Research
Education & Career
July 24, 2025
Các chỉ số đánh giá thành tích của vận động viên chuyển giới: Nghiên cứu cắt ngang về sức mạnh và khả năng tim phổi

Giới thiệu
Transgender individuals are those whose gender identity differs from the sex assigned to them at birth. For example, a transgender man is someone who was assigned female at birth but identifies as male. In recent years, the participation of transgender athletes in competitive sports has raised important discussions, particularly around testosterone levels, which are traditionally associated with athletic performance. While the inclusion of transgender men in sports is generally less contested, the participation of transgender women continues to be debated, especially in relation to perceived physiological advantages.
As physiotherapists—experts in movement, rehabilitation, and physical performance— we have a role to play in shaping inclusive health practices, contributing to sport policy development, and ensuring equitable access to training and competition. Moreover, given that transgender individuals often face discrimination and barriers in healthcare, it is essential for clinicians to deepen their understanding of the unique challenges this population encounters.
This article review offers preliminary evidence on transgender athlete performance metrics, as well as the implications for their participation in sports.
Phương pháp
Study design
This cross-sectional study took place in a laboratory at the University of Brighton’s School of Applied Sciences in the UK. Participants completed laboratory testing in a single visit.
Recruitment
The study recruited 75 participants, consisting of 19 cisgender men (men identifying to their assigned sex at birth), 12 transgender men, 23 transgender women, and 21 cisgender women. Recruitment was conducted through social media advertising.
Participants and eligibility criteria
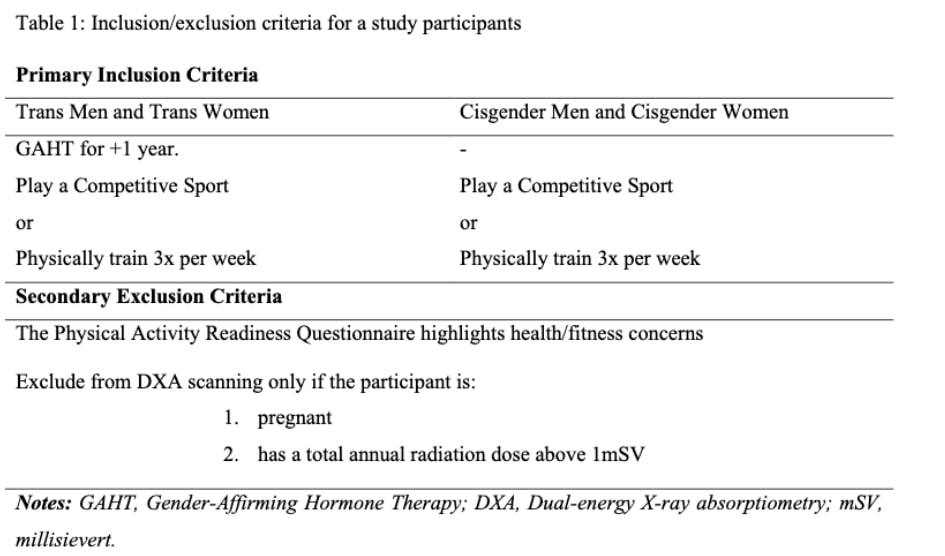
Full inclusion/exclusion criteria are detailed in the table 1. Three participants (two cisgender women and one transgender man) were excluded for missing blood samples. Additionally, two transgender women and one cisgender woman were excluded due to testosterone levels exceeding the female reference threshold (2.7 nmol/L).
Laboratory assessment
The study used two blood sampling methods:
- Finger-prick test – A quick capillary blood sample measured hemoglobin (Hb).
- Venous blood draw – A single 10 mL blood sample was taken from the arm fortestosterone and estradiol analysis.
