative and adjuvant therapies
Evidence supporting manual therapy and other adjunctive physical modalities in knee osteoarthritis (knee osteoarthritis) is limited. Manual therapy (mobilization/manipulation) may provide short-term pain relief, sometimes greater than exercise alone immediately post-intervention, but long-term benefits are unclear and evidence quality is low. Techniques such as kinesio taping and acupuncture show mixed or inconclusive results.
Beyond physical therapy techniques, several adjuvant therapies are used alongside core interventions (exercise, weight management). Intra-articular hyaluronic acid injections may offer moderate short- to medium-term pain and functional improvement, though results vary and long-term cost-effectiveness is debated. Low-level laser therapy (LLLT) has shown short-term pain reduction and functional gains with a good safety profile, but optimal parameters remain uncertain. Other options—such as topical NSAIDs, TENS, and heat/cold therapy—may help manage symptoms, particularly during pain flares, but have smaller effects than core treatments. Overall, adjuvant therapies should be individualized and used only as supplements within a comprehensive rehabilitation program..
Questions and Thoughts
A key question in knee osteoarthritis rehabilitation concerns the structural effects of exercise on joint tissues, particularly whether specific exercise modalities can improve or preserve cartilage structure. Current evidence on this topic remains conflicting and inconclusive. Human studies have not consistently demonstrated meaningful improvements in cartilage thickness or volume following exercise interventions; however, another narrative review suggests that exercise may influence osteoarthritis pathogenesis through biological and inflammatory pathways, even in the absence of clear structural regeneration.
Preclinical research provides important mechanistic insights. For example, animal studies have shown that aerobic exercise may reduce the expression of inflammatory and catabolic markers, including interleukin-1β (IL-1β), caspase-3, and matrix metalloproteinase-13 (MMP-13)—all of which are implicated in cartilage degradation. These findings support the hypothesis that appropriate mechanical loading may exert a chondroprotective effect, potentially slowing degenerative processes rather than reversing established structural damage.
From a clinical perspective, exercise appears to exert its benefits primarily through symptom modulation and functional improvement, rather than direct cartilage regeneration. The reviewed literature suggests that aquatic exercise may be particularly useful in the early stages of rehabilitation to reduce pain and improve range of motion, thereby facilitating patient engagement. As symptoms and mobility improve, land-based exercise tends to provide greater benefits for pain reduction and functional gains, likely due to higher mechanical and neuromuscular demands.
Importantly, it must be acknowledged that structural changes observed in osteoarthritis do not consistently correlate with pain or functional impairment. This dissociation may explain why surgical interventions such as knee arthroplasty do not invariably result in superior outcomes compared with conservative, holistic management, particularly in earlier disease stages. Consequently, an excessive focus on structural alteration may be clinically misleading.
These findings reinforce the need for physiotherapists to adopt a rigorous, biopsychosocial approach to knee osteoarthritis rehabilitation. A comprehensive assessment should encompass physical impairments, functional limitations, psychosocial factors, and barriers to adherence, all of which strongly influence outcomes. Despite robust guideline recommendations supporting conservative management, implementation remains suboptimal; the reviewed literature suggests that fewer than 50% of individuals with knee osteoarthritis receive evidence-based conservative care.
Emerging technologies, including artificial intelligence (AI), are increasingly discussed as tools to support clinical decision-making and precision rehabilitation by integrating large volumes of patient-specific data. Such approaches may enhance exercise prescription, progression, and long-term monitoring.
Talk nerdy to me
The study selection process was reported as following PRISMA guidelines, which generally improves transparency, validity, and reproducibility of literature identification and screening. Restricting inclusion to randomized controlled trials (RCTs) may enhance the overall level of evidence; however, the presence of an RCT design alone does not guarantee methodological rigor. No detailed appraisal or justification regarding study quality, risk of bias, or adequacy of control conditions was clearly reported, leaving open the possibility that poorly designed RCTs were included.
Despite the use of a PRISMA flow diagram, the number of included studies and the selection process remain unclear. The flowchart reports a total of nine studies included in the review, yet simultaneously indicates zero “new studies included” and zero studies included from a previous version of the review. This apparent contradiction may reflect a reporting issue rather than an actual methodological error; however, it creates confusion for the reader. While the stepwise identification, screening, and eligibility assessment is described, the final inclusion stage lacks clarity regarding the origin and classification of the included studies, undermining transparency.
Furthermore, the data extraction and synthesis methods are insufficiently described. The absence of a structured extraction framework raises concerns about selection and interpretation bias, as authors may have preferentially extracted information they deemed most relevant, rather than systematically representing the full scope of findings across studies. This limitation is particularly important in narrative reviews, where synthesis is inherently interpretive.
To strengthen rigor and reduce arbitrariness, the review could have employed a thematic literature analysis approach after study inclusion. Methods adapted from qualitative thematic analysis, such as the framework proposed by Braun and Clarke (2006), may be appropriate when transparently applied to literature synthesis. In this adapted approach, included studies are treated as textual data; meaningful units relevant to the review question are coded, codes are then grouped into higher-order themes, and themes are iteratively reviewed and refined. While this method does not eliminate subjectivity, it enhances analytic transparency, coherence, and traceability in narrative reviews, thereby improving methodological credibility.
Take-home messages
- Exercise therapy is the cornerstone of KOA management, improving pain, function, muscle strength, and quality of life—even without measurable structural cartilage changes (Physiotutors, Knee Osteoarthritis Overview).
- Structural changes are not required for clinical benefit: symptom and functional improvements often occur independently of MRI or radiographic findings.
- Individualized, progressively dosed mechanical loading is safe and effective; high-impact activities can be appropriate if tolerated and carefully monitored.
- Exercise prescription should follow a FITT framework (frequency, intensity, time, type) and be guided by patient function, symptoms, and response. A combination of aerobic, resistance, neuromuscular, balance, and mobility exercises provides the greatest benefit. Aquatic exercise can be used initially, transitioning to land-based exercises as tolerance improves (Physiotutors Video on KOA Exercise).
- Biopsychosocial factors are critical: kinesiophobia, catastrophizing, self-efficacy, and social support influence pain, adherence, and rehabilitation outcomes. Education, shared decision-making, and barrier identification are essential.
- Adjuncts such as weight management and dietary optimization may support symptom reduction and lower systemic inflammation.
- Despite strong evidence, many patients do not receive guideline-based conservative care, emphasizing the physiotherapist’s role in delivering evidence-informed, holistic rehabilitation (Physiotutors Insights on Hip and Knee OA).
Reference
Liu, H., Qin, L., Liu, Y. et al. Knee osteoarthritis rehabilitation: an integrated framework of exercise, nutrition, biomechanics, and physical therapist guidance—a narrative review. Eur J Med Res 30, 826 (2025). https://doi.org/10.1186/s40001-025-03083-4
THE ROLE OF THE VMO & QUADS IN PFP
Watch this FREE 2-PART VIDEO LECTURE by knee pain expert Claire Robertson who dissects the literature on the topic and how it impacts clinical practice.
