
Research
Exercise
May 5, 2025
Tham gia các hoạt động an toàn sau phẫu thuật thay khớp háng toàn phần (THR).

Giới thiệu
Being one of the most common orthopedic surgeries performed, activity participation after total hip replacement (THR) remains controversial. With some surgeons and health care practitioners fiercely discouraging people from participating in higher impact-related sports, others are supporting any activity participation without restrictions. In 2023, we published a blog article concerning returning to running after THR, concluding that most of the available evidence was merely based on expert opinions and fear, rather than on sound evidence. Swanson et al. (2009), for example, indicated that surgeons who performed many hip replacement surgeries were generally more likely to encourage participation in higher-load impact activities, suggesting that fear may be a factor holding other surgeons back from supporting their patients in returning to their desired level of sports. This limited evidence calls for more in-depth research, and the current study used a prospective cohort design to follow people post-surgery and to investigate what safe activity participation following THR could consist of.
Phương pháp
A prospective parallel cohort study was undertaken to answer the following research questions:
- Is there activity-related pain at any time point after THR surgery?
- If any activity-related pain is present, is it associated with activity intensity and duration? (primary aim)
- Is there a change in patient-reported outcomes or activities over time?
- What is the association of revision rates and activity intensity over time?
Two cohorts were compared: one recruited at the time of THR surgery (cohort 1) and the other at 5-7 years post-surgery (cohort 2). Both of these cohorts were followed for five years, with 2 assessments per year. Participants under the age of 80 years with end-stage hip arthritis (due to osteoarthritis, avascular necrosis, or hip dysplasia), scheduled for their primary unilateral THR, were included.
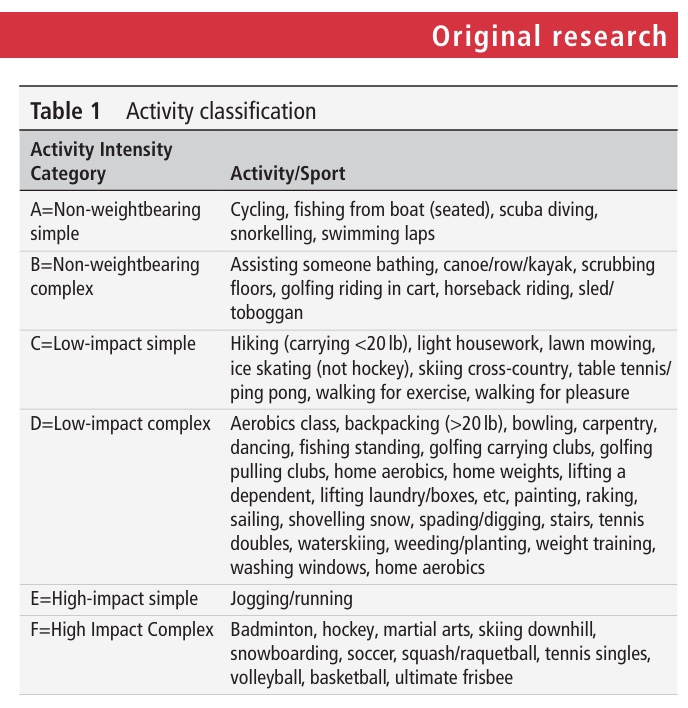
Physical activities were assessed at baseline and each year, using the Minnesota Leisure Time Physical Activity Questionnaire (MLTPAQ). This is a tool that captures the self-reported frequency and intensity of a wide range of physical activities. From this questionnaire, 6 groups of activities were created, based on their level of impact and torque on the prosthetic joint.
The WOMAC index, Pain Catastrophizing Scale (PCS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP) scale were administered. The WOMAC measures health status, with lower scores indicating lower levels of physical disabilities. The PCS measures thoughts and feelings associated with chronic pain, with higher scores representing greater catastrophizing. The ICOAP evaluates patients’ experiences with pain in their hip, distinguishing between intermittent and constant pain. Lower scores indicate lower levels of disability.