Body composition
The study measured participants’ body mass using first bio impedance device while they were lightly clothed, representing clothed body mass. Body composition and bone mass were assessed via DXA scanning. A single researcher performed all participant positioning and scanning to ensure consistency. Body mass index (BMI), fat mass index (FMI), and fat-free mass index (FFMI) were then calculated.
Lung function
The study evaluated lung function as part of its assessment of transgender athlete performance metrics, using standardized spirometry protocols. Participants performed flow-volume-loop spirometry to measure forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), and peak expiratory flow. The FEV1/FVC ratio was calculated to evaluate potential obstructive lung patterns.
Strength assessment
The study assessed grip strength using a calibrated hand dynamometer. Prior to testing, hand size was measured at the metacarpophalangeal joints to account for potential anthropometric influences. Participants performed three consecutive trials per hand in an alternating left-right sequence to allow adequate recovery between efforts. The average of these three trials for each hand was used as the final strength measure.
Lower body power
Lower body power, a key component of transgender athlete performance metrics, was assessed through countermovement jumps using a validated jump mat system. Participants completed the test with hands maintained on their hips and a controlled countermovement not exceeding 45 degrees of knee flexion to ensure movement standardization. Three valid trials were recorded, with the average score used for analysis.
Cardiopulmonary exercise testing
The study assessed maximal aerobic capacity (VO2max) using a standardized treadmill protocol with metabolic gas analysis. Participants performed an incremental exercise test on a motorized treadmill using a validated ramp protocol. To ensure test validity, only participants achieving a respiratory exchange ratio ≥1.1 (indicating maximal effort) were included in the final analysis. This resulted in the exclusion of three participants (one cisgender man and two cisgender women) from the dataset.
Statistical analysis
The statistical methods used align with standardized guidelines and will be further discussed in the Talk Nerdy to Me section.
Kết quả
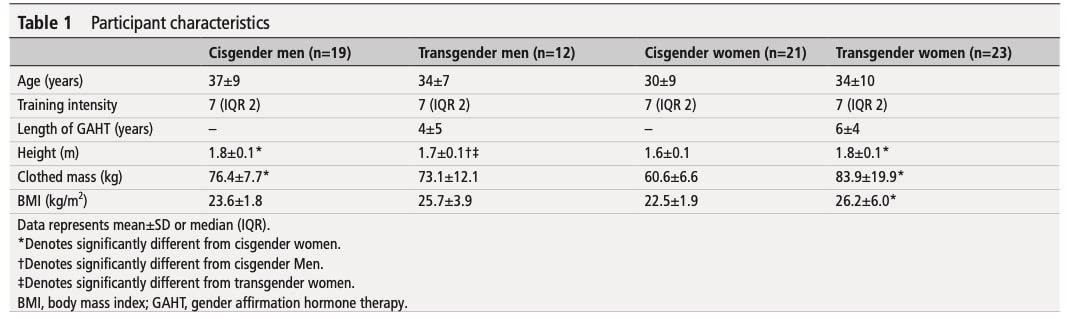
The research encompassed different athletes from different sports specialties, endurance sport represented 36% team sport 26% and power sports representing 38% of the total cohort. None of the participants were competing at national or international levels. As shown in Table 1, no significant differences were found in participant age, duration of gender-affirming hormone therapy, or training intensity scores
Participants characteristics
Regarding height, significant difference were found, cisgender men tends to be taller than transgender men, transgender women were also taller than cisgender women. Significant differences were also found in clothed mass, transgender woman were found to be more heavier than woman. Finally, BMI was also significantly different between the transgender woman and cisgender woman, with transgender woman having a significant higher BMI.
