Research
Ankle/Foot
December 15, 2025
Is It Really Achilles Tendinopathy? Considering Posterior Ankle Impingement Syndrome

Introduction
Pain localized at the Achilles tendon insertion is frequently attributed to Achilles tendinopathy. However, patients who fail to respond to evidence-based interventions for tendinopathy may warrant evaluation for Posterior Ankle Impingement Syndrome as an important differential diagnosis. This narrative expert opinion review provides a comprehensive examination of Posterior Ankle Impingement Syndrome, including its anatomical basis, pathophysiology, clinical and differential diagnosis, diagnostic evaluation, and management strategies.
Posterior ankle impingement syndrome predominantly involves osseous structures, such as the posterolateral talar process or an os trigonum, although soft tissue involvement, including synovitis and posterior ligament pathology, is also frequently observed. In addition, the flexor hallucis longus (FHL) tendon may present with tendinopathic changes. A readily implementable clinical test for the diagnosis of posterior ankle impingement is also detailed within this review.
Methods
This article is a narrative expert-opinion review authored by a single clinician (J.-C. Moati) and published in a peer-reviewed journal. No methodological framework is described, including search strategy, study selection criteria, or critical appraisal of the literature. The content is therefore not based on a systematic or reproducible selection of available evidence but primarily reflects the author’s clinical experience and interpretation of selected references. Consequently, the overall level of evidence provided by this article is low.
Results
Anatomical Considerations
The posterior ankle compartment is delimited superiorly by the distal edge of the tibial epiphysis and inferiorly by the retro-talar calcaneal aspect.
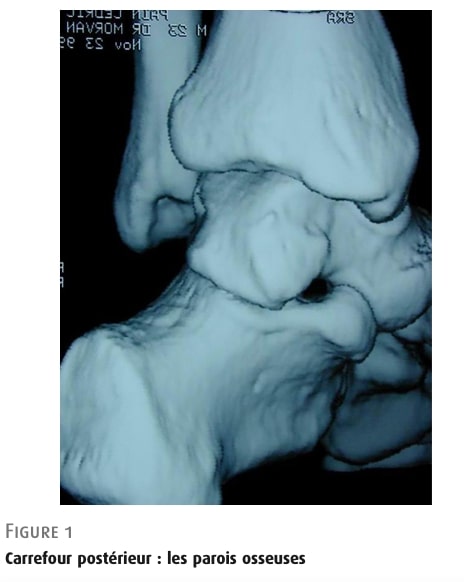
Figure 1
Posterior ankle compartment: osteology.
Posterior talar aspect
Between the posterior margin of the tibia and the calcaneus lies the posterior aspect of the talus, which can be more or less prominent (Figure 2). It has two posterior tubercles: a smaller postero-medial one and a larger postero-lateral one. The latter comes from the fusion of a secondary ossification center that appears between ages 8 and 13. Its size varies and it can be enlarged, sometimes exceeding 1 cm (Stieda process). Between the two tubercles is the intertubercular groove, where the Flexor Hallucis Longus (FHL) tendon runs.
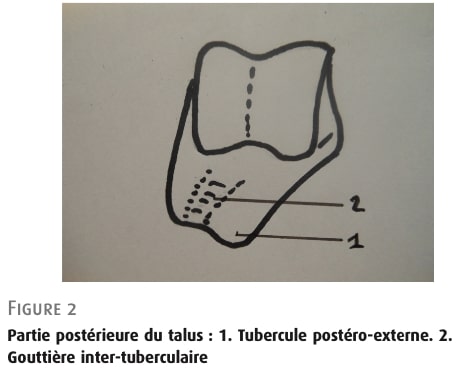
Figure 2: Posterior aspect of the talus: 1 Postero-lateral tubercule 2: Intertubercular groove
Trigonum bone
When the secondary ossification center of the talus fails to fuse an os trigonum is formed (Figure 3). This accessory bone is found in 8–13% of the population and is bilateral in just under 2% of cases. Its size varies but is usually under 1 cm; it may be bipartite or even fragmented. It articulates with the postero-lateral tubercle of the talus via a synchondrosis, and sometimes with the calcaneus on its inferior surface. Failure of fusion appears to be promoted by repeated micro-trauma in plantar flexion, which may explain its higher frequency in football players who started training in childhood.