Kết quả
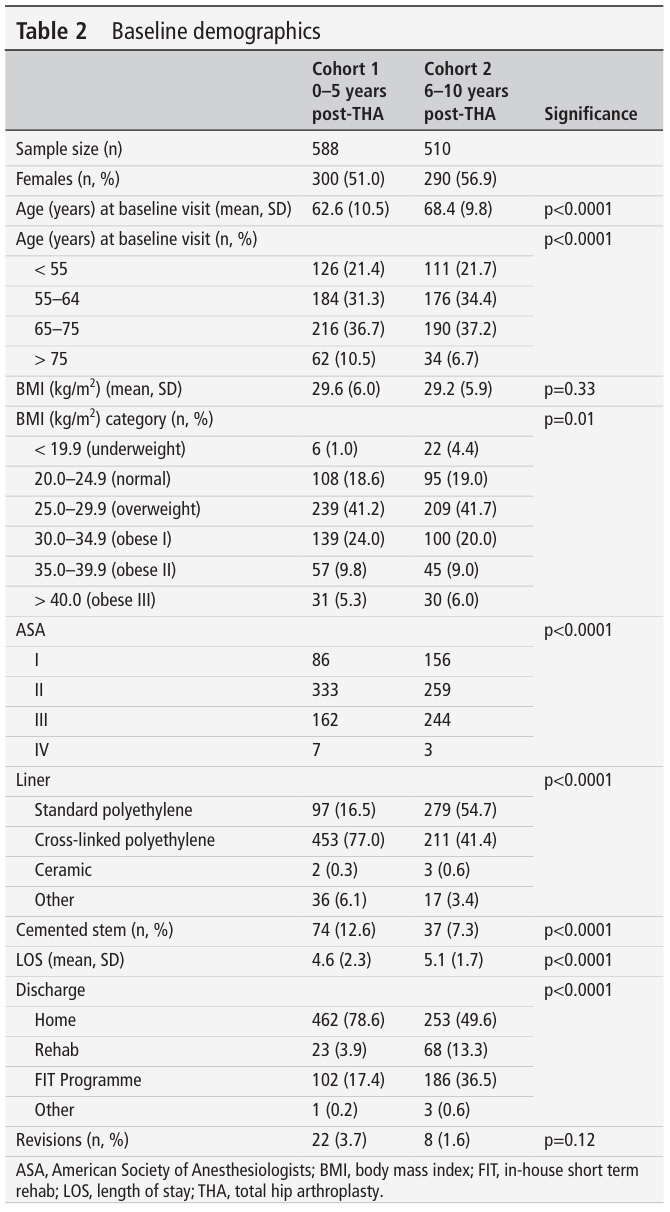
1098 subjects were included in the cohort study, 588 in the first cohort and 510 in the second. The samples were approximately equally divided into males and females. Age at baseline was around 62 years in the first cohort and 68 in the second, which was significantly different. But importantly, age at surgery was not different between the cohorts. Remember, the second cohort was already at 5-7 years post-THR surgery.
Other baseline differences between the cohorts were in the BMI categories (with more underweight participants in cohort 2), the American Society of Anesthesiologists (ASA) physical status classification system, which is a surrogate for comorbidities, the liner material, the number of cemented stems, length of hospital stay and location of discharge.
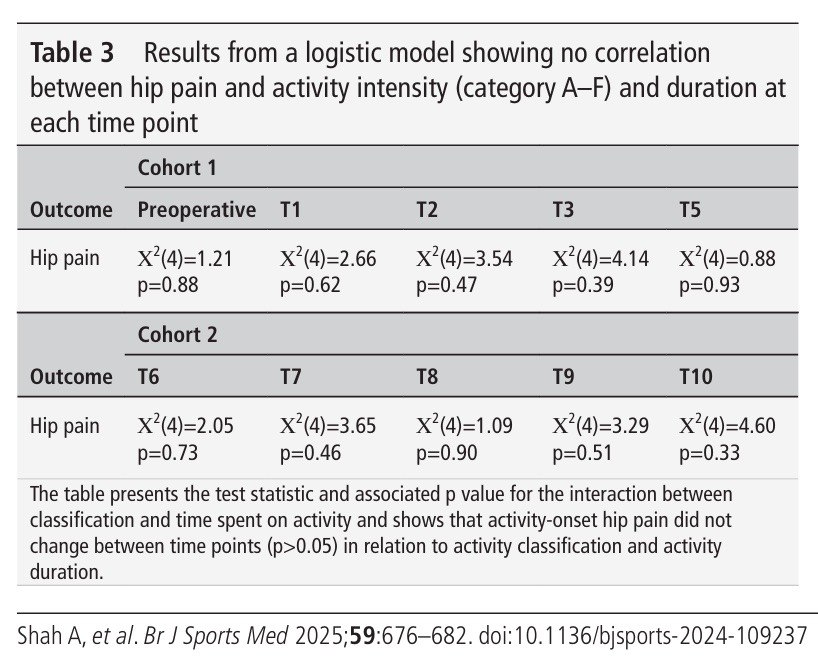
One in five reported hip pain with activity, and one in eight indicated having reduced their participation in activities due to hip pain. However, the regression did not reveal an association between hip pain and activity intensity.