Blood measures
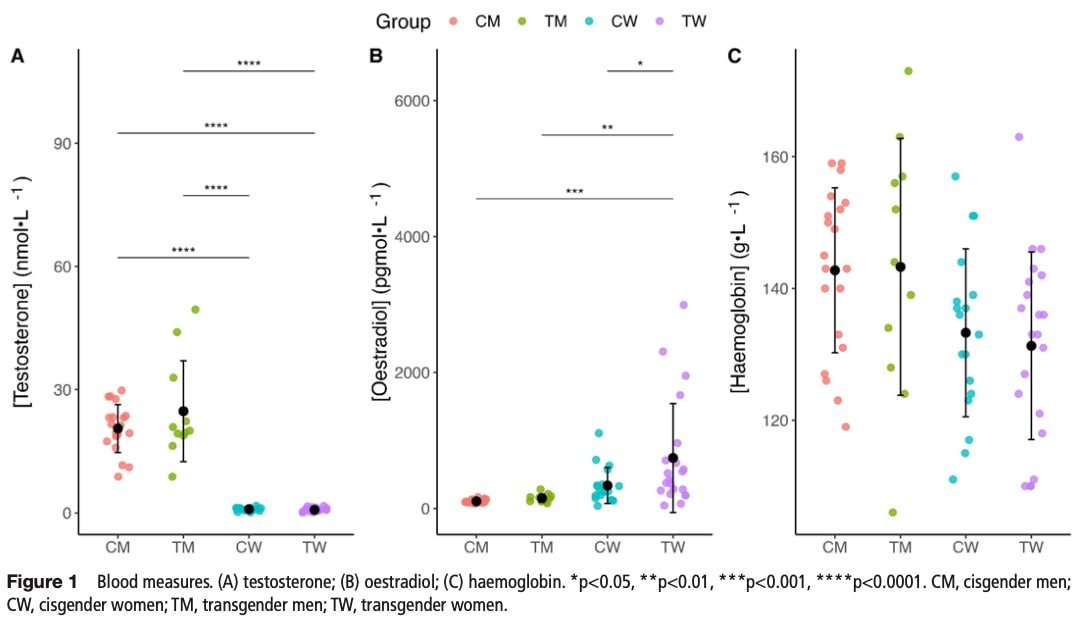
- Testosterone:
- Cisgender men had significantly higher levels than transgender women.
- Transgender men exceeded both transgender women and cisgender women.
- Estradiol:
- Transgender women showed higher levels than all other groups.
Clinical targets
Transgender women exhibited testosterone levels (0.7 nmol/L) within recommended GAHT guidelines (≤1.8 nmol/L), though their estradiol concentrations surpassed typical targets (400-600 pmol/L). Meanwhile, transgender men showed testosterone levels (24.8 nmol/L) that exceeded NHS clinical thresholds (15-20 nmol/L) but remained within the wider therapeutic range (11-34.7 nmol/L) established by the Endocrine Society.
Hemoglobin
Post hoc tests revealed no significant pairwise differences between groups.
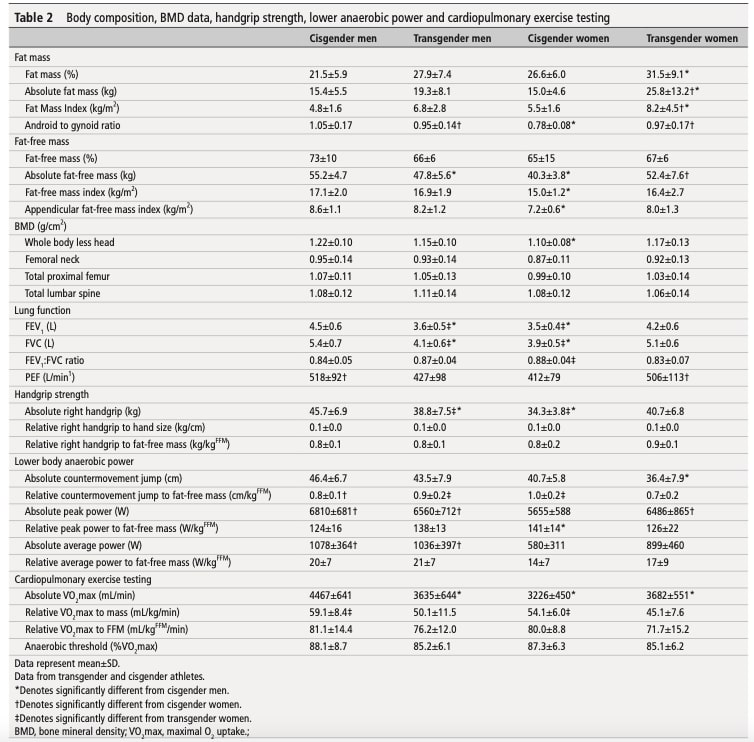
DXA assessment
Significant gender-based differences emerged in body composition: cisgender men showed lower percentage fat mass than transgender women, while transgender women exhibited higher absolute fat mass than both cisgender men and women. Fat Mass Index (FMI) followed a similar pattern, with transgender women surpassing cisgender men and women. Android-to-gynoid fat ratio analysis revealed cisgender women had a lower ratio than both transgender men and women.
