Research
Diagnosis & Imaging
March 6, 2026
Neurogenic Thoracic Outlet Syndrome: Assessment, Rehabilitation and Clinical Reasoning Identified by a Scoping Review

Introduksjon
Neurogenic thoracic outlet syndrome, despite being more frequent than vascular thoracic outlet syndrome, is a relatively rare condition. With an incidence of 2 to 3 cases per 100.000 people per year, the chances of having neurogenic thoracic outlet syndrome are far less than that of having cervical radicular syndrome, for example. Despite being quite rare, we should be able to have this condition in the back of our minds as a differential diagnosis when a patient presents with pain, sensory and motor abnormalities, despite cervical radicular syndrome provocation tests being negative.
As the condition is rare, so is the literature. Despite rehabilitation being recommended as the standard of care, the components and details of such interventions are poorly described, leading to an evidence base of low-quality, as was concluded in a 2014 Cochrane Review. Therefore, the current scoping review aims to update the field
Metoder
A scoping review was conducted with the aim of identifying and describing the assessment and rehabilitation components of neurogenic thoracic outlet syndrome and to give insight into the clinical reasoning behind the strategies identified.
Eligible studies were literature reviews, systematic reviews, Cochrane reviews, primary empirical studies, treatment guidelines, and clinical commentaries. Studies included participants aged 16 years and older. When the studies investigated management strategies, it had to be part of conservative or pre-operative care. Postoperative care studies were not eligible for this scoping review. Studies had to be published in English and from the year 2000. Studies that included patients with arterial or venous thoracic outlet syndrome were excluded.
Resultater
A total of 29 studies were included in this scoping review. The most common study types included were literature/narrative reviews or expert opinion pieces (n=13), followed by: prospective studies (n = 4), randomised controlled trials (RCT), retrospective analysis and consensus studies (all n = 3), case reports (n = 2), and one cross-sectional study.
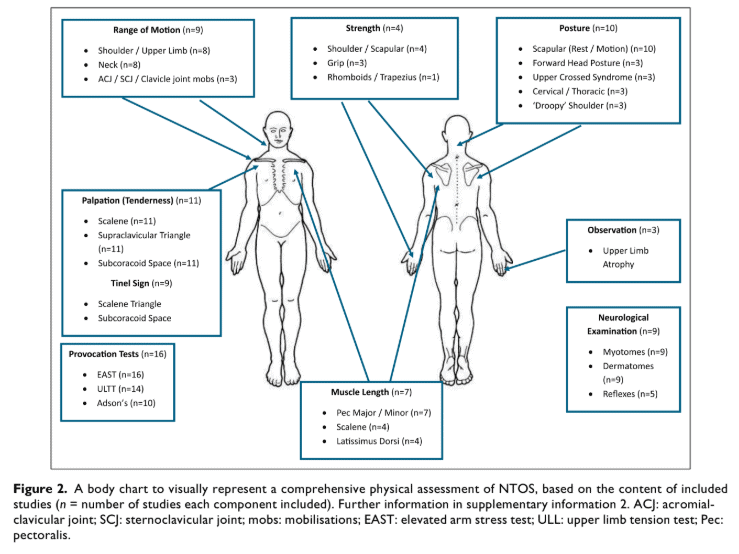
Physical assessment
Sixteen out of 18 studies (89%) described neurogenic thoracic outlet syndrome provocation tests:
- Roos/EAST (89%)
- ULTT (77%) was described, but not which one
- Adson’s Test (56%)
Eleven studies (61%) described palpation of the pectoralis muscles and the scalene muscles, and the supraclavicular space and the subcoracoid space as the methods of diagnosing the condition. Ten studies (56%) described posture and scapulothoracic assessment.
Only in three studies was the mobility of the first rib evaluated, and in one study, a glance was given to breathing assessment.