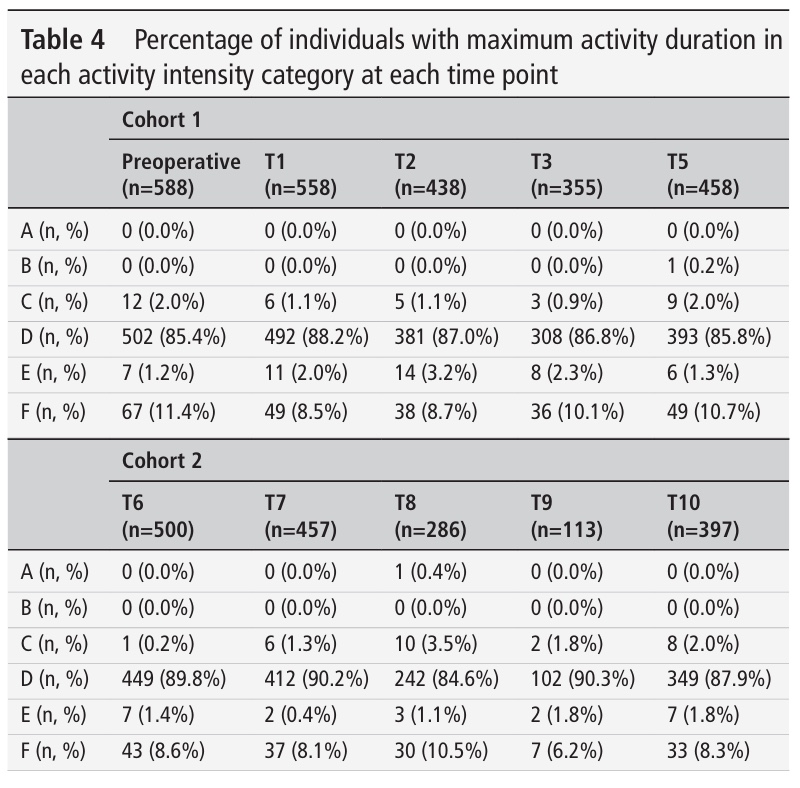
Further, the cohorts did not change the mean duration of activities spent in each of the categories A-F when comparing baseline and all postoperative visits.
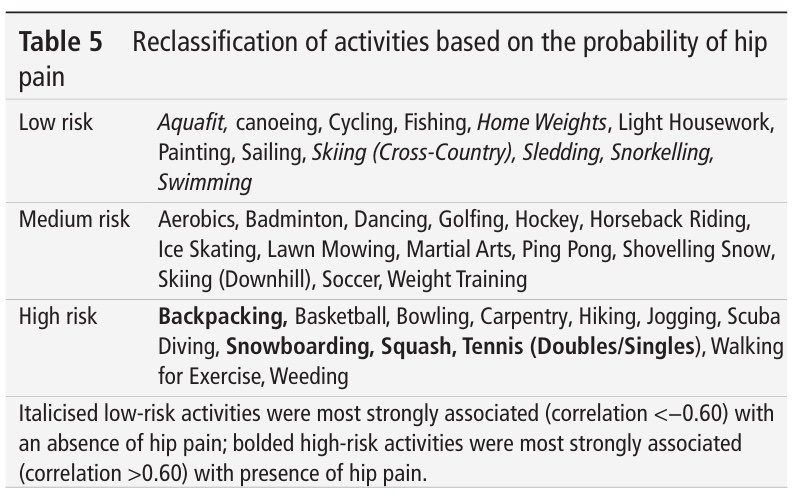
The MLTPAQ classification of activities showed a correlation to hip pain and activity. Therefore, a logistic regression was conducted to look into the association. This analysis led to a reclassification of activities into low-, medium-, and high-risk categories for the probability of hip pain.