Fat-free mass
This indicator represents the sum of all non-fat body components including muscles, bones, and connective tissues). Fat free mass showed significant variations between groups in absolute terms. Cisgender men exhibited higher absolute values than transgender men, while cisgender women had lower values than both transgender men and women. However, when accounting for body size through normalized measures (fat- free mass index, percentage fat-free mass, and appendicular FFMI), no significant differences emerged between transgender and cisgender athletes of the same gender.
Bone mineral density
Bone mineral density (BMD) did not differ significantly between transgender and cisgender athletes at any measured site (whole-body, femoral neck, proximal femur, or lumbar spine).
Lung function
FEV1 differences:
- Cisgender men had higher values than transgender men
- Transgender women outperformed both cisgender women and transgender men
FVC patterns:
- Cisgender men showed greater values than transgender men
- Transgender women exceeded cisgender women and transgender men
Ratio findings:
- Transgender women had marginally lower FEV1/FVC ratios than cisgender women
Peak flow:
- Transgender women demonstrated higher values than cisgender women
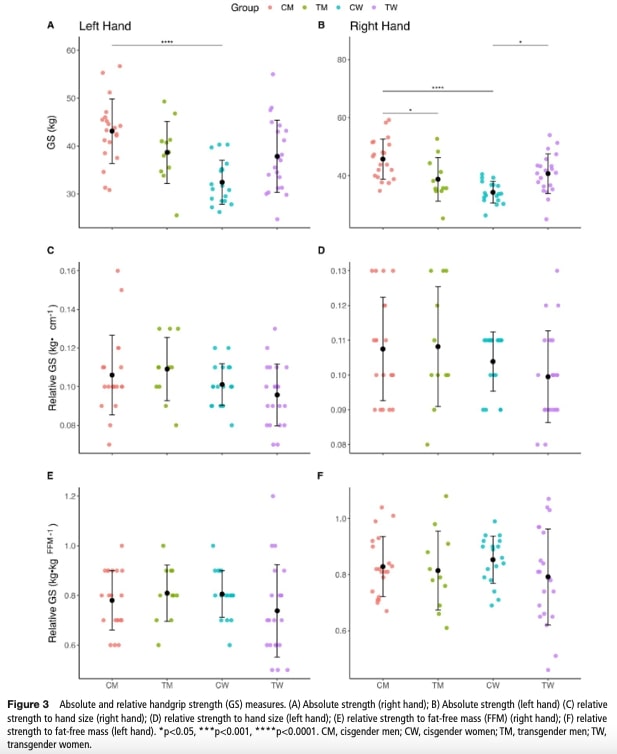
Grip strength
Absolute Right Handgrip:
The analysis of handgrip strength showed cisgender men exhibited significantly greater strength than transgender men, while transgender women demonstrated stronger grip strength compared to cisgender women.
Absolute Left Handgrip:
While significant intergroup variations emerged, analysis of transgender athlete performance metrics revealed no systematic disparities between transgender and cisgender athletes after controlling for physiological factors.