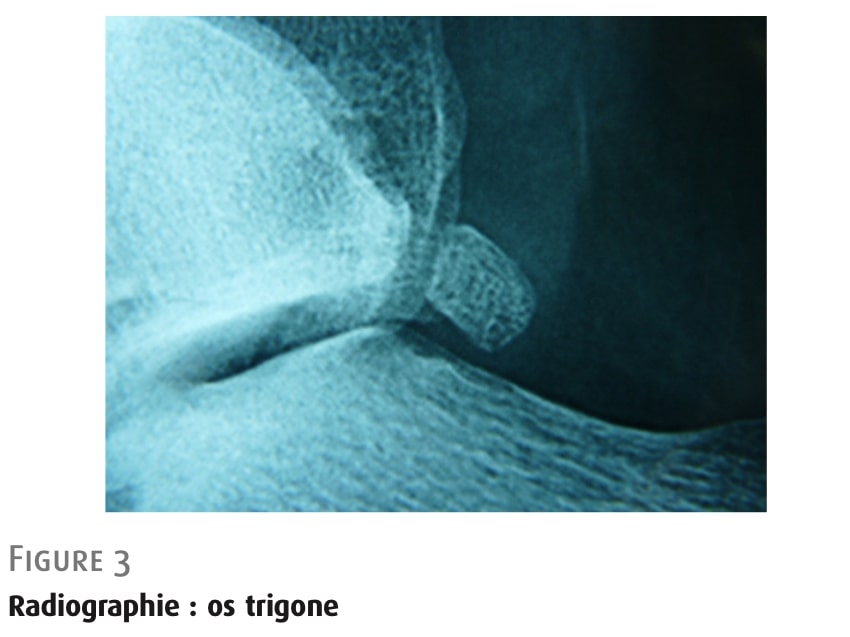
Figure 3: Trigonum bone.
Ligaments
Within the posterior ankle compartment lies the deep portion of the posterior-inferior tibiofibular ligament, the posterior talofibular ligament, running from the fibular malleolus to the postero-lateral tubercle of the talus and the posterior intermalleolar ligament: not present in all individuals. It extends from the fibular malleolus to the medial malleolus and may sometimes project toward the posterior talocrural recess
flexor hallucis longus (FHL) tendon
Surrounded by its synovial sheath, the tendon runs vertically through the tibial groove, then through the intertubercular groove, which is closed by the posterior annular ligament. It then changes direction, running downward and forward beneath the sustentaculum tali (Figure 4). Just medial to it lies the posterior tibial neurovascular bundle.
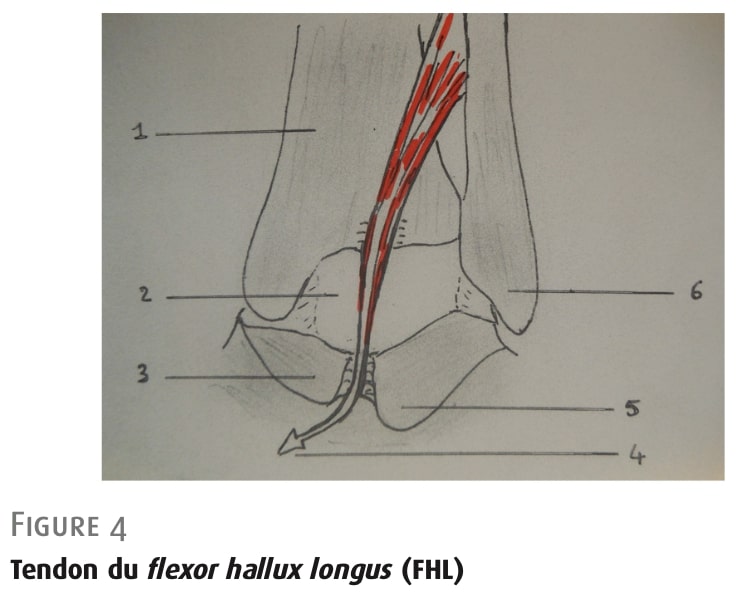
Figure 4: Flexor Hallucis Longus tendon.
