
Research
Lumbar/SIJ
October 6, 2025
Liệu pháp nắn chỉnh cột sống có hiệu quả trong việc điều trị thoát vị đĩa đệm không? Một nghiên cứu mới tiết lộ điều gì?

Giới thiệu
Lumbar disc herniation (LDH), most common at L4-L5 and L5-S1, is a major cause of low back and radicular pain due to nerve root compression. Treatment strategies are either surgical or conservative, with the latter including medications, injections, rest, exercise, and manual therapies. Among these, spinal mobilization involves gentle, passive joint movements that can reduce stiffness, improve mechanics, and trigger short-lived neurophysiological effects such as pain relief. Prior studies have shown benefits, mostly from neurophysiological mechanisms, of mobilization for pain and function in LDH and low back pain patients, and that herniation regression is possible with conservative treatment.
Most of the current literature, as discussed in this article review, suggests that the effectiveness of manual therapy is largely explained by short-term neurophysiological mechanisms rather than structural or mechanical changes. This study uniquely investigates mobilization for herniation regression by assessing if multi-directional techniques, when combined with stabilization exercises, can induce measurable structural changes. Specifically, it investigates their impact on radiological parameters such as herniation size, disc height, and facet joint distance, alongside clinical outcomes including pain, function, mobility, and flexibility.
Phương pháp
Study Design
This research was a single-blinded, randomized controlled clinical trial conducted at the outpatient physiotherapy clinic. Participants were randomized into two groups:
- Intervention group: spinal mobilization for disc herniation regression + stabilization exercises
- Control group: stabilization exercises only
No additional physiotherapy or pain medication was allowed during the treatment period.
Inclusion criteria
- Confirmed lumbar disc herniation (LDH) by MRI and physician diagnosis
- Pain score ≥ 3 on the Visual Analogue Scale
- Persistent pain for at least 8 weeks
- Age between 18 and 65 years
Exclusion criteria
- Previous spinal surgery
- Autoimmune diseases
- Spondylolisthesis
- Spinal fractures
- Cardiac pathologies
- Stroke history
- Cauda equina syndrome
- Current use of pain medication
- Spinal inflammation
- Spinal tumors
- COVID-19
- Pregnancy
Sample Size and Randomization
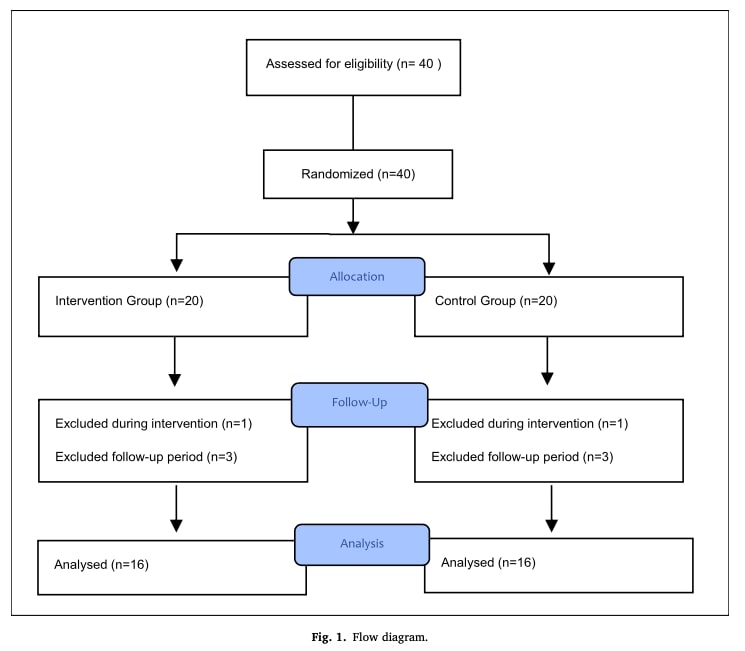
Sample size was calculated based on pilot data, with 16 participants per group required to achieve 80% power at a 5% error level. A snowball sampling method was used, followed by random allocation to intervention or control groups. A total of 40 individuals initially met eligibility requirements. Due to withdrawals (pregnancy, relocation, or unspecified reasons), 32 participants (26 men, 6 women) completed the study.
Randomization and Blinding
Participants were randomly allocated to intervention or control groups (1:1) using sealed envelopes. Both participants and the radiologist/statistician were blinded to group assignments, while the same physiotherapist conducted all mobilization and clinical assessments.
Measurement Timeline
Assessments were carried out at three time points: before treatment (T1), after treatment (T2), and at a three-month follow-up (T3).