Normalized Strength (Fat-Free Mass & Hand Size)
After adjusting for confounding factors like fat-free mass and hand size, all previously observed significant differences in grip strength between groups disappeared completely. These findings demonstrate that variations in transgender athlete performance metrics for handgrip strength are primarily attributable to body composition and anthropometric factors (e.g., hand size) rather than gender identity alone.
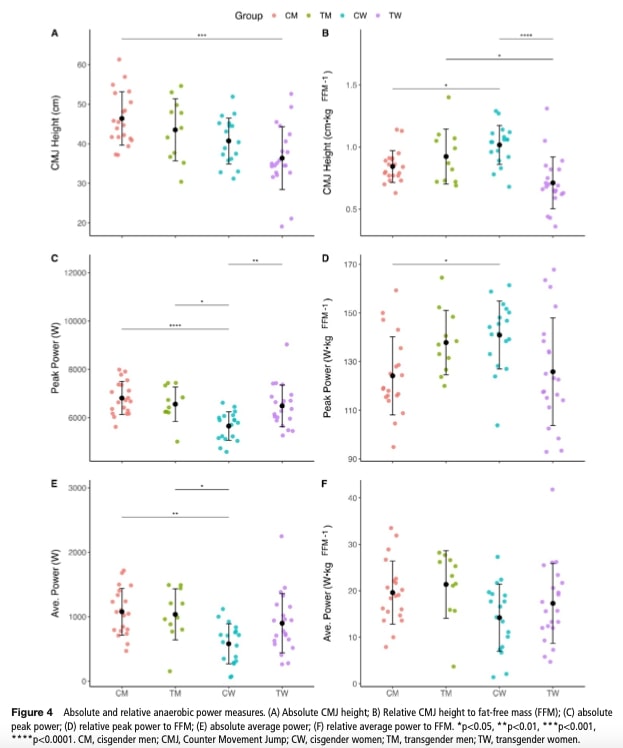
Lower Body Anaerobic Power
Absolute Countermovement Jump Height
The analysis showed cisgender men achieved significantly greater jump height than transgender women. Additionally, when normalized for fat-free mass, transgender women demonstrated lower jump height compared to both cisgender women and transgender men.
Absolute Peak Power
Cisgender women exhibited reduced peak power compared to both transgender men and transgender women. However, these differences disappeared when adjusted for fat- free mass.
Absolute Average Power
Cisgender women showed reduced average power compared to transgender men, though no differences remained after fat-free mass normalization.
Normalized Power (Fat-Free Mass Adjusted)
After accounting for fat-free mass, all significant differences in peak and average power between groups disappeared. The exception was jump height relative to mass, where transgender women underperformed both cisgender women and transgender men.
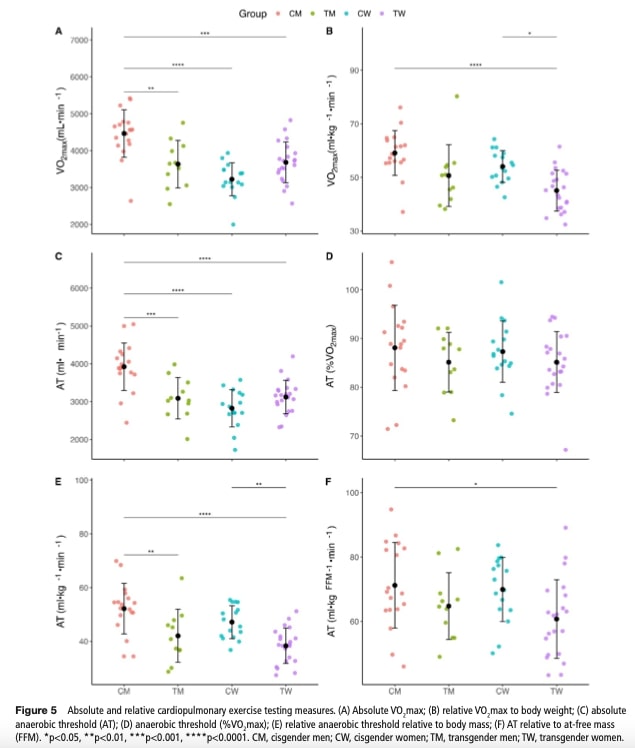
Cardiopulmonary exercise testing
Absolute VO2max
Cisgender men demonstrated significantly higher absolute VO2max than both transgender men and transgender women.
