
Research
Lumbar/SIJ
June 5, 2025
Quan điểm của bệnh nhân về việc tập thể dục thay vì phẫu thuật: Kỳ vọng về điều trị đau lưng dưới dự đoán như thế nào về hiệu quả giảm đau lâu dài và cải thiện chức năng?

Giới thiệu
Low back pain (LBP)—a leading global cause of disability—drives high healthcare use, yet outcomes remain poor due to its complex, biopsychosocial nature. Crucially, patient treatment expectations for LBP shape engagement and recovery, with optimistic beliefs often enhancing outcomes. However, mismatched expectations—such as overestimating surgery’s benefits—may worsen long-term function.
This study investigates how baseline treatment expectations for LBP (exercise or surgery) predict pain and function in LBP patients receiving nonpharmacologic care. By revealing which expectations align with better outcomes, the findings can refine clinician-patient communication, helping steer patients toward evidence-based, expectation-sensitive care—a key step in improving LBP management.
Phương pháp
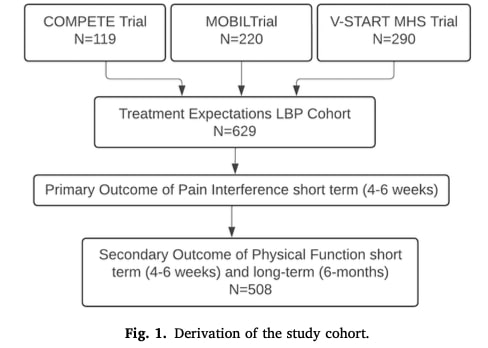
This prospective cohort study included 629 participants derived from three different randomized control trials. This pooled analysis included participants from three null-result (no significant treatment effects) trials of non-pharmacological LBP treatments conducted across US Military Health System hospitals. All patients were screened for red flags and received either: (1) early classification-based physical therapy, (2) educational video with self-management guidance, or (3) risk-stratified care using the STarT Back tool. Control groups received usual primary care. Common elements included exercise education/advice to stay active, with some participants receiving structured exercise interventions. Notably, no trial involved surgical randomization or subsequent surgeries during follow-up.
At baseline, patients rated their agreement (1-5 scale) on whether specific treatments would improve their back pain. The analysis focused on surgery and exercise (aerobic/resistance) expectations as key contrasting treatments in pain management. Responses were categorized as: high expectations (scores 4-5), neutral (score 3), and low expectations (scores 1-2) for:
- Surgery (“high surgical expectations”)
- Both aerobic and resistance exercise (“high exercise expectations”)
This dichotomization allowed comparison between patients with strong beliefs in each treatment’s efficacy prior to receiving non-surgical care.
Primary Outcome:The study used the NIH-developed PROMIS (Patient-Reported Outcomes Measurement Information System) to measure pain interference. PROMIS Pain Interference domain (PI) is a validated test that quantifies how much pain hinders daily activities (e.g., work, social engagement) over the past week. Scores are derived from patient responses to dynamic, severity-weighted questions (e.g., “How much did pain interfere with household chores?”). The primary endpoint was PROMIS PI at 4-6 weeks, with data pooled across trials (one trial’s Oswestry scores were converted to PROMIS PI using crosswalk tables).
Secondary Outcomes:PROMIS Physical Function (PF) was also assessed, measuring mobility and task performance (e.g., “Are you able to climb stairs?”). Both measures use T-scores (mean=50, SD=10 in the general population), where:
- PI: Higher scores = worse pain-related disability
- PF: Higher scores = better function.
Statistical approach
Separate regression models (n=6 total) assessed exercise and surgery expectations as independent predictors of short-term (4-6 weeks) and long-term (6 month) outcomes, avoiding collinearity concerns since expectations weren’t mutually exclusive. Generalized linear models adjusted for baseline scores, age, active-duty status, and military rank. A conservative significance threshold (p<0.025) accounted for multiple comparisons. Rigorous model validation confirmed assumptions of linearity, independence, and homoscedasticity using residual diagnostics. Missing data were handled via Bayesian multiple imputation (20 iterations). Sensitivity analyses on complete cases (n=595 primary; n=481 secondary outcomes) verified result robustness.