In this cohort, including almost 1100 people, only 30 revisions occurred. Twenty-two were noted in the first cohort, and 8 in the second. Again, no significant relationship emerged between the activity levels and the number of revisions.
All patient-reported outcomes improved from baseline (preoperative), to the first postoperative visit, as expected. These measures remained constant over the other postoperative timepoints.
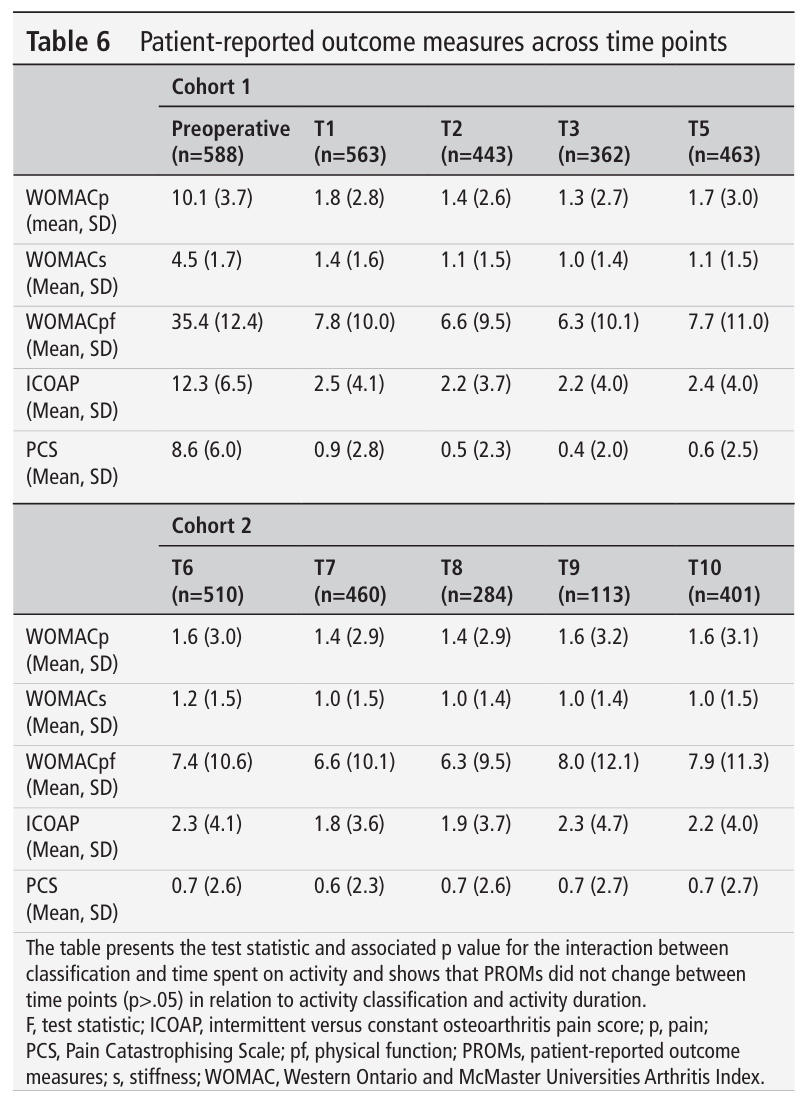
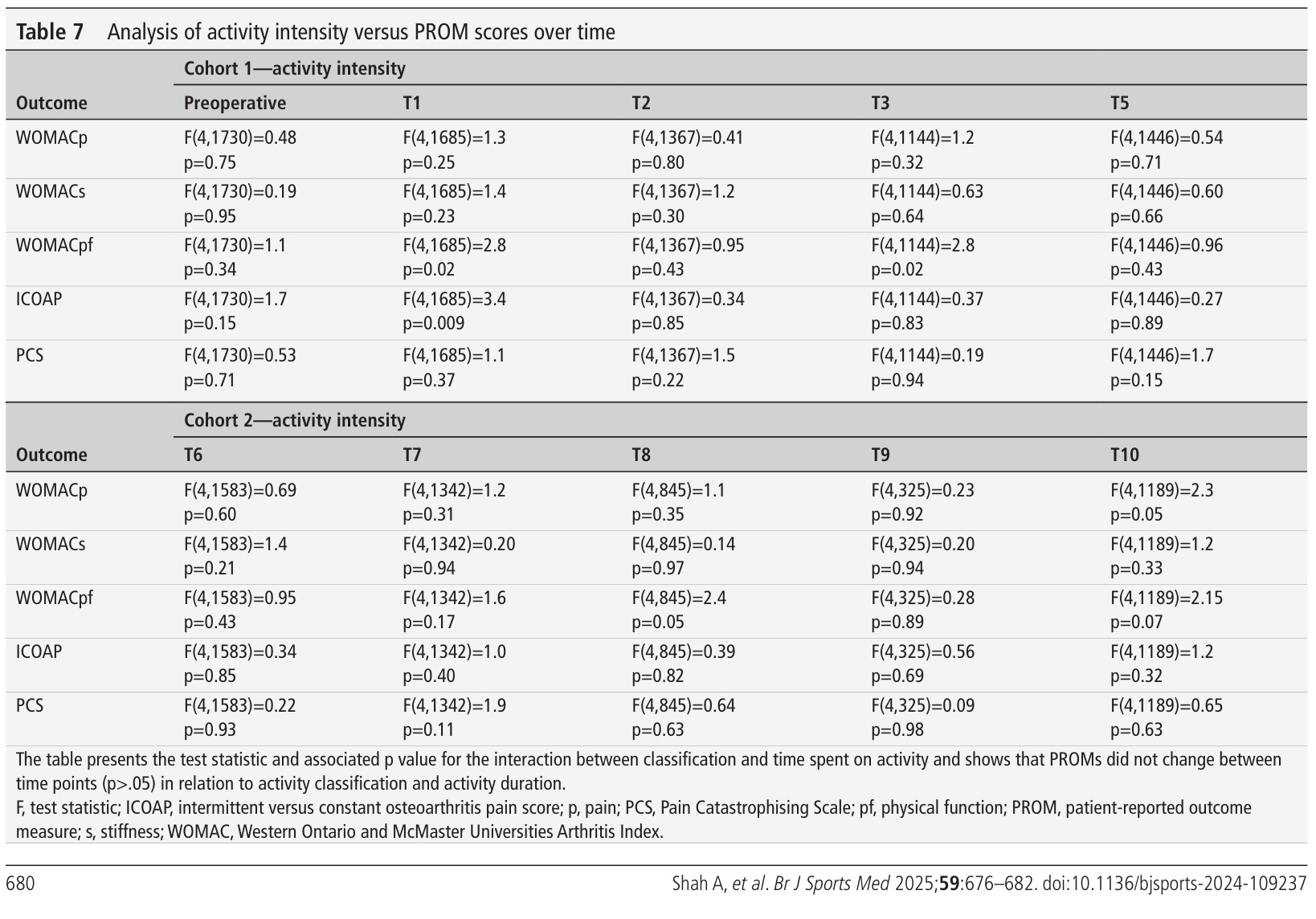
A subanalysis was run to seek whether the intensity of activities led to changes in patient-reported outcomes, but was negative. The patient-reported outcomes did not worsen over time in people participating in higher-intensity sports. But, those participating in higher-intensity activities had a greater change in ICOAP score at T1, but not anymore afterwards. The reclassified activity categories did not show any change in patient-reported outcomes over time.
Câu hỏi và suy nghĩ
Previous research indicated that the best prognostic indicator for returning to sports was the previous experience in that sport. The main reason patients did not return to sports was the surgeon’s recommendation. Sowers et al. (2023). The current study tackles the recommendation to avoid high-intensity activities after undergoing THR and can guide safe activity participation following THR.
A limitation of this study lies in the use of self-reported data, which may be prone to recall and reporting biases. Also, the average physical activity was self-reported at baseline and over 1 year, and then every six months. This approach does not consider that activity participation may vary through the year, for example, due to seasonal changes. Nor does it account for peaks and lows in activity participation; rather, these extremes are flattened out. Certain details may not get captured over such long periods of reporting. A monthly report could have been more suited.
