
Research
Education & Career
July 10, 2025
Shared Decision Making in Physiotherapy for Shoulder Pain: The Gap Between Theory and Practice

Introduction
Shoulder issues and pathologies are often challenging to diagnose and manage due to unreliable clinical examinations, unclear prognostics, and a lack of strong treatment guidelines. While some treatment modalities—such as exercise therapy—demonstrate better outcomes than passive approaches for RC related shoulder symptoms (for a review on RC related pain click here) no specific exercises have been definitively established as superior, and patient responses can vary significantly. This uncertainty complicates clinical decision-making, leaving physiotherapists without a clear path when managing shoulder conditions.
Shared decision making in physiotherapy is a patient-centered approach that incorporates patients’ preferences, values, and expectations into their care plan. Given the ambiguity in shoulder treatment recommendations, this collaborative method could play a crucial role in optimizing outcomes. Despite its potential benefits and patient demand for greater involvement in care decisions, shared decision making is not yet widely implemented in physiotherapy practice.
This study explores how physiotherapists integrate shared decision making in physiotherapy when managing shoulder conditions. By reviewing current practices and evidence, we aim to highlight the importance of this approach in enhancing patient-centered care.
Methods
This cross-sectional observational study evaluated clinical interactions at a single time point. Initial physiotherapy consultations in primary care were recorded and analyzed to assess the integration of shared decision making in physiotherapy.
Participants
- Physiotherapists: Licensed practitioners working in Dutch primary care were recruited via convenience sampling, primarily through the authors’ university affiliations and professional networks. Convenience sampling from academic/professional networks may bias results by over-representing physiotherapists predisposed to shared decision-making.
- Patients: Adults (>18 years) presenting with shoulder-related symptoms, including pain or dysfunction localized to the neck, scapular region, pectoralis area, or proximal arm (distal boundary: elbow). Eligible participants had to communicate independently to ensure meaningful engagement in shared decision making in physiotherapy.
To minimize bias, neither physiotherapists nor patients were informed of the specific components under investigation during consultations.
Data collection
Each participating physiotherapist was asked to record up to six initial consultations. The sample size was determined based on the Observer OPTION-5 tool (a validated measure for assessing shared decision-making in clinical encounters) to ensure sufficient statistical power for regression analyses. This approach allowed the researchers to identify potential correlations between shared decision making in physiotherapy and other variables.
Consultations were audio-recorded using a digital Dictaphone. Physiotherapists also documented patient demographics (e.g., age, sex), clinical characteristics (duration of shoulder symptoms), and referral patterns (direct access or physician-referred). Additionally, therapist-level data—including years of experience, education level, age, and sex—were collected for analysis.
Rationale for Variables
The selection of these variables was grounded in empirical evidence highlighting how shared decision making in physiotherapy is shaped by multiple factors. Clinician-related variables (such as experience and training) and patient-related factors (including education level and symptom chronicity) are known to influence collaborative decision-making. Referral pathways (e.g., self-referred vs. physician-directed) were also considered, as prior research suggests they may affect communication dynamics during consultations.
Outcome Variables
The primary outcome was the level of shared decision making in physiotherapy, evaluated using the OPTION-5 scale. This validated and reliable tool assesses clinician performance across five key domains of shared decision-making: (1) justifying deliberative work, (2) justifying deliberative work as a team, (3) informing patients, describing options, and exchanging views, (4) eliciting preferences, and (5) integrating preferences into the care plan. Each item is scored on a 5-point Likert scale (0 = no effort, 4 = exemplary effort), with total scores summed to a maximum of 20. For interpretability, raw scores were rescaled to a 0–100 range.
Rater Training and Reliability
Three researchers underwent standardized training in OPTION-5 scoring to ensure intra-rater reliability. Training included iterative scoring of practice consultations using illustrative quotes until an intraclass correlation coefficient (ICC) >0.6 was achieved.
Calibration Process
To further refine consistency, the researchers independently scored 12 physiotherapy consultations across three rounds:
- Round 1: 3 consultations (ICC = 0.25)
- Round 2: 4 consultations (ICC = 0.50)
- Round 3: 5 consultations (ICC = 0.92)
Once the group exceeded the pre-specified ICC threshold of 0.6 in the third round, the remaining audio recordings were scored by a single assessor to maintain efficiency without compromising reliability.
The data analysis will further be discussed in the Talk nerdy to me section.