Kết quả
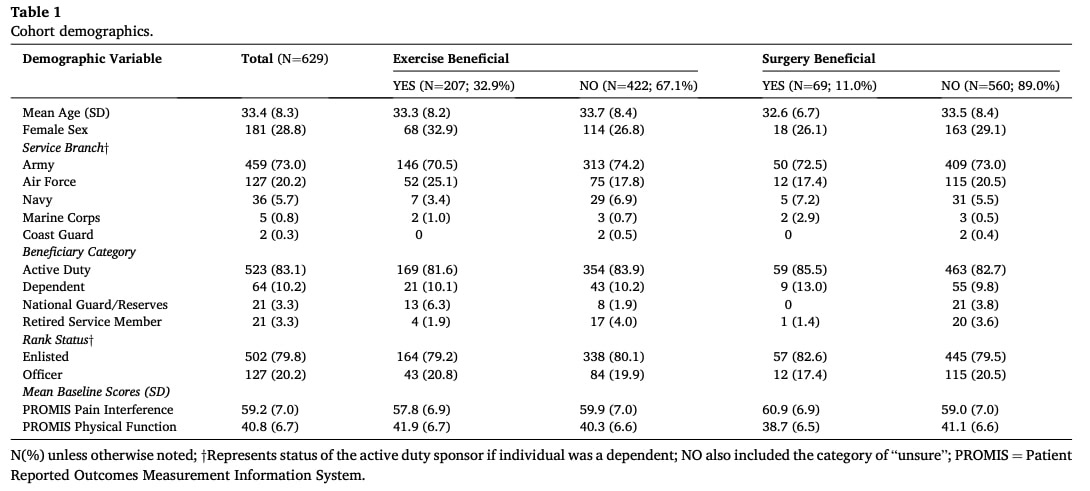
The analysis included 629 participants (mean age 33.4±8.3 years; 28.8% female; 83.1% active-duty). Demographic characteristics were relatively balanced across expectation groups.
Pattern of treatment expectations for LBP revealed:
- 32.9% had high exercise expectations (believed both aerobic and resistance training would help).
- 28.9% had high expectation for exercise only.
- 11% had high surgery expectations.
- 7% had high expectation for surgery only.
- Only 4% had high expectations for both treatments.
- 60.1% had low expectations for both exercise and surgery.
Notably, the high surgery expectation group showed worse baseline status: highest pain interference and lowest physical function scores.
Expectations on pain interference and physical function
Surgery Expectations:
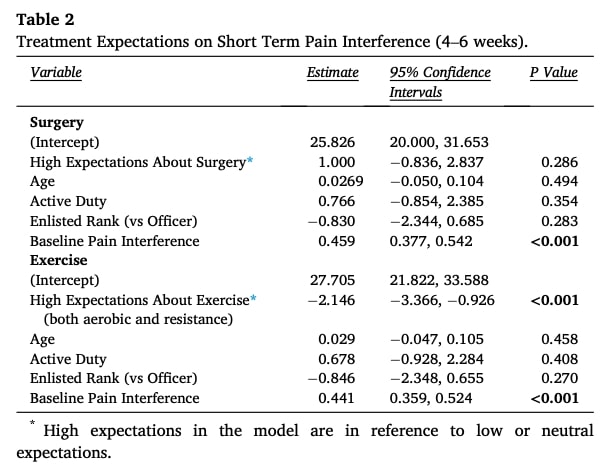
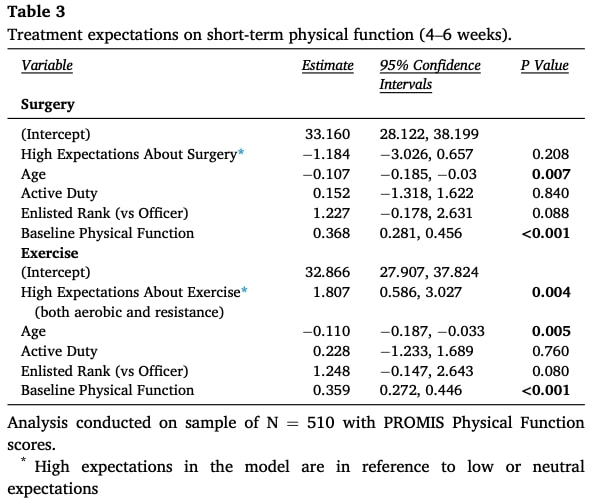
High expectations were not a significant predictor of pain interference or physical function at 6-week or 6-month follow-ups (Tables 2 and 3).