There was an age difference at baseline. However, the second cohort was already at 5-7 years post-surgery at enrollment. There was no age difference between the cohorts when considering the age at the time of the THR surgery. Yet, a 5-7 year difference between the cohorts can have led to differences in surgical techniques and materials used, which may be confounding certain effects.
Those participating in higher-intensity activities had a greater change in ICOAP score at T1, but not anymore afterwards. This effect can likely be attributed to the sudden increase in postoperative demands after the operation to T1. You can consider that this approach may be a bit fast for high-intensity activities. Although not contraindicated, as these results have shown, you should consider progressions in every individual. For some, participation in high-intensity sports may be too early at 1 year postoperative, while others may progress faster.
Revision rates in this study were low: 30 occurred in a sample of almost 1100 people. That’s only about 3%. The low occurrence of revisions is a good indication of the safety of participation in higher-intensity activities, yet it can be a limitation since a sufficient number of outcomes would be necessary to make meaningful conclusions about the risk of revisions.
Nói chuyện với tôi một cách ngớ ngẩn
Two different cohorts were followed, as described above, one immediately following the THR surgery, with the other cohort already having been operated on 5 to 7 years earlier. This was to ensure a sufficient follow-up period, without increasing the costs associated with a very long follow-up. The first cohort was followed from surgery until 5 years postoperative, the second cohort delivered data from 10 to 12 years postoperative. This way, both the immediate period after surgery and more longitudinal data from several years later could be analysed without having to set up a very costly study. But also because the authors expected that many revisions in the first years after surgery would be due to infections and trauma, but not due to “wear” from intense activities, this risk was mitigated.
Activity levels were first classified into 6 groups, A to F, based on the evidence from biomechanical studies looking at contact forces and torsion on the hip joint. But a biomechanical load does not imply pain. Therefore, this study reorganized the activity levels using data from a logistic regression analysis looking at how these activities actually related to patients’ experience of hip pain. This allowed them to “reclassify” the 55 activities from the MLTPAQ into three risk groups:
- Low Risk: These activities were less likely to be associated with hip pain
- Medium Risk: These activities had a moderate association with hip pain.
- High Risk: These activities were more likely to be associated with hip pain.
Even though they reclassified activities into these 3 categories based on the probability of associated hip pain, these classifications did not translate into a difference in revision rates. Researchers looked at whether people who engaged in “High Risk” activities (like snowboarding, squash, or tennis singles) were more likely to need a revision (a second surgery) of their hip replacement. Despite these activities being associated with higher reports of pain, there was no evidence that they led to a higher rate of revisions. This is a very important point, as it informs the advice that surgeons and physicians can give to patients about activity after hip replacement surgery.
The authors looked further than just activity level, by also running their analyses for activity duration and the interaction of the type of activity with the duration. Although not specifically mentioned as being sensitivity analyses, these additional analyses can be viewed in this way since they helped explore different perspectives of the collected data. Equally, these models did not show differences regarding activity and hip pain over time.
Những thông điệp mang về nhà
The study concluded that there was no association between the intensity of physical activities and hip pain. Furthermore, higher-intensity activity participation did not lead to worsening patient-reported outcomes over time, nor did it increase revision rates. Over the follow-up, the participants were not forced to reduce their activity intensity. This altogether implies that activity restrictions should not be applied to individuals following THR. The authors point to a shared-decision making between the patient and his healthcare providers, to allow for safe activity participation following THR.
Thẩm quyền giải quyết
NÂNG CAO CHẨN ĐOÁN PHÂN BIỆT CỦA BẠN VỀ ĐAU HÔNG LIÊN QUAN ĐẾN CHẠY BỘ - MIỄN PHÍ!
Đừng để có nguy cơ bỏ lỡ những dấu hiệu cảnh báo tiềm ẩn hoặc phải điều trị cho người chạy bộ dựa trên chẩn đoán sai ! Hội thảo trực tuyến này sẽ giúp bạn tránh mắc phải những sai lầm mà nhiều nhà trị liệu thường mắc phải!
