
Research
October 20, 2025
Exercise for Chronic Ankle Instability: Best Practices, Duration & Most Effective Techniques

Introduction
The ankle is the most frequently injured weight-bearing joint in the body, with ankle sprains being the most common injury type. These typically involve either the lateral ligament complex (especially the anterior talofibular ligament) or, the medial deltoid ligament complex. After an initial sprain, many individuals develop chronic ankle instability (CAI) — a condition marked by recurrent sprains, instability, pain, weakness, and limited range of motion as described in this physiotutors’ clinical pattern. Lateral ankle sprains account for about 73% of all ankle sprains, and inadequate rehabilitation after the first injury (reported in 50–70% of cases) is a major contributor to chronic instability.
Exercise for chronic ankle instability — including strength, balance, and proprioceptive training — is considered a cornerstone of rehabilitation and has proven benefits for various chronic conditions. Evidence shows it helps prevent recurrent ankle sprains; however, there is still uncertainty about which specific exercise components are most effective.
Recent studies have highlighted the positive effects of balance training in CAI. Still, existing meta-analyses have methodological limitations (e.g., overlapping control groups or inclusion of mixed exercise interventions), making it difficult to isolate the true effect of different exercise types. To address these gaps, the present meta-analysis aims to evaluate the overall effectiveness of exercise for chronic ankle instability and to compare the relative benefits of different exercise modalities. Importantly, all included control groups were true non-intervention conditions, ensuring cleaner comparisons and more reliable conclusions.
Methods
Search Strategy:
Four medical databases were searched. Only English-language RCTs were included. Eligible studies involved participants with chronic ankle instability (CAI), an exercise therapy intervention group, a no-intervention control group, and quantitative outcomes on ankle function (FAAM and SEBT).
Study Selection
Two reviewers independently screened all retrieved titles and abstracts. Studies that appeared relevant were read in full to determine eligibility based on predefined inclusion and exclusion criteria. Disagreements were resolved through discussion or by consulting a third reviewer.
Inclusion criteria
- Population: Participants explicitly diagnosed with chronic ankle instability (CAI).
- Intervention: The experimental group received exercise therapy (any structured rehabilitation, balance, or strengthening program).
- Control: The comparison group received no intervention (no exercise, placebo, or standard care without structured exercise).
- Outcomes: Studies provided quantitative data assessing ankle function using validated measures — specifically the Foot and Ankle Ability Measure (FAAM) and/or the Star Excursion Balance Test (SEBT).
- Study Design: Only randomized controlled trials (RCTs) were included to ensure high-quality evidence.
Exclusion criteria
- Participants with acute ankle injuries or non-chronic instability conditions.
- Non-original studies such as abstracts, conference proceedings, editorials, expert opinions, reviews, case reports, or laboratory-based studies.
- Non-English publications or articles lacking full text.
Outcome Measures
- Functional performance: Foot and Ankle Ability Measure – A self-reported ankle instability questionnaire consisting of two parts: Activities of Daily Living (FAAM-ADL) and Sports (FAAM-S). The FAAM is scored from 0 to 100%, with higher results corresponding to greater function.
- Dynamic balance: Star Excursion Balance Test (SEBT) across eight directions anterior (A), antero-medial (AM), antero-lateral (AL), medial (M), lateral (L), posterior (P), postero-medial (PM), postero-lateral (PL).
Data Extraction
Two reviewers independently extracted study characteristics and outcome data using a standardized form. Studies were grouped into:
- Exercise therapy group (intervention)
- Blank control group (no intervention)
All outcomes were continuous variables. For outcomes using the same units, mean difference (MD) and 95% confidence interval (CI) were calculated; otherwise, standardized mean difference (SMD) was used. Authors were contacted when key numerical data (mean or SD) were missing.
Risk of Bias and Quality Assessment
Methodological quality was assessed using the Cochrane Risk of Bias Tool (RoB 2). The GRADE framework (via GRADE Profiler 3.0) was used to rate the overall strength of evidence for main outcomes as High, Moderate, Low, or Very Low.
Statistical analyses
Results were expressed as mean difference (MD) or standardized mean difference (SMD) with 95% confidence intervals (CI).