Exercise Expectations:
At 6 Weeks: High exercise expectations predicted lower pain interference and higher physical function.
At 6 Months: High expectations remained significant for reduced pain interference and improved function.
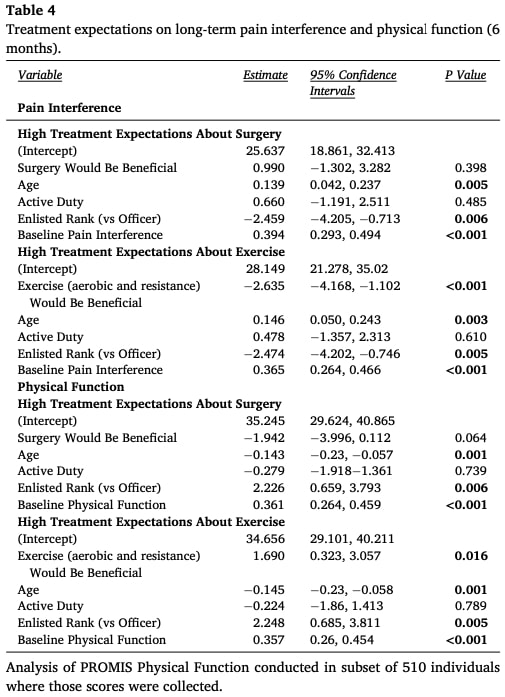
Influence of covariates
Age demonstrated progressive effects over time, showing no association with short-term pain interference but emerging as a significant predictor of poorer physical function at both 6 weeks and 6 months, along with increased 6-month pain interference.
military rank selectively influenced long-term outcomes, with enlisted personnel exhibiting clinically meaningful improvements at 6 months—reporting both reduced pain interference and enhanced physical function compared to officers. These demographic patterns complemented the primary expectation-driven findings while highlighting distinct temporal trajectories for different covariates.
Câu hỏi và suy nghĩ
Although this study was conducted in a specific military population—with distinct social and demographic characteristics that limit generalizability—it nonetheless highlights a critical disconnect in patient beliefs. Only 32.9% of participants had high expectations for exercise, and among them, a majority (55.1%) simultaneously expressed doubts about the effectiveness of surgery. This lack of confidence in both conservative and invasive treatments was strongly tied to poorer outcomes, suggesting that pre-treatment pessimism may create a self-fulfilling prophecy. Clinically, this underscores the need to proactively address exercise-related misconceptions early in care. For example, using motivational interviewing techniques to explore fears (“What concerns you about trying exercise?”) or sharing success stories from similar patients could help reframe expectations.
Notably, patients with higher baseline pain and disability were more likely to expect surgery to help—even though pain severity rarely correlates with structural damage in back pain. This reflects a common patient misperception that intense pain is due to severe tissue damage requiring aggressive intervention. Here, pain neuroscience education could play a transformative role by explaining how pain works (e.g., central sensitization) and why movement is often safe and beneficial. Future research should test whether such education reduces surgery expectations in high-pain subgroups.
The dynamic nature of treatment expectations for LBP—shaped by clinician interactions and time—offers both a challenge and an opportunity. The study’s strict definition of “high exercise expectations” (requiring belief in both aerobic and resistance training) may underestimate optimism for specific interventions. This suggests that tailored expectation assessments (e.g., asking about yoga vs. strength training) could better predict adherence and outcomes. Limitations like the lack of post-treatment expectation data highlight the need for longitudinal tracking of how beliefs evolve during care.