Physiopathology
Acute mechanism of injury
- Macro traumatism: Reception on a plantar flexed foot.
The injuries are usually bony, caused by a posterior compression mechanism: a fracture of the postero-lateral tubercle (Shepherd’s fracture), more rarely of the postero-medial tubercle (Cedell’s fracture), or a fracture of an os trigonum.
Chronic mechanism of injury
- Micro traumatism: repetitive end-of-range plantar flexion.
Multiple structures within the posterior ankle complex are exposed to repetitive compression. Ballet dancers—who frequently work in extreme plantar flexion—as well as athletes such as runners and fencers are particularly prone to developing posterior ankle impingement syndrome.
Structural Sources of Pain
The impingement is most often bony, due to an elongated postero-lateral tubercle or the presence of an os trigonum.
It is less commonly soft-tissue or cartilaginous when no prominent bony structure is present:
- Tibio-talar impingement, with repeated contact between the posterior talus and the inferior margin of the tibia, leading to localized chondropathy.
- Compression of the posterior synovial recesses, which are often distended and hypertrophied—particularly in ballet dancers—resulting in significant synovitis.
- Compression of the posterior ligaments, causing thickening and secondary fibrosis. The posterior intermalleolar ligament, when present, is especially vulnerable.
- Flexor hallucis longus (FHL) tendon involvement, with tenosynovitis, sheath effusion, or even partial tears due to stenosis created by a thick intertubercular ligament. This occurs in more than 30% of bony impingements and may be promoted by a large os trigonum. Isolated FHL injury may also occur when low-lying muscle fibers impinge against the ligament.
- An accessory soleus muscle is usually asymptomatic, but may become problematic if excessively large.
Clinical Diagnosis
Subjective findings suggestive of posterior ankle impingement syndrome:
- Mechanism of injury.
- Progression: end-range pain has progressed to pain occurring at a lower degree of ankle plantarflexion.
- Presence of clicking/cracking.
- Previous ankle injuries.
Clinical examination:
- oedema
- posterior ankle impaction test.
According to the study authors, this test is more indicative of bony impingement. The test is considered positive if it reproduces the patient’s symptoms and can be performed using two different techniques:
Seated patient: The patient sits at the edge of the exam table with legs hanging and the knee flexed at 90°. The examiner forcefully plantarflexes the foot while the other hand stabilizes the heel.
Prone patient: The patient lies prone with the knee flexed at 90° and the foot is moved into plantarflexion in the same manner (Figure 5).
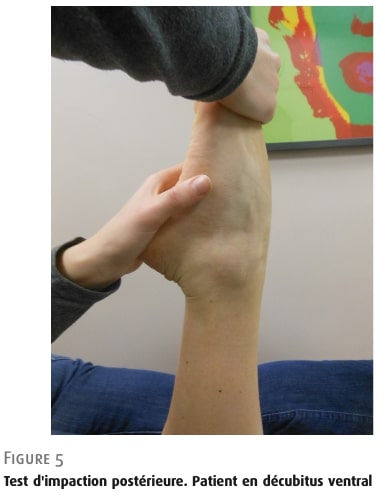
Figure 5: Posterior Impaction test. Patient prone lying position.
This Physiotutors’ video additionally presents a third technique.
- Reproduction of posterior ankle pain during ankle and hallux dorsiflexion with the knee extended, especially when combined with compression of the retro-malleolar region, may suggest FHL tendinopathy.
- Ankle range of motion assessment and the anterior drawer test of the talocrural joint may reproduce the patient’s symptoms due to compression.
- More advanced diagnostic techniques, such as local anesthetic (xylocaine) infiltration, can be used, with symptom relief during the posterior ankle impingement test helping to confirm the diagnosis.