Heterogeneity—the degree of variation between study results—was assessed using the I² statistic. If variation was low (I² < 50%), a fixed-effects model was used; if high (I² ≥ 50%), a random-effects model was chosen to account for differences among studies.
To test the stability of results, a sensitivity analysis was performed by removing individual studies to see if outcomes changed. When enough data were available (≥10 studies), subgroup and meta-regression analyses explored factors that might explain result differences (e.g., exercise type or study quality). Funnel plots were used to check for publication bias. Statistical significance was set at p < 0.05.
Results
Study selection
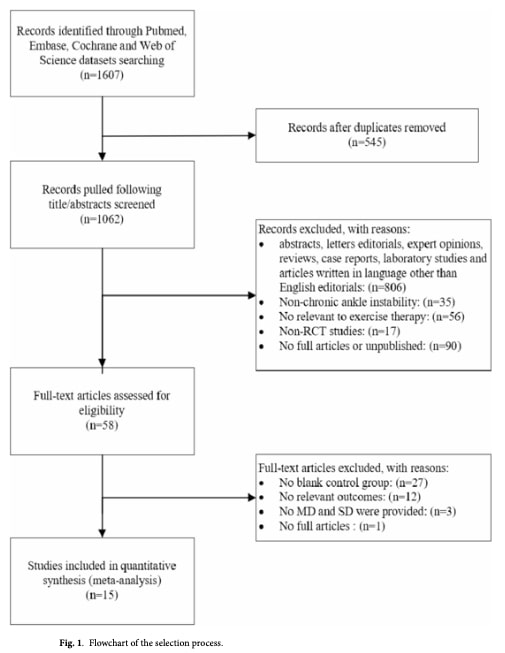
From 1,607 records initially identified, 1,062 remained after removing duplicates. After title, abstract, and full-text screening, 16 studies met the inclusion criteria and were included in the meta-analysis.
Risk of bias assessment
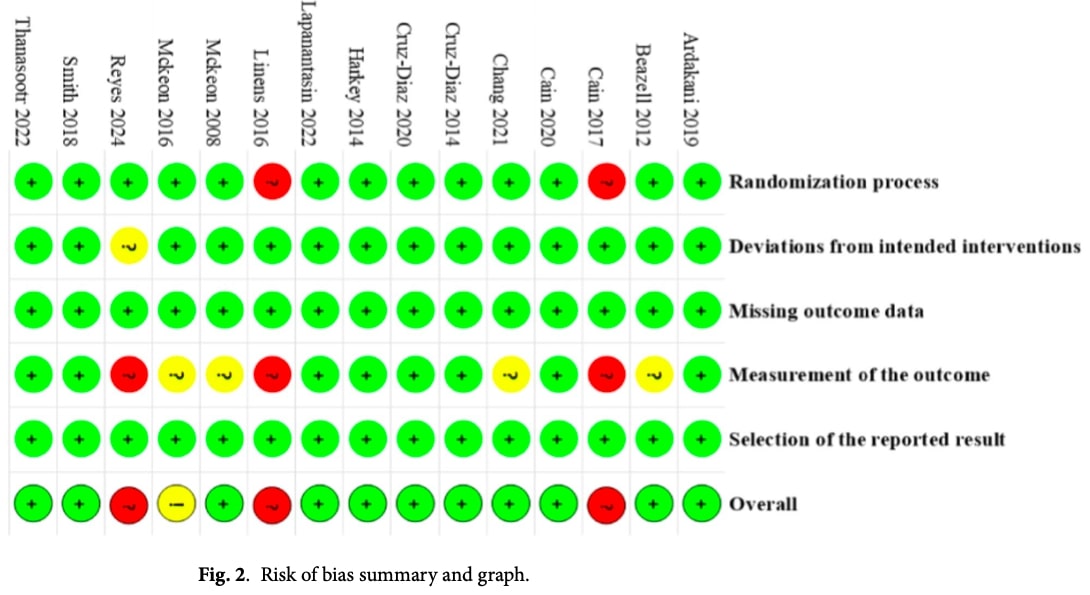
Overall, the included studies showed generally good methodological quality, as assessed with the Cochrane RoB 2 tool. Most trials reported clear randomization methods, appropriate intervention procedures, and complete outcome data. However, a few studies had unclear randomization processes or lack of blinding of outcome assessors, which introduced some risk of bias.