Ultimately, these findings position clinicians as “expectation architects.” By normalizing doubts (“Many patients share your concerns”), reframing surgery (“It’s one tool, but your nervous system often heals with activity”) and leveraging placebo-like effects (“This approach has helped others with similar pain”), providers can align patient beliefs with evidence-based recovery. The next frontier is embedding expectation-modification strategies into trials and practice—from 5-minute pre-exercise “benefit framing” to multi-timepoint expectation monitoring.
Nói chuyện với tôi một cách ngớ ngẩn
The study revealed how treatment expectations for LBP—particularly preferences for exercise versus surgery—directly shaped long-term pain and functional outcomes. Because participants could have high expectations for both treatments simultaneously, the researchers avoided statistical confounding by modeling exercise and surgery expectations separately. This approach was critical because patients could hold strong beliefs about both treatments simultaneously, which – if analyzed together – might obscure whether improvements were truly driven by exercise expectations, surgery expectations, or their interaction. To fully isolate these effects while accounting for different outcome timelines, they ran six distinct linear regression models—statistical tests measuring how expectations predict outcomes—separately assessing each expectation type (exercise/surgery) against short-term (4-6 weeks) and long-term (6 months) measures of both pain interference and physical function. This comprehensive approach not only prevented the statistical entanglement of overlapping expectations but also revealed whether their influence varied depending on the outcome type or follow-up period.
Each model adjusted for baseline scores, age, active-duty status, and military rank to isolate the specific impact of expectations. To ensure robust results, they validated key statistical assumptions (like linear relationships and consistent error patterns) using diagnostic plots and tests, while applying a stricter significance threshold (p<0.025) to account for multiple comparisons.
Missing outcome data were assumed to occur randomly (e.g., due to administrative gaps rather than treatment failure) and were addressed using Bayesian multiple imputation with Markov chain Monte Carlo (MCMC) simulations (20 iterations). This method replaced missing values with statistically plausible estimates based on patterns in observed data, using iterative sampling to refine accuracy while accounting for uncertainty. The researchers reran all analyses using only complete cases—participants with no missing data (N=595 for primary outcomes; N=481 for secondary outcomes)—to verify that the imputation process didn’t artificially distort results. If findings from the imputed datasets (with statistical guesses for missing values) matched the complete-case analysis, it confirmed that:
- The imputation model was reliable.
- Conclusions weren’t driven by assumptions about missing data.
Những thông điệp mang về nhà
This review confirms that patient treatment expectations for LBP significantly influence outcomes—both pain levels and functional recovery. Proactively assessing and addressing these beliefs should become routine in clinical practice.
How to Assess Beliefs
Ask directly: Use simple questions like:“What do you expect exercise to do for your back?”“Have past treatments met your expectations?”
To support your assessment and management of low back pain rehabilitation and patient expectations, explore these Physiotutors resources for clinical practice:
Standardized tools: Supplement with validated scales:
- STarT Back (risk stratification)
- Tampa Scale for Kinesiophobia (fear of movement)
- Pain Catastrophizing Scale (negative thought patterns)
Strategies to Modify Unhelpful Beliefs
- Gradual exposure: Systematically reintroduce feared movements (e.g., bending, lifting) to disprove harm expectations.
- Activity pacing: Collaborate on incremental return-to-activity plans to rebuild confidence.
- Team-based care: Refer to psychologists or pain specialists for entrenched fear/catastrophizing.
Thẩm quyền giải quyết
Dinh dưỡng có thể là yếu tố quan trọng đối với sự nhạy cảm trung tâm - Bài giảng video
Xem bài giảng video MIỄN PHÍ này về Dinh dưỡng và Nhạy cảm trung ương của nhà nghiên cứu về chứng đau mãn tính số 1 Châu Âu Jo Nijs. Những thực phẩm mà bệnh nhân nên tránh có thể sẽ khiến bạn ngạc nhiên!