Body Mass-Relative VO2max
When adjusted for body mass, transgender women showed lower values than both cisgender men and cisgender women. Notably, when analyzing transgender athlete performance metrics for VO2max normalized to fat-free mass, no significant gender- based differences persisted
Anaerobic Threshold Findings
- Absolute thresholds were higher in cisgender men compared to both transgender groups.
- No differences existed when the anaerobic threshold was expressed as %VO2max.
- Body mass-relative thresholds were lower in transgender women versus both cisgender groups and in transgender men versus cisgender men.
- Fat-free mass adjustment reduced but didn’t eliminate differences, with a small but significant gap remaining between cisgender men and transgender women.
Finally, Table 2 provides a quantitative summary of the study results.
Câu hỏi và suy nghĩ
This comprehensive study reveals that while transgender athlete performance metrics exhibited some differences in absolute strength, power, and aerobic capacity compared to cisgender athletes, these disparities largely disappeared when adjusted for body composition and anthropometric variables. For example, differences in grip strength became non-significant after accounting for fat-free mass and hand size, and most variations in cardiopulmonary performance were similarly explained by normalization to fat-free mass. The notable exceptions were jump height relative to body mass, where transgender women underperformed compared to both cisgender women and transgender men, and a modest residual difference in anaerobic threshold (adjusted for fat-free mass) between cisgender men and transgender women. Additionally, the study highlights differences in body composition and fat mass distribution, which may be influenced by gender-affirming hormone therapy.
This study provides pioneering empirical evidence on transgender athlete performance metrics, offering crucial physiological insights for sports participation policies. These findings are particularly important in light of recent literature showing that individuals from sexual and gender minorities often experience discrimination in medical settings, potentially contributing to disparities in care and performance outcomes
While this study provides valuable insights, certain methodological limitations affect the generalizability of its findings. First, the sample size was relatively small (*n* = 75) and divided into four groups (cisgender men, cisgender women, transgender men, and transgender women), reducing the statistical power for between-group comparisons. Moreover, the recruitment method—via social media—may have introduced selection bias and recall bias, as participants self-reported their medical history and training levels. Crucially, the types of sports practiced and athletic experience may not have been sufficiently controlled—factors known to significantly influence performance metrics such as grip strength and VO2max.
Given that debates around the inclusion of transgender athletes in competitive sports often center on physiological differences, this study invites us to reflect on the multifactorial nature of athletic performance. While it underscores the role of body composition and fat mass distribution, it also raises the question of what other factors might be influencing performance outcomes. From a social science perspective, there is a growing body of research suggesting that discrimination, minority stress, and reduced access to training environments can negatively impact transgender athletes’ participation and development. For instance, a recent review on societal discrimination and mental health among transgender athletes found that exclusion and stigma can lead to decreased training frequency, lower self-esteem, and poorer mental health—factors that likely influence physical performance outcomes.