In total, 11 studies were rated as low risk, one raised some concerns, and three were considered high risk. A detailed breakdown of bias across each domain is presented in Figure 2.
Meta-analysis results – FAAM
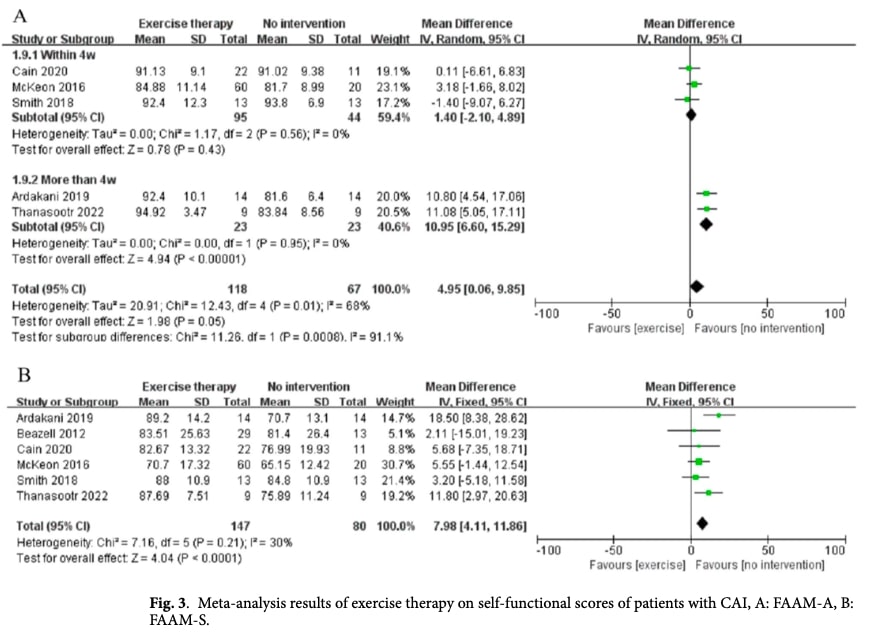
Six studies investigated the impact of exercise for chronic ankle instability on self-reported functional assessment in patients with chronic ankle instability, using the Foot and Ankle Ability Measure (FAAM) for both the Activities of Daily Living (FAAM-ADL) and Sports (FAAM-Sports) subscales.
The meta-analysis showed that exercise for chronic ankle instability therapy significantly improved self-reported ankle function on both measures. Initial