Results
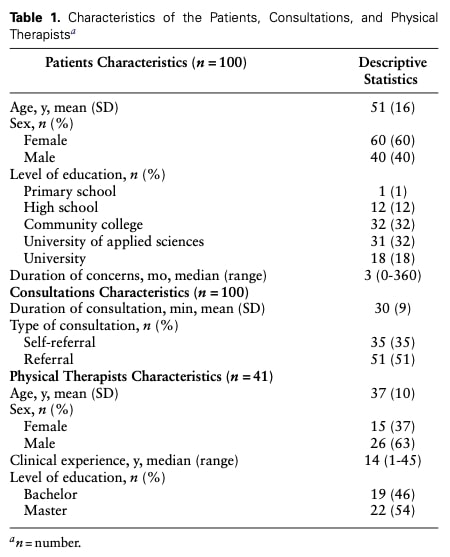
A total of 100 initial physiotherapy consultations were retained for analysis. These consultations involved 41 physiotherapists, with individual contributions ranging from 1 to 6 recorded sessions per clinician. Patients and physiotherapist characteristics are presented in the following table 1.
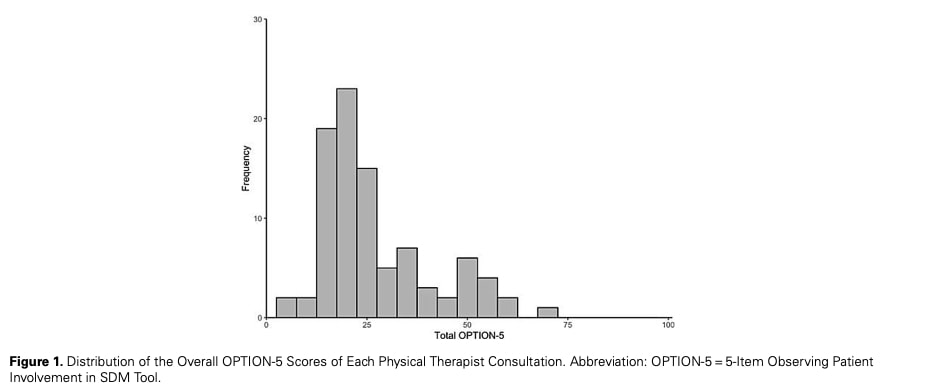
The mean OPTION-5 score across all consultations was 27/100 ranging from 5 to 70 (see the Figure 1), indicating limited implementation of shared decision-making principles in routine practice. As illustrated in the Figure 2, score distributions revealed that:
- A score of 1 (minimal effort) was most frequently assigned across all five items
- No consultations received an exemplary score (4) on any item, highlighting an absence of best-practice demonstrations
Characteristics Associated with the level of SDM.
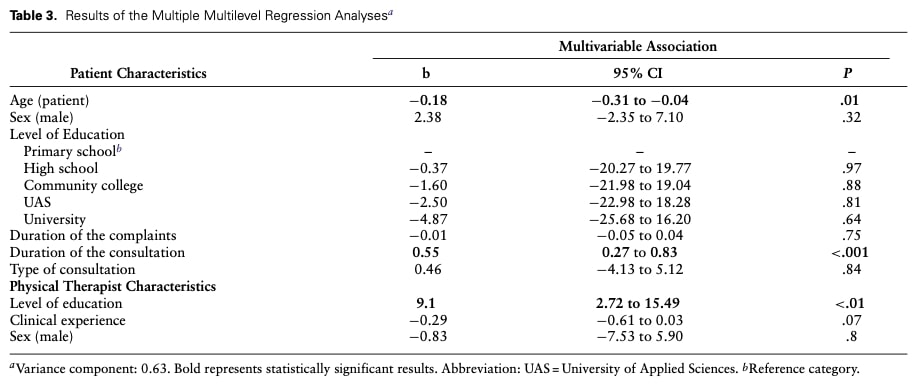
Multilevel regression analysis revealed three significant predictors of higher OPTION-5 scores (*p* < .05):
- Clinician Education Physical therapists with master’s-level education demonstrated substantially greater shared decision-making implementation(*b* = 9.1, 95% CI [2.7, 15.4])
- Consultation Duration Longer sessions were associated with improved shared decision-making performance(*b* = 5.5, 95% CI [2.7, 8.3])
- Patient Age Older patients received more shared decision-making engagement(*b* = -1.8, 95% CI [-3.1, -0.4])
Questions and thoughts
The study reveals suboptimal implementation of shared decision-making in physiotherapy practice, as evidenced by the mean OPTION-5 score of 27/100 indicating limited adherence to shared decision-making principles.
A closer examination of specific shared decision-making elements through Table 2 reveals nuanced patterns. The discussion of treatment options (Item 1) emerged as the relatively strongest area, though still suboptimal, with 74% of therapists demonstrating minimal effort and 22% showing moderate effort in presenting alternatives. More troubling was the finding that 65% of therapists made only minimal attempts to establish true collaborative partnerships (Item 2)—a fundamental shared decision-making requirement that demands recognizing patients as experts in their lived experience of their condition through egalitarian engagement.