Baseline and Primary Outcomes
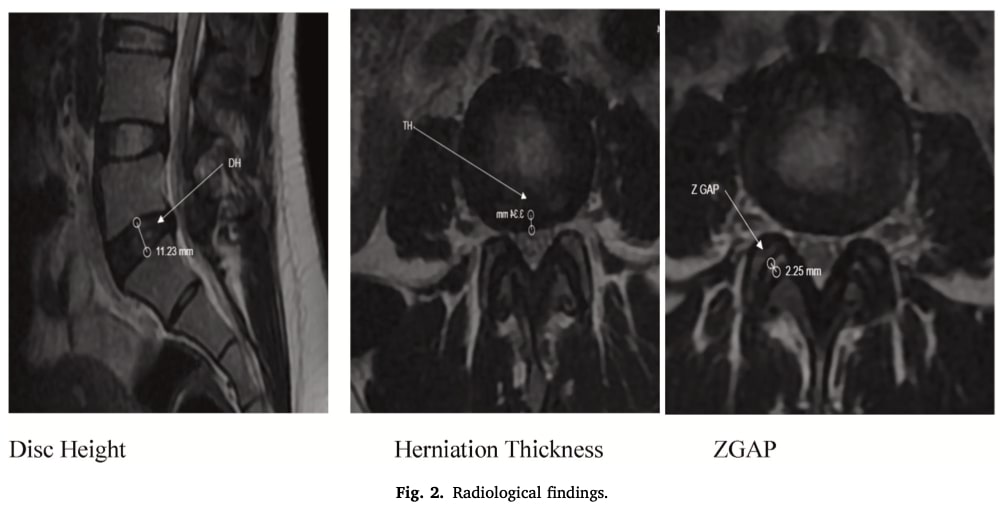
Demographic data included diagnosis, age, gender, height, weight, and BMI. MRI scans, performed before and after treatment by a blinded radiologist, measured disc height, herniation thickness, and facet joint distance. In cases of multiple herniations, the most severe level was analyzed.
Pain Assessment
The study quantified participants’ pain levels using the Visual Analogue Scale (VAS), a validated and reliable tool. The VAS is a line anchored by the descriptors “no pain” on one end and “severe pain” on the other. Patients self-reported their current pain level by marking a point along this line. The resulting measurement, taken from the “no pain” endpoint to the patient’s mark, provided a numerical value for pain intensity.
Range of Motion Assessment
Hip joint range of motion was objectively measured using a validated Straight Leg Raising Test (SLRT) in conjunction with a digital inclinometer. For this test, the participant lay supine with the inclinometer placed on the tibia. With the knee kept in full extension, the hip was flexed. The test was considered positive, and the angle was recorded at the point where the participant experienced pain in the lower extremity. To ensure accuracy and capture the maximum range, the test was performed three times, with the highest value being used for analysis.
Flexibility Assessment
Lumbar flexibility was evaluated using the validated Sit and Reach Test. Participants sat with legs straight and feet flat against a test board. They then leaned forward from the waist, pushing a measuring board with their fingertips while maintaining straight knees, and held the final position for 1-2 seconds. The distance reached was measured in centimetres. This procedure was repeated three times, and the average of these distances was calculated and recorded for data analysis.
Intervention Protocol
The study featured a two-group design to compare treatment efficacy. The control group received a program of stabilization exercises only. In contrast, the intervention group underwent the same stabilization exercises but with the addition of spinal mobilization techniques applied beforehand. The entire treatment regimen was conducted over ten sessions, scheduled twice weekly for five weeks. The intervention began with education on safe spinal movements and awareness of the neutral spine position, highlighting the role of deep stabilizer muscles in maintaining this alignment. Under physiotherapist supervision, participants practiced activating these muscles while preserving spinal neutrality. Training then progressed in stages: first ensuring correct activation and control, then building endurance through increased repetitions, and finally enhancing strength by adding resistance or modifying the lever arm. Throughout, feedback was provided to ensure safe and accurate execution.