Rehabilitation components
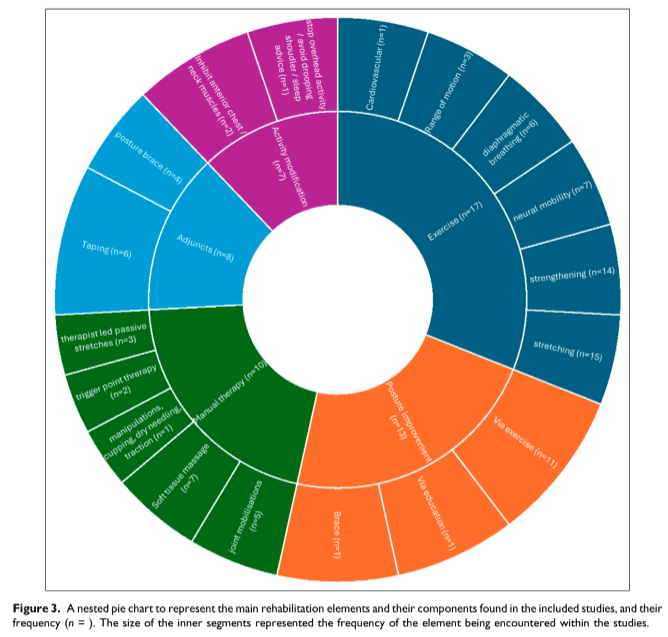
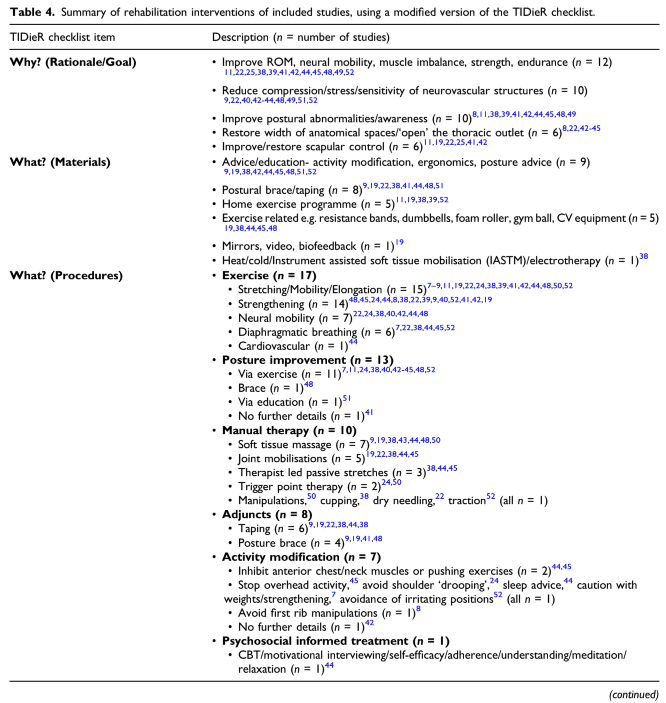
Most of the included studies describing rehabilitation interventions (17/19) included exercise as a core element. Stretching (n = 15), strengthening (n = 14), neural mobility (n = 7), and diaphragmatic breathing (n = 6) were the most prevalent exercise components encountered. Additional rehabilitation interventions were: ‘Posture Improvement’ (n =13), ‘Manual Therapy’ (n = 10), ‘Adjuncts’ (n = 8), such as taping or braces, and advice on ‘Activity Modification’ (n = 7). Only one study proposed using a ‘Psychosocial informed treatment’.
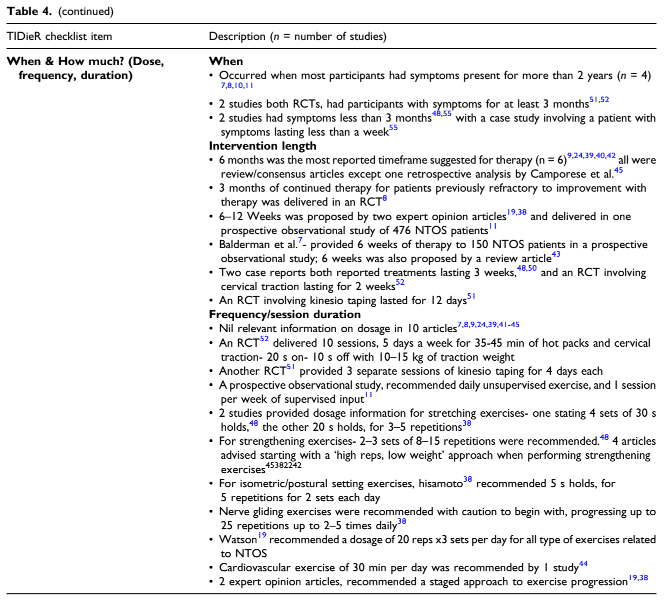
Information on intervention frequency, duration, and dosage was sparsely described within the included studies, with nil relevant information on dosage in 10 articles. When describing strengthening exercises for NTOS, a ‘high repetition, low weight’ approach was suggested in four studies.