analyses revealed high heterogeneity (I2= 68%)among studies for FAAM-ADL, but further sub-grouping investigation indicated that intervention duration was a key factor — programs lasting longer than four weeks produced more consistent and superior improvements compared to shorter interventions. Detailed results and subgroup analyses are presented in Figure 3.
Meta-analysis Results – Dynamic Balance (SEBT)
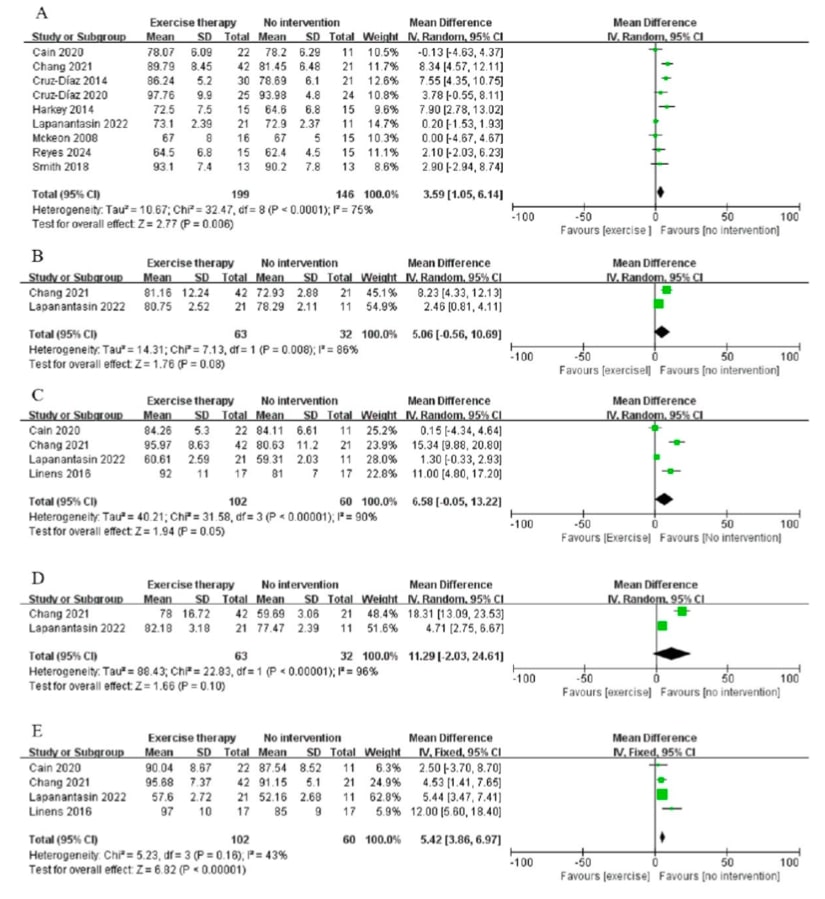
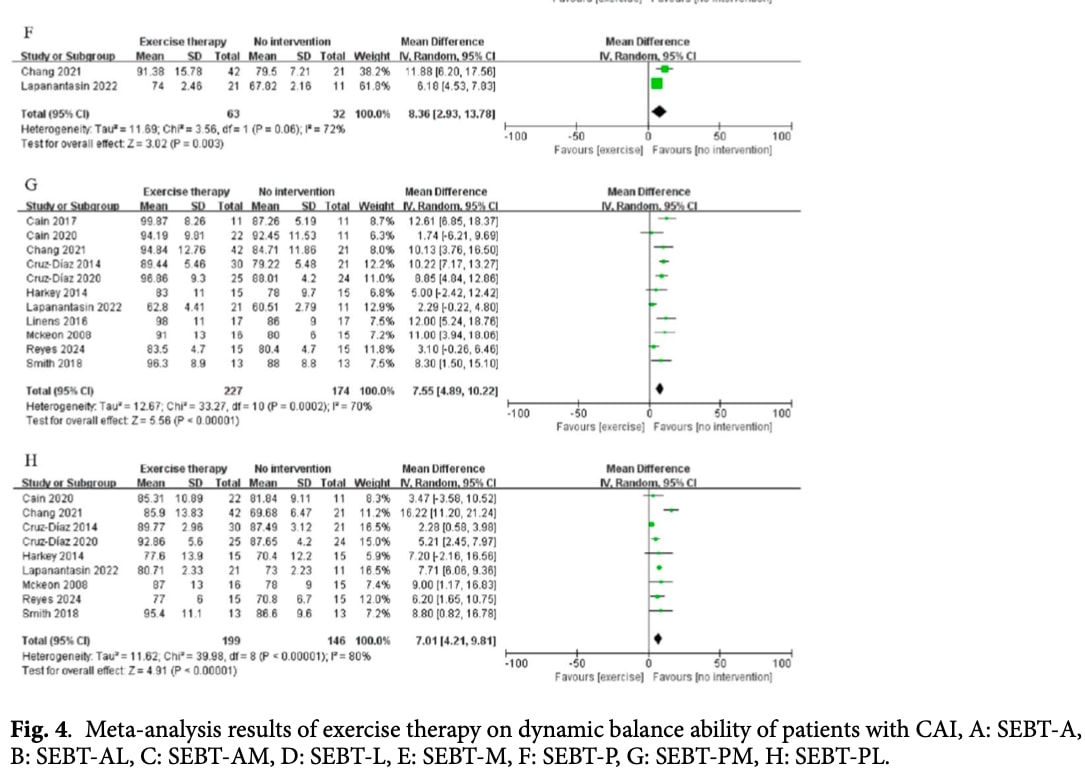
Eleven studies evaluated the effects of exercise for chronic ankle instability on dynamic balance in patients with chronic ankle instability using the Star Excursion Balance Test (SEBT) across the eight directions.