Complementary exams
Complementary exams for posterior ankle impingement focus primarily on bone and soft tissue evaluation. Standard radiographs are essential to assess the postero-lateral tubercle, identify an os trigonum, and detect posterior subtalar osteoarthritis or ossifications. CT scans provide detailed bone imaging and 3D reconstructions, helping to distinguish an os trigonum from fractures or pseudarthrosis and to evaluate the posterior tibiotalar and subtalar joints. MRI assesses both bone and soft tissues, revealing bone edema, synovitis, posterior ligament or capsule thickening, and FHL tenosynovitis, as well as low-lying FHL muscle fibers. Ultrasound has limited use but can detect soft tissue lesions and rule out Achilles tendinopathy. Bone scintigraphy may show increased uptake in the posterior ankle and can be combined with CT for precise localization if needed.
Differential diagnosis
The main condition to rule out is posterior subtalar arthropathy, which can present with similar symptoms. It may coexist with an os trigonum or an enlarged posterior process, and failing to recognize it can lead to poor outcomes after bony excision; in such cases, bone scintigraphy combined with CT is particularly useful.
Achilles tendinopathy is another classic differential, usually diagnosed by painful palpation of the tendon and confirmed with ultrasound or MRI. Pre-Achilles bursitis can be more difficult to detect and may require imaging (ultrasound or MRI with injection). Calcaneal stress fractures may mimic posterior ankle impingement; lateral radiographs show a characteristic dense line perpendicular to trabeculae, with CT or MRI used for confirmation if needed.
For a more detailed discussion of differential diagnoses for posterior ankle pain, refer to Physiotutors’ review of this Delphi consensus study.
Treatment
Acute posterior ankle impingement syndrome
According to the study authors, fractures of the posterior talar process or an os trigonum require 4 to 6 weeks of immobilization.
Chronic posterior ankle impingement syndrome
Medical Management
For patients with marked or persistent pain, a brief immobilization period of 1 to 3 weeks using a brace or cast may be appropriate. Medical management also includes oral analgesics and anti-inflammatory drugs, along with cryotherapy and anti-inflammatory occlusive dressings. In most cases, a corticosteroid injection should be considered and may be repeated, particularly when soft tissues are involved.
Conservative Management
Rehabilitation, as described by Ledoux, focuses on restoring ankle range of motion and reducing muscular tightness, particularly through deep massage of the plantar flexor muscles. Physiotherapeutic modalities such as ultrasound can also be helpful. Gait retraining is essential, emphasizing heel control and proper foot rollover. Postural stretching of the relevant muscle chains is combined with strengthening of the quadriceps, gluteal muscles, and triceps surae. Proprioceptive training is crucial, especially when tibiotalar laxity is present. For athletes, adjustments to training conditions and load management should not be overlooked.
Surgical Management
If conservative management fails, surgical intervention may be considered. A precise identification of pain sources—based on the complementary examinations described above—is essential before proceeding. Arthroscopy is the preferred surgical technique. Postoperative care typically involves 4 to 6 weeks of relative rest before resuming regular activities, with a return to sports generally expected around 6 to 8 weeks.
Questions and thoughts
The reliance on a 1991 publication to inform conservative management highlights important methodological limitations. This article represents a narrative expert-opinion review rather than a systematic synthesis of the literature. As such, it does not follow a transparent or reproducible methodology for identifying or selecting sources, and its recommendations largely reflect the authors’ clinical experience. While this perspective can be valuable—particularly in encouraging clinicians to consider posterior ankle impingement in patients who fail to improve—it should be interpreted with caution.
In addition, the conservative management section relies on physiotherapy modalities that are now considered outdated. Clinical practice has evolved substantially over the past two decades, and interventions such as therapeutic ultrasound or deep friction massage are no longer regarded as first-line treatments for posterior ankle impingement syndrome, limiting the relevance of these recommendations in contemporary practice.
Although more recent studies provide additional insights into posterior ankle impingement syndrome, the overall body of evidence remains limited. A 2011 review focusing on conservative management in professional ballet dancers emphasizes an initial phase aimed at inflammation control through load reduction and avoidance of provocative movements, particularly plantarflexion. In this early phase, injections may be considered to reduce inflammation. Manual therapy may be used to restore ankle mobility, followed by activity-specific strategies to improve ankle stability. Given the association between impaired core stability and lower-limb injuries, individualized core-stability exercises are also recommended. Strength training should progress logically—from open to closed kinetic chain, general to sport-specific, and unloaded to loaded tasks—with the integration of jump training as appropriate. Notably, therapeutic ultrasound is not recommended.