Stabilization Exercises:
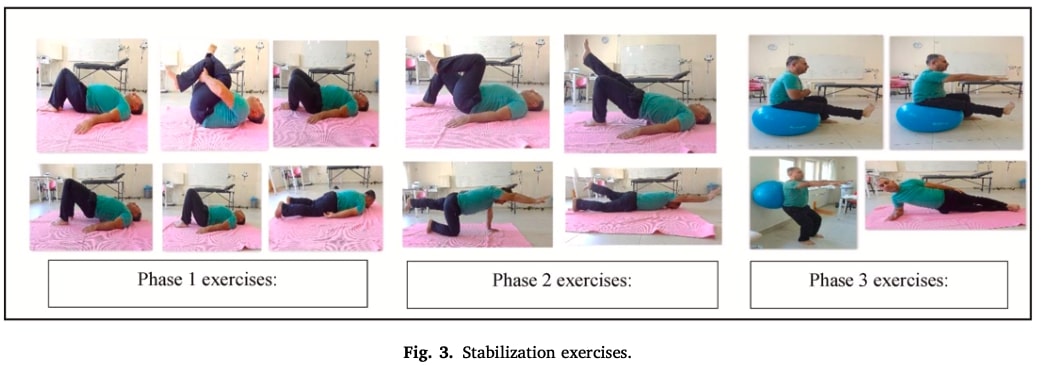
This was a progressive, three-phase program supervised by a physiotherapist.
Phase 1 focused on activating local deep-core muscles (transversus abdominis and multifidus) with exercises like maintaining neutral positions in supine and prone, piriformis stretching, and basic bridge-building.
Phase 2 increased complexity with exercises such as single-leg bridges and cross-arm-leg lifts in prone and crawling positions.
Phase 3 introduced dynamic movements, including mini-squats, leg extensions on a stability ball, and lateral bridges.
Participants were provided with brochures and, after the formal treatment period, were advised to continue the exercises at home until the three-month follow-up, with weekly telephone monitoring by the research team.
Spinal Mobilization Practices:
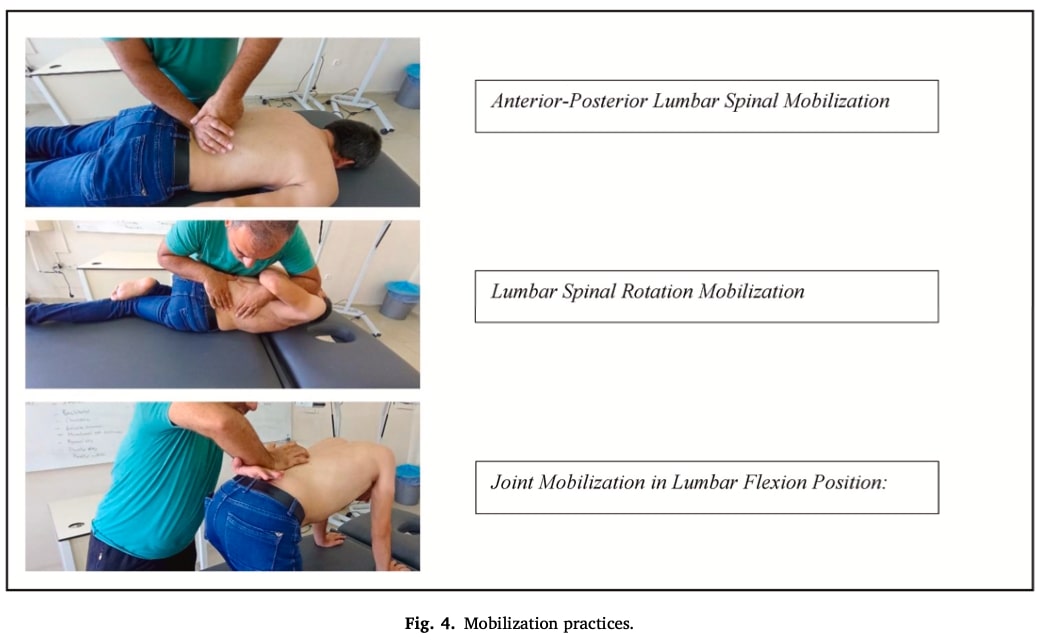
The mobilization for disc herniation regression component consisted of three specific techniques, described as being performed in the manner of Maitland IV grade. The techniques included:
- Anterior-Posterior Mobilization: Applying downward pressure on the lumbar spinal processes with the patient in a prone position.
- Lumbar Rotation Mobilization: Applying a rotational force to the lumbar spine with the patient lying on their side.
- Joint Mobilization in Flexion: Mobilizing individual vertebrae while the patient was supine in a lumbar-flexed position.
Each of these mobilization techniques was repeated 20 times per lumbar vertebra during the treatment sessions.
Statistical analyses
The team verified that all their data followed a normal, bell-curve distribution, which is a key requirement for the statistical tests they used. They did this by checking metrics called skewness and kurtosis, confirming all values fell within an acceptable range.
To compare the two groups at a single point in time—for instance, looking at patient demographics or one-off radiological results—they used independent-sample t-tests. This test determines if the average score of one group is significantly different from the other.