The Scalene and Pectoral muscles (n = 10) were the most frequently mentioned in descriptions of stretching exercises. Scapular Stabilisation (n =9) was the most common feature of strengthening exercises, followed by mid-lower Trapezius and Serratus Anterior (n = 5). Minimal detail for neural mobility exercises other than ‘upper limb neural glides’ (n = 6) was provided, and no further details concerning diaphragmatic breathing exercises were provided by any of the six studies.
Clinical reasoning
Some studies gave insight into clinical reasoning. Considering the prognosis, two studies of the same author identified significant differences between the patients who improved with rehabilitation alone (31%) and those who did not (69%). Those who improved had less tenderness on palpation, less positive clinical diagnostic criteria (CDC) signs, less severe Cervical Brachial Symptom Questionnaire (CBSQ) and Short Form 12 (SF-12) physical component scores and could tolerate a longer EAST test before failure. Two studies proposed that lasting lifestyle interventions and postural modifications and having a sedentary job were positive prognostic factors for response to rehabilitation. On the other hand, obesity, depression, previous upper limb trauma and chronicity of symptoms were negative prognostic factors.
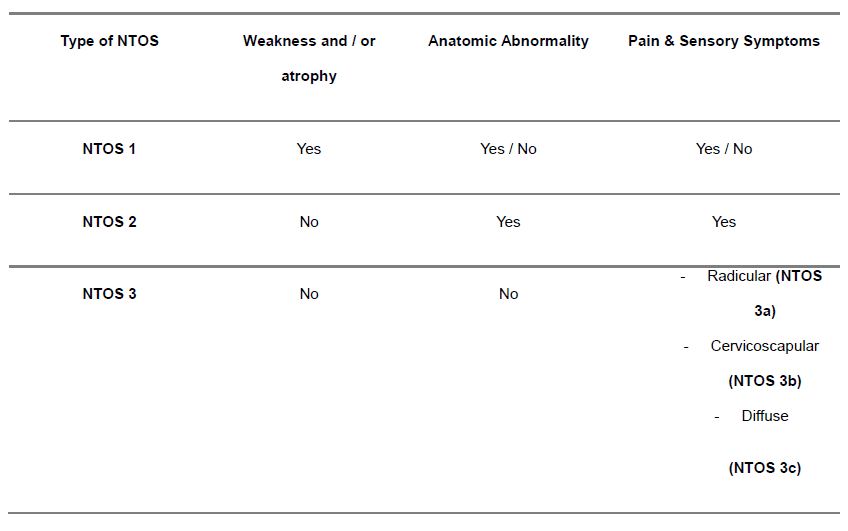
Regarding management decisions, a subclassification of neurogenic thoracic outlet syndrome was proposed by a consensus study by the members of the European Association of Neurosurgical Societies (EANS). This subclassification can guide rehabilitation decisions. According to this consensus, patients with atrophy and objective weakness (NTOS 1) should be referred for urgent assessment for potential surgery. Participants with no weakness and or atrophy (NTOS 2 and 3a) can be directed towards conservative management, and only in case of non-response to conservative care, surgical intervention can be considered. Those with cervicoscapular (NTOS 3b) or diffuse (NTOS 3c) should only progress to surgery in rare circumstances.
Another consensus study, by the International Neurogenic Thoracic Outlet Syndrome (INTOS) Hand Surgery workgroup proposed 3 to 6 months of conservative care for all NTOS patients, except for those with objective weakness and atrophy (NTOS 1).
Diagnose
As a secondary aim, the review wanted to find out how the diagnosis of neurogenic thoracic outlet syndrome was established in the included studies. Sixteen out of 29 studies (55%) discussed the diagnosis. Nine out of 16 (56%) studies quoted the Society of Vascular Surgeons clinical diagnostic criteria or the Consortium of Research and Education on Thoracic Outlet Syndrome (CORE-TOS) clinical diagnostic criteria, or both. Other studies were less explicit but mentioned combinations of the EAST, ULTT, and Adson’s tests, with the absence of other, more likely diagnoses.
One study described the most prevalent elements of the CORE-TOS clinical diagnostic criteria found within their study (n = 150 patients). Elements encountered in more than 90% of patients included: pain (99%), symptoms exacerbated by elevation (97%), tenderness to palpation of the scalene triangle/subcoracoid space (96%), numbness, paraesthesia or weakness in the arm and/or hand (94%), and a positive EAST test (94%). The least prevalent positive elements were a history of previous clavicle/first rib fracture or presence of a cervical rib (8%), previous cervical or peripheral nerve surgery (20%), previous treatment for ipsilateral TOS (21%) and weak handgrip/hand intrinsic atrophy (23%).