Finally, it is important to recognize that much of the existing literature adopts a predominantly structural perspective, which may influence clinical reasoning. Patients should not be managed solely through the lens of their anatomical diagnosis, but rather within a broader, individualized biopsychosocial framework.
Talk Nerdy to me
While this article provides a comprehensive and clinically useful overview of posterior ankle impingement syndrome, its narrative expert-opinion design contrasts markedly with higher-level evidence frameworks. Unlike systematic reviews or meta-analyses, it does not follow a predefined methodology for literature identification, selection, or appraisal, limiting transparency and reproducibility. In contrast, systematic reviews aim to minimize author-dependent interpretation by using explicit search strategies, inclusion criteria, and risk-of-bias assessments.
Similarly, the article differs from randomized controlled trials (RCTs) and prospective cohort studies, which allow for causal inference and comparative evaluation of treatment effectiveness. Such designs provide quantifiable outcome data and enable assessment of intervention efficacy, whereas the present paper offers descriptive recommendations without comparative outcome measures.
It is also important to recognize that, given the nature of the subject addressed—namely clinical diagnosis, anatomy, pathophysiology, and both medical and conservative management—traditional research designs such as randomized controlled trials or prospective cohort studies may not always be appropriate or feasible. Many aspects of posterior ankle impingement syndrome rely on clinical reasoning, expert pattern recognition, and anatomical considerations that are difficult to standardize or isolate within experimental designs. In this context, narrative reviews can be a suitable format to synthesize clinical knowledge and translate expert experience into practical guidance.
However, the quality and reliability of narrative reviews can be substantially improved through more structured methodological approaches. Delphi consensus studies, for example, offer a robust alternative by combining expert clinical judgment with a transparent, reproducible framework. Through iterative rounds of expert input, predefined consensus thresholds, and grading of recommendations, Delphi methods help reduce individual author bias while strengthening the credibility and applicability of expert-derived conclusions.
Consequently, while the reviewed article is appropriate in format given the clinical nature of the topic, future work in this field would benefit from structured expert-consensus methodologies to enhance methodological rigor and clinical relevance.
Take-home messages
Think beyond Achilles tendinopathy
- Posterior ankle pain that does not improve with evidence-based Achilles tendinopathy management should prompt consideration of posterior ankle impingement syndrome.
Identify at-risk populations
- Common in athletes exposed to repeated or sustained end-range plantarflexion (e.g. ballet dancers, football players, runners, fencers).
- It can be related to both bony (os trigonum, enlarged posterior talar process) and soft-tissue structures.
Use targeted clinical assessment
- Progressive pain from end-range plantarflexion to earlier symptom onset is suggestive.
- A positive posterior ankle impingement test strongly supports the diagnosis.
- Pain reproduced with ankle and hallux motion plus retro-malleolar compression may indicate FHL involvement.
- Consider ankle instability and prior ankle sprains.
Guide imaging and referrals appropriately
- Persistent or unclear cases may require imaging (X-ray, CT, MRI) to identify bony and soft-tissue contributors.
Prioritize active, modern conservative management
- Initial focus on load management and avoidance of provocative plantarflexion.
- Restore ankle mobility and progressively develop ankle stability and strength.
- Progress rehabilitation logically (unloaded → loaded, general → activity-specific).
- Integrate core stability and jump training when appropriate.
- Passive modalities from older literature (e.g. ultrasound, deep tendon friction massage) should not be considered first-line.
Recognize when escalation is needed
- Failure of conservative care may warrant medical interventions (e.g. injection) or surgical opinion.
- Early recognition can prevent prolonged symptoms and inappropriate treatment pathways.
Reference
5 ESSENTIAL MOBILIZATION / MANIPULATION TECHNIQUES EVERY PHYSIO SHOULD MASTER
Learn 5 essential mobilization / manipulation techniques in 5 days that will skyrocket your manual therapy skills immediately – 100% For Free!