Overall, exercise therapy led to significant improvements in most SEBT directions, showing that such programs effectively enhance balance control and postural stability. However, no significant differences were found in the anterolateral and lateral directions. Interestingly, after removing two studies for sensitivity analysis purposes, the results for SEBT anteromedial direction became non-significant.
Although high heterogeneity existed between studies, the benefits of exercise therapy remained consistent, particularly in the anterior, posteromedial, and posterolateral directions. Sensitivity analyses confirmed that the positive effects persisted even when individual studies were excluded.
Further subgroup and meta-regression analyses were conducted to investigate the source of heterogeneity. Three subgroups were defined: intervention duration (< or >4 weeks), exercise type (proprioception, strengthening, neuromuscular activation or joint mobilization) and country. Detailed results and subgroup comparisons are presented in Figure 4.
Meta-regression and Subgroup Analysis Results
Meta-regression analysis was conducted to explore potential sources of variation between studies. No significant subgroup differences were identified (p > 0.05), suggesting that the observed heterogeneity was not explained by study-level factors such as country, intervention duration, or exercise type. Because most studies originated from the United States, country-based comparisons were considered less meaningful.
Subgroup analyses focused on intervention duration and exercise type. The findings indicated that programs lasting longer than four weeks produced more consistent and greater improvements in dynamic balance (SEBT A, PL and PM) compared to shorter interventions. Shorter programs (≤4 weeks) showed benefits only for SEBT PM and PL directions.
Overall, these results suggest that longer exercise interventions are more effective for improving balance in patients with chronic ankle instability, although results should be interpreted cautiously due to remaining heterogeneity.
Sensitivity Analysis of Intervention Period Subgroups
Because the subgroup analyses still showed high heterogeneity, a sensitivity analysis was performed by removing individual studies one at a time. The results showed that heterogeneity dropped substantially — or even disappeared — after excluding certain studies. Specifically, removing Cruz-Diaz et al. (2014) eliminated variability in SEBT-PL (≤4
weeks), and removing Chang et al. (2021) did the same for SEBT-A and SEBT-PL (>4 weeks). Excluding Lapanantasin et al. (2022) reduced heterogeneity in SEBT-PM and SEBT-PL (≤4 weeks), while removing Reyes et al. eliminated heterogeneity in SEBT-PM (>4 weeks).
Exercise Type Subgroup Analysis
Strength training significantly enhanced SEBT performance in the posteromedial and posterolateral directions, while proprioceptive training produced similar benefits. Joint mobilization improved balance across anterior, posteromedial and posterolateral directions.
Neuromuscular activation exercises, such as whole-body vibration training, led to moderate improvements, particularly in the PL direction, though results were less consistent across studies. Proprioceptive training also led to notable improvements in SEBT-PM and SEBT-PL
A sensitivity analysis showed that removing certain studies (notably those by Chang et al. and Lapanantasin et al.) reduced heterogeneity without changing the overall findings. This suggests that while the type of exercise contributes to variability, the overall conclusions remain robust. However, the effects of neuromuscular activation on SEBT outcomes should be interpreted with caution due to inconsistent evidence.