Two consensus studies emphasized the importance of patient history and clinical examination, along with arm symptoms referring to the C8/T1 distribution.
Measurements
67% of studies used the QuickDASH, 44% the Cervical Brachial Symptom Questionnaire (CBSQ), and one third of studies referred to the Short-Form 12 (SF-12). The TOS Disability score, the Pain Catastrophizing Scale, and the Zung Self-Rating Depression score were each reported twice.
Four studies objectified grip strength, isokinetic shoulder rotator strength, changes in range of motion, or tenderness to palpation.
Spørsmål og tanker
Clinical Reasoning strategies were “assessed on merit subjectively” by the lead author and discussed with the second reviewer, based on their own clinical experience of managing NTOS. This might involve subjectivity and clinical bias that have influenced the synthesis and tabulation of the clinical reasoning findings.
Nevertheless, that is the issue with scoping reviews. As a scoping review is a type of research synthesis that aims to map the available evidence on a broad topic or question, it is often used as a preliminary step to a more focused systematic review or to clarify a concept. While it is appropriate for mapping the current therapy management of NTOS and identifying existing literature gaps, it does not evaluate intervention effectiveness (as a systematic review would). By adhering to the PRISMA-SCR guidelines and using the Joanna Briggs Institute methodology for scoping reviews, the rigor and transparency of the search strategy were enhanced.
The current literature was assessed from 2000 to date, but 22 studies were published since 2020. Much of the literature elaborates on the assessment, and while crucial to effectively diagnose neurogenic thoracic outlet syndrome, the evidence base on rehabilitation strategies remains sparse. Further, a biomedical emphasis is apparent, with only one study discussing “psychosocial informed treatment”, while all other studies describe more mechanistic views of “decompression of the neurovascular structures” and “opening” the thoracic outlet.
The clinical reasoning identified in the included studies was often inconsistent. For example, some studies cautioned against the use of neural mobility and resistance exercises for fear of exacerbating symptoms, despite both featuring prominently in most rehabilitation descriptions. Another example is the application of manual therapy to the first rib, which was encouraged in five studies but excluded from a rehabilitation package in an RCT, as they felt it may aggravate pain. These are two inconsistencies, but there were more than exemplified here. The identified weaknesses in rehabilitation increase the importance of more research around this topic, especially in how to effectively rehabilitate the condition.
Snakk nerdete til meg
A limitation of a scoping review is the absence of a quality or risk of bias assessment. Yet, the use of the TIDieR checklist (Template for Intervention Description and Replication) is a strength. This validated tool helps to extract consistent and detailed information about intervention components, which is crucial when trying to understand how rehabilitation was performed across different studies.
Another limitation of this scoping review is that the TIDieR checklist revealed a generally poor description of the rehabilitation components in terms of dosage and frequency, which further complicates the already complex rehabilitation. As most of the studies were literature/narrative reviews or expert opinion pieces (n=13), the evidence is mostly of low quality, and the authors already mentioned excluding a large number of studies due to insufficient detail on rehabilitation parameters. This further emphasizes the challenge in summarizing reproducible therapy programs.
A striking finding is the use of therapy approaches for “lengthening” the pectoral and scalene muscles, but re-assessment is rarely the case. The authors also describe that the assessment of muscle length is rarely conducted in an objective or reproducible manner, further questioning the relevance of these assessments.
Ta med hjem meldinger
This review confirms that the conservative management of NTOS, primarily through physical therapy, revolves around a core set of components, but the literature is very vague on the specifics. The main goal of treatment identified in this scoping review is to create more space for the nerves and blood vessels in the thoracic outlet. Therapists widely use a combination of specific exercises—stretching the tight muscles in the front of the neck and chest, and strengthening the muscles that stabilize the shoulder blade. They also incorporate hands-on therapy, posture work, and advice on modifying aggravating activities. Despite the theoretical plausibility of these approaches, a lack of retest and re-evaluation is identified. Only one study highlights the importance of psychosocially informed treatment, calling for more psychosocial-based approaches to support mere biomedical reasoning strategies.
Referanse
21 AV DE MEST NYTTIGE ORTOPEDISKE TESTENE I KLINISK PRAKSIS
Vi har samlet en 100 % gratis e-bok som inneholder 21 av de mest nyttige ortopediske testene per kroppsregion, garantert for å hjelpe deg med å få en riktig diagnose i dag!