Particularly alarming were the results for core shared decision-making components: one-third of therapists (33%) made no effort whatsoever to explain treatment pros and cons or verify patient understanding (Item 3), while similarly, 33% showed no effort and 43% only minimal effort to explore patient preferences, expectations or concerns about discussed treatments (Item 4). These findings align with our prior systematic review examining reassurance practices for low back pain patients, which similarly identified clinicians’ limited engagement with patient concerns. For a comprehensive analysis, see our previous publication.
These findings highlight a significant disconnect between shared decision-making theory and current practice, particularly interesting in the context of shoulder pain management where the authors argue shared decision-making could prove especially valuable given the condition’s diagnostic and therapeutic complexities. However, this perspective requires careful consideration against existing evidence showing superiority of active over passive treatments for shoulder pain, alongside improved diagnostic accuracy through standardized assessment protocols.
This tension raises crucial questions about shared decision-making ‘s true nature and implementation. Importantly, shared decision-making should not be misconstrued as simply deferring decisions to patients or abandoning clinical expertise. As the OPTION-5 tool clarifies, effective shared decision-making represents a sophisticated clinical skill that: deliberately integrates patient expertise about their symptoms with professional knowledge; employs specific communication techniques like teach-back and active listening; and cultivates genuinely collaborative relationships through both verbal and nonverbal engagement. For additional guidance on enhancing clinical communication, we recommend reviewing this Physiotutors resource on patient-centered care.
While this study did not examine the relationship between shared decision-making and clinical outcomes, the stark gap between patient preferences for collaborative care and current practice realities underscores two critical needs moving forward. First, rigorous outcome research must establish whether and how shared decision-making influences treatment results in musculoskeletal care. Second, the field requires targeted training interventions to help clinicians develop competencies that move beyond superficial information-sharing toward authentic shared decision-making.
Talk nerdy to me
The study combined descriptive and inferential statistical methods to systematically evaluate shared decision-making practices in physiotherapy consultations. Researchers first characterized the study population by summarizing key demographic and clinical variables: categorical data as frequencies with percentages, and continuous measures as either mean ± standard deviation (for normally distributed variables) or median and range (for non-normal distributions).
Shared decision-making implementation was quantitatively assessed using the validated OPTION-5 instrument. Researchers reported both composite scores (mean and range across all consultations) and item-level performance (frequency distributions for each of the five OPTION-5 items). This dual approach enabled comprehensive evaluation of where shared decision-making processes were most and least effectively implemented during clinical encounters.
Given the hierarchical nature of the data – with multiple patient consultations nested within individual therapists – the analysis required specialized multilevel linear regression techniques. This advanced methodology addresses three fundamental limitations of conventional regression when applied to clustered data:
- It properly accounts for non-independence among consultations conducted by the same clinician
- It distinguishes between therapist-level effects (e.g., professional education) and patient-level factors (e.g., age or symptom duration)
- It generates more precise estimates of predictor effects by modeling the nested data structure explicitly
The final regression model incorporated all relevant patient and therapist characteristics simultaneously, with results presented as:
- Regression coefficients (b) representing the magnitude of effect on OPTION-5 scores
- 95% confidence intervals indicating estimate precision
- p-values assessing statistical significance against an α threshold of 0.05
This analytical framework provides distinct advantages for understanding shared decision-making in clinical practice. Unlike standard regression that assumes independence among all observations, multilevel modeling acknowledges the reality that therapists develop consistent practice patterns affecting multiple patients. The approach thus yields findings that more authentically reflect the complexities of real-world therapeutic relationships and decision-making processes.
Take-home messages
Shared decision making Matters, But It’s Underused
- Your colleagues averaged only 27/100 on shared decision-making implementation (OPTION-5). Prioritize discussing treatment options, eliciting preferences, and building collaborative partnerships.
Focus on These Critical Gaps
- 33% of therapists skipped explaining pros/cons of treatments.
- 65% made minimal effort to partner with patients as equals.
Start with simple steps: Ask (“What matters most to you?”), Share (“Here’s what we could do…”), Decide Together.
Master’s-Level Training Helped
- Therapists with advanced education (master’s degree) scored 9 points higher on OPTION-5 scale. Consider targeted shared decision-making training (e.g., motivational interviewing, preference elicitation).
- You can further consult this blog article providing greater insights in shared decision making.
Bottom line: shared decision-making isn’t about surrendering expertise—it’s about blending your clinical knowledge with the patient’s lived experience to achieve better outcomes.
Reference
Learn to Treat the Most Common Cause of Vertigo in This FREE Mini-Video-Series
Leading Vestibular Rehabilitation Expert Firat Kesgin takes you on a 3-Day Video Course on how to recognize, assess and treat posterior canal Benign-Paroxysmal Positional Vertigo (BPPV)