Efficacy Validation of Exercise Therapy
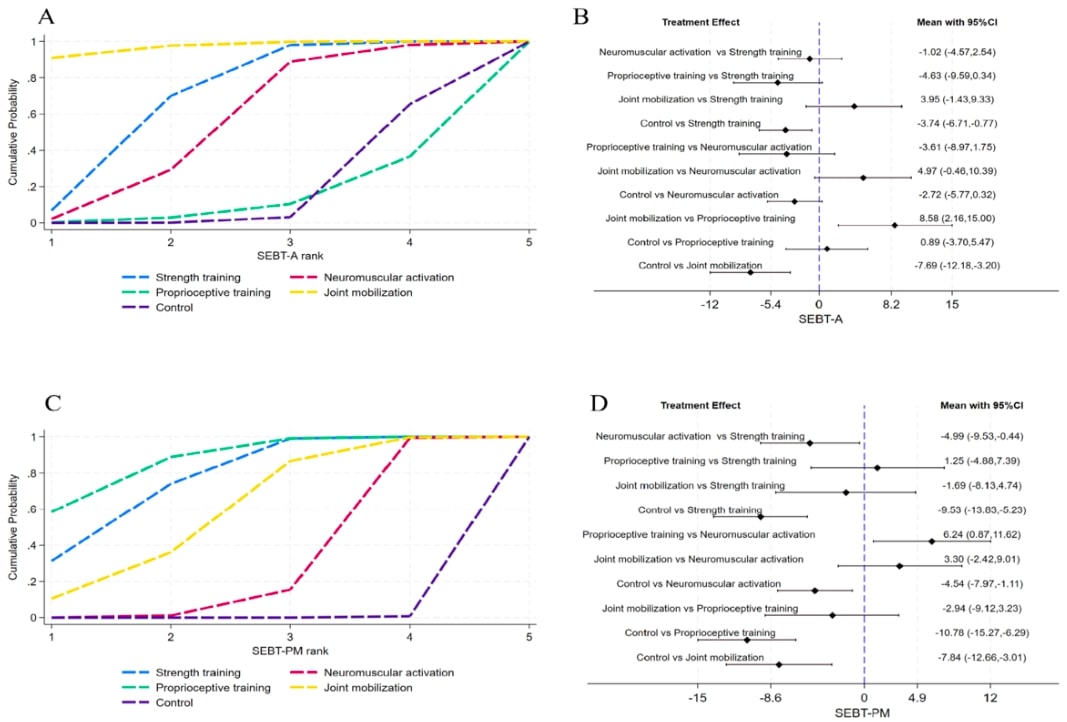
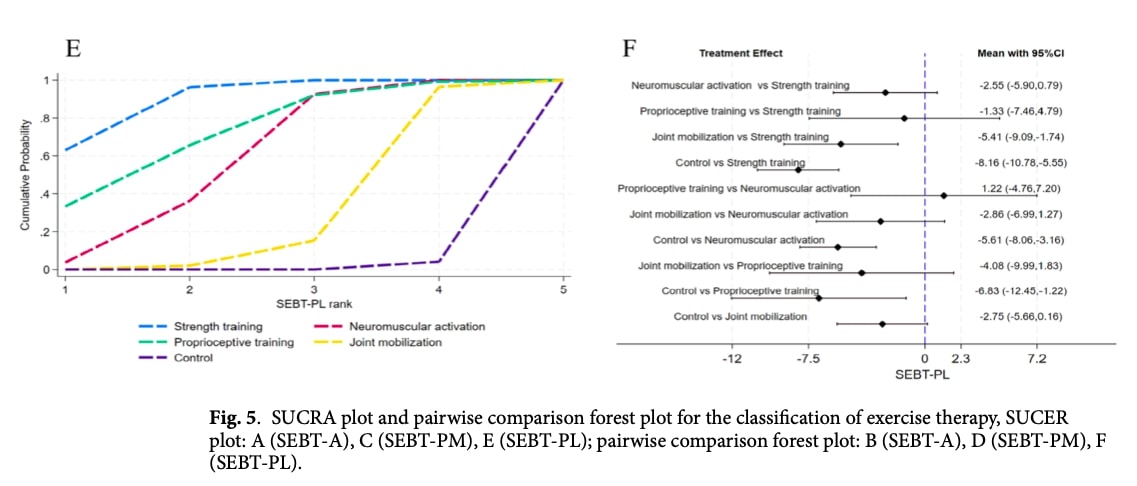
To compare the relative effectiveness of different exercise types, indirect comparisons were made using the control group as a common reference. Indirect comparisons were conducted for studies including SEBT-A, SEBT-PM and SEBT-PL. Surface Under the Cumulative Ranking Curve, and pairwise comparison forest plot are displayed in Figure 5 and will be further discussed in the Talk nerdy to me section.
The results, illustrated in Figure 5, show that:
- For SEBT-A (anterior direction), joint mobilization was the most effective, followed by strength training, both showing significant improvements compared to the control group.
- For SEBT-PM (posteromedial direction), strength training and proprioceptive training produced the greatest improvements, significantly outperforming other exercise types.
- For SEBT-PL (posterolateral direction), strength training again showed the best results, followed by proprioceptive and neuromuscular training.