The analysis of changes over time was handled in two ways. For tracking changes within a single group across two time points, such as before and immediately after treatment, a paired-sample t-test was used to see if participants improved from their own baseline. For measurements taken at three or more time points, a more powerful test called repeated-measures analysis of variance (ANOVA) was applied. Whenever this test found a significant change, a follow-up test (the Least Significant Difference test) was used to pinpoint exactly which time points were different from each other.
Most importantly, to answer the key question of whether the new treatment led to a better rate of improvement than the control, the researchers used two-way and three-way ANOVA tests. This method directly compares how the pattern of change over time differs between the intervention and control groups.
Throughout the entire study, a result was considered statistically significant if the probability of it occurring by chance was less than 5%, adhering to the conventional threshold of p < 0.05.
Kết quả
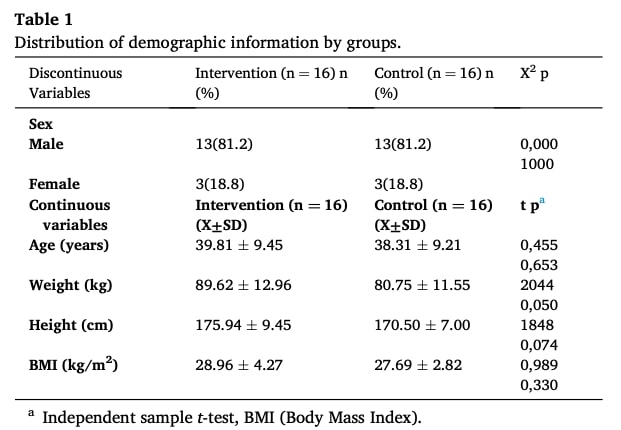
The demographic profiles of participants, including age, weight, height, and BMI, were comparable between the intervention and control groups. Both groups had a similar gender distribution, with 81.2% males and 18.8% females, and no statistically significant differences were observed in any demographic characteristic, confirming homogeneity between groups.
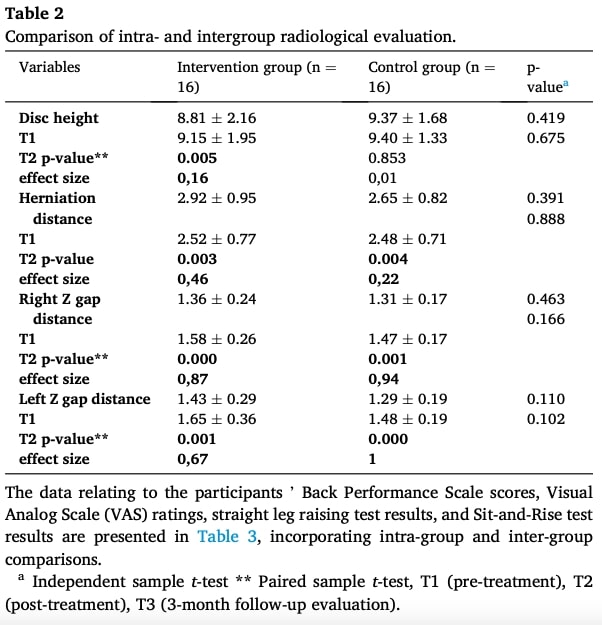
In the between-group analyses (pre- to post-treatment), radiological findings revealed a significant increase in disk height in the intervention group, whereas no such change was observed in the control group. Both groups showed a reduction in herniation distance, with the effect being approximately twice as pronounced in the intervention group. Right and left Z gap distances also increased significantly within both groups. However, between-group comparisons showed no statistically significant differences between the intervention and control groups for any of the radiological parameters.
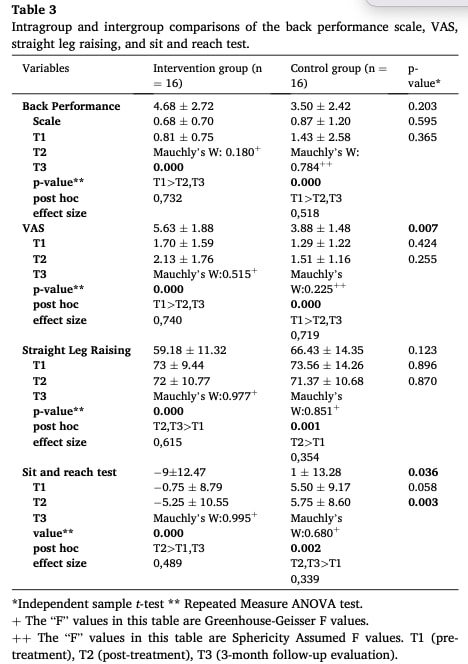
Clinically, both groups experienced significant improvements in pain (VAS), functional performance (Back Performance Scale), straight leg raise angle, and sit-and-reach flexibility, with changes generally emerging at early follow-ups. Effect sizes were consistently larger in the intervention group, yet no statistically significant differences were observed between groups in post-treatment comparisons.