Taking this reflection further, one might argue that our current understanding of sports performance remains incomplete, particularly in terms of how social, psychological, and physiological factors interact. Mapping the full range of influences on performance could help explain—and perhaps predict—athletic outcomes more comprehensively. But this also raises a deeper ethical question: do we really want to fully “explain” and quantify performance in this way? Doing so may lead us to focus narrowly on measurable traits and could complicate efforts to fairly include or exclude athletes from competition. For instance, safety may also be an important aspect to consider; in sports like boxing, it is essential that opponents are on average equally matched in strength, ensuring no one exceeds the limits allowed within a given category. This highlights how both fairness and safety must inform our definitions of competitive equity. Rather than relying solely on gender classifications, this perspective suggests that key metrics directly associated with performance—such as strength, speed, or endurance—could potentially serve as more relevant and equitable classification criteria. Ultimately, recognizing the complex interplay of factors behind athletic performance might move the conversation beyond simple binary comparisons, toward more nuanced and inclusive policy decisions.
Nói chuyện với tôi một cách ngớ ngẩn
The researchers used different statistical methods depending on whether the data met certain assumptions, namely normality (the data follow a normal distribution) and homogeneity of variance (similar spread of data across groups). For data that satisfied these assumptions, they applied a one-way analysis of variance (ANOVA). This test is commonly used to determine whether there are any statistically significant differences between the means of three or more independent groups. In this case, it allowed the authors to compare measures such as strength and aerobic capacity across four distinct groups: cisgender men, cisgender women, transgender men, and transgender women.
When a significant difference was detected using ANOVA, the researchers conducted Bonferroni post hoc tests to perform pairwise comparisons between groups. The Bonferroni correction is a method used to control for Type I error (false positives) that can occur when making multiple comparisons. It does this by adjusting the p-value threshold based on the number of comparisons, making the test more conservative but more reliable in identifying true differences.
For data that did not meet the assumptions of normality or equal variances, the researchers used the Kruskal-Wallis ANOVA, a non-parametric alternative to the one-way ANOVA. This test compares the medians between groups rather than the means and does not require the data to follow a normal distribution. When significant differences were found using this method, they applied the Dwass-Steel-Critchlow-Fligner (DSCF) post hoc test. This test is specifically designed for multiple non-parametric comparisons and maintains appropriate control over Type I error across multiple group comparisons, similar to the Bonferroni method but adapted for non-normal data.
An alpha level of 0.05 was used throughout the analysis to determine statistical significance, meaning results with a p-value less than 0.05 were considered statistically significant. Finally, the study followed the Checklist for Statistical Assessment of Medical Papers, a standardized guideline that ensures the statistical analyses are conducted and reported rigorously and transparently. This adherence strengthens the credibility and reproducibility of the findings.
Take home-messages
- Differences in strength and aerobic capacity between transgender and cisgender athletes are largely explained by body composition (e.g., fat-free mass) and anthropometric measures rather than gender identity alone.
- Gender-affirming hormone therapy may significantly impact muscle mass, fat distribution, and physical performance markers. Physiotherapists should consider these factors when developing rehabilitation or training plans, particularly in athletic populations.
- While this study provides important physiological insights, its limitations— including small sample size, self-reported training levels, and lack of sport specificity—underscore the need for cautious interpretation and further research.
- Psychosocial factors such as discrimination, access to care, and mental health concerns may affect training consistency, recovery, and overall physical functioning in transgender individuals. These should be integrated into biopsychosocial assessments and patient-centered care.
- In clinical and athletic settings, physiotherapists have a role to play in promoting inclusive environments and advocating for equitable access to care and sport participation, recognizing that performance is influenced by both biological and social determinants.
As sexual minority populations often face discrimination in healthcare systems, patient- centered care becomes a crucial approach. These two Physiotutors blog articles on patient-centered care and shared decision-making provide ready-to-use information to enhance your clinical skills.
Thẩm quyền giải quyết
HAI HUYỀN THOẠI BỊ PHÁ VỠ & 3 QUẢ BOM KIẾN THỨC MIỄN PHÍ
Trường đại học nào không nói cho bạn biết về hội chứng chèn ép vai và loạn động xương bả vai cũng như cách cải thiện đáng kể tình trạng vai của bạn mà không phải trả một xu nào!