Overall, these findings suggest that joint mobilization is most effective for improving anterior balance, while strength and proprioceptive training yield the greatest benefits for posterior balance stability in individuals with chronic ankle instability.
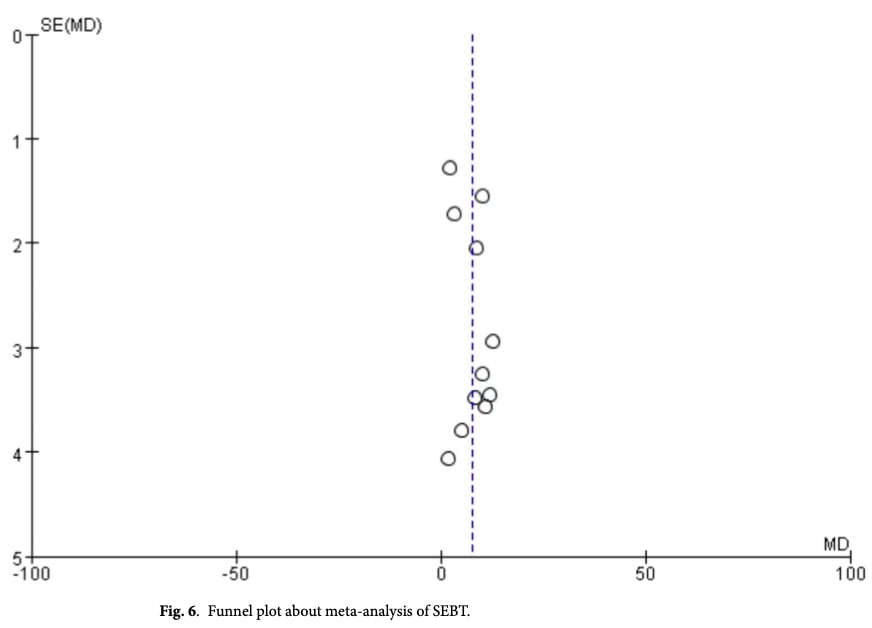
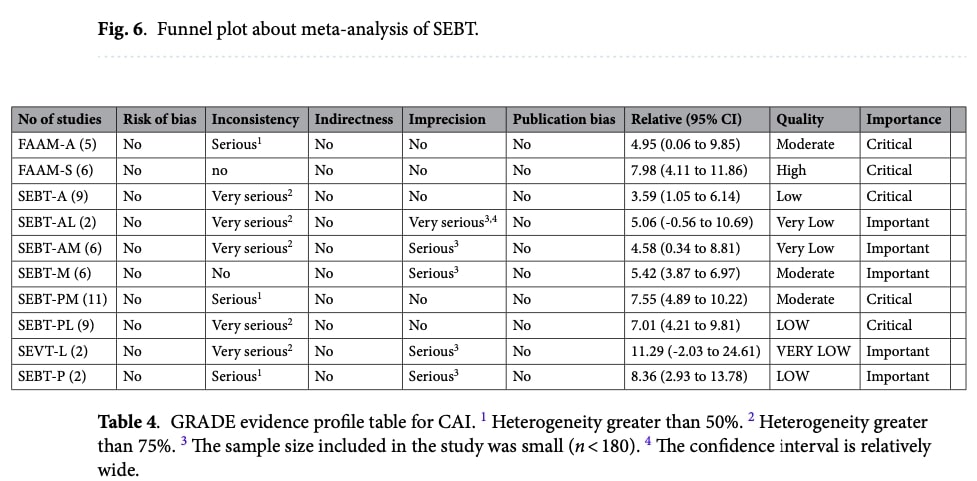
Publication Bias and Quality of Evidence
A funnel plot analysis was performed for SEBT outcomes (see Figure 6). The plot showed a generally symmetrical distribution, suggesting that publication bias was minimal.
Using the GRADE approach (see Table 4), the overall quality of evidence across all outcomes was rated as low to very low, mainly due to high heterogeneity among studies and small sample sizes.
Questions and thoughts
The authors do not specify how chronic ankle instability (CAI) was defined in the included studies. Criteria such as chronicity or clinical features required for CAI diagnosis are not described, which may have contributed to heterogeneity in participant characteristics and influenced the results.
While the FAAM and SEBT are valuable tools for assessing functional improvement in patients with CAI, they may not fully capture the overall effectiveness of exercise for chronic ankle instability. Including outcomes such as strength or the recurrence rate of ankle sprains would have provided a more comprehensive picture of long-term efficacy. Reporting odds ratios for recurrence could also have strengthened the interpretation of exercise effectiveness. Overall, the scope feels somewhat limited for evaluating rehabilitation success.
Regarding the comparison of exercise modalities, it is debatable whether isolating interventions—such as strength, neuromuscular, or proprioceptive training—reflects real-world clinical practice. These elements are often integrated rather than applied independently. Future studies should focus on structured, individualized rehabilitation programs that target specific deficits and follow objective-led progression, rather than comparing single exercise types against generic protocols.
Finally, one methodological limitation of this meta-analysis lies in its design: since the control groups received no intervention, participants and assessors could not be blinded, which introduces a potential performance and detection bias.
Talk nerdy to me
In Figures 3 and 4, the forest plots may appear slightly misleading at first glance, as most of the green boxes (representing each study’s mean difference) are positioned on the “Favours no intervention” side. However, this does not indicate that no intervention was superior for FAAM-S or SEBT outcomes. The apparent reversal likely arises from the way the mean difference was calculated — using the formula (intervention group mean – control group mean). As a result, positive values represent greater improvement in the exercise group, even though they are displayed on the “Favours no intervention” side of the graph.
To compare the different exercise interventions with each other, the authors used the Surface Under the Cumulative Ranking Curve (SUCRA) analysis. This approach is commonly applied in network meta-analyses to rank several interventions based on their relative efficacy, even when not all have been directly compared in individual studies. The SUCRA value, displayed in Figure 5, represents the probability that a treatment is among the most effective options, with larger areas indicating greater effectiveness. This method helps visualize which exercise type performs best across all available evidence for SEBT–A, SEBT–PM, and SEBT–PL outcomes.
In Panel A, which shows the results for SEBT–A, the SUCRA plot (left) and the pairwise comparison forest plot (right) together illustrate the relative performance of each exercise type. The SUCRA curves indicate that joint mobilization had the highest probability of being the most effective intervention for improving SEBT–A scores, followed by strength training, while neuromuscular activation, proprioceptive training, and control ranked lower. In the forest plot, a positive mean difference (MD) means the first intervention achieved higher SEBT–A values than the second, whereas a negative MD favors the second intervention. Confidence intervals (CIs) that do not cross zero indicate statistically significant differences. For example, joint mobilization vs proprioceptive training (MD = +8.58, 95% CI: 2.16–15.00) significantly favors joint mobilization, confirming its superior efficacy. In contrast, neuromuscular activation vs strength training (MD = –1.02, 95% CI: –4.57–2.54) shows no significant difference between these two interventions.
Take Home messages
- Exercise therapy works. Structured exercise programs significantly improve self-reported function (FAAM) and dynamic balance (SEBT) in patients with chronic ankle instability (CAI), confirming its central role in rehabilitation.
- Program duration matters. Interventions lasting more than four weeks produce greater and more consistent improvements, particularly in the posterior balance directions (posteromedial and posterolateral).
- Exercise type influences outcomes.
- Strength and proprioceptive training are most effective for enhancing posterior stability.
- Joint mobilization shows superior effects on anterior balance.
- Combine, don’t isolate. In clinical practice, integrating multiple exercise components—strength, proprioception, neuromuscular control, and joint mobility—may yield the most functional benefits.
- Evidence quality is low to very low, largely due to small samples and methodological differences, but the overall direction of findings strongly supports active rehabilitation over no intervention.
Clinical takeaway:For managing Chronic Ankle Instability, implement multi-modal exercise for chronic ankle instability of 4+ weeks duration. Key components include strength, proprioception, and mobilization to achieve the primary goals: restoring balance, reducing recurrence rates, and enhancing long-term functional outcomes. Dive deeper into the rationale with this Physiotutors podcast on ankle sprain management
Reference
THE ROLE OF THE VMO & QUADS IN PFP
Watch this FREE 2-PART VIDEO LECTURE by knee pain expert Claire Robertson who dissects the literature on the topic and how it impacts clinical practice.