Câu hỏi và suy nghĩ
One question is whether the authors adequately controlled for the home exercise program (HEP). Were patients actually performing the exercises at the prescribed intensity and frequency? A follow-up phone meeting was mentioned, but no home exercise adherence data were provided in the results.
Another point concerns the physiotherapist delivering the intervention. Since only one therapist was involved, and no information is provided about whether he had specific manual therapy certifications, the results can only be interpreted as: “mobilization for disc herniation regression performed by this particular physiotherapist was associated with decreased lumbar disc herniation.” This limits the generalizability of the findings.
In terms of patient selection, no formal classification system was used to guide treatment pathways. The only classification criteria were radiological findings, which are known to correlate poorly with patients’ symptoms.
The educational component of the intervention is also debatable. In light of recent literature, the notion of “safe movements for the spine” or the need to stabilize the back in a neutral position is increasingly questioned. Furthermore, the mobilization techniques, stabilization exercises, and educational content are contradictory. The manual techniques promote lumbar flexion (although the degree of spinal flexion in Figure 4 is questionable), while the stabilization exercises foster a neutral spine and bracing. This conflicting approach may induce kinesiophobia in some patients.
Another limitation is that no follow-up MRI at three months was performed, reportedly due to financial constraints. Such data would have provided valuable insights into the longer-term effects of mobilization for disc herniation regression.
Overall, the study found improvements in disc metrics within groups when comparing pre- and post-intervention, but no significant differences between groups. There is evidence in the literature that disc herniations can regress spontaneously through the natural healing process. This could partly explain the reductions in herniation distance observed in both groups of this study. Given the small sample size and the methodological limitations, more thoroughly discussed in the Talk nerdy to me section, the conclusions of this study should be interpreted with caution.
Nói chuyện với tôi một cách ngớ ngẩn
The presentation of Tables 2 and 3 is fundamentally unclear, which significantly hinders straightforward interpretation of the results. A major issue is evident in Table 3, where numerical data for the crucial post-treatment (T2) time point are completely absent, leaving only p-values. This omission prevents readers from assessing the magnitude of the reported changes. Moreover, the labeling within the tables is ambiguous; for example, a single value presented in the “Disc height” row does not specify whether it corresponds to the baseline (T1) or another measurement, creating uncertainty about potential misalignment of the entire data set. This lack of clarity in basic data presentation severely undermines confidence in the reported findings.
In addition to the tabular issues, the statistical reporting raises further concerns. The methodology used to calculate effect sizes is not specified, leaving it unclear whether these values reflect Cohen’s d, partial eta-squared, or another metric. This omission is particularly troubling because some reported effect sizes appear unusually high, such as 0.94 for the control group’s “Right Z gap distance” in Table 2, which requires explicit justification. Finally, the use of “p = 0.000” is a statistically improper convention, as a p-value can never be exactly zero; standard practice is to report such results as “p < 0.001.” These recurring issues collectively detract from the study’s statistical credibility and limit confidence in its conclusions.
Những thông điệp mang về nhà
Within-group analyses improvements were observed in the intervention group for:
- Disc height (significant increase)
- Herniation distance (greater reduction than control group)
- Right and left Z gap distances
- Clinically, both groups improved in:
- Pain (VAS)
- Functional performance (Back Performance Scale)
- Straight leg raise angle
- Lumbar flexibility (sit-and-reach test)
Effect sizes were consistently larger in the intervention group, though inter-group comparisons showed no statistically significant differences for radiological or clinical outcomes.
The results of this study are limited by significant methodological concerns.
- Small sample size (32 participants completed the study)
- Single physiotherapist delivering the intervention and assessing the patients
- Home exercise program adherence not objectively measured
- Short-term follow-up (no 3-month MRI to assess structural changes)
- Methodological and statistical reporting issues (ambiguous tables, unclear effect size calculations, improper p-value reporting)
- No formal classification system to guide individualized treatment
Practical Messages for Physiotherapists:
The findings of this study should be interpreted with caution due to concerns regarding the statistical reporting. Nevertheless, spinal mobilization can be safely incorporated as part of a comprehensive management plan for patients with discogenic low back pain. While the precise mechanisms of manual therapy remain unclear, some biomechanical effects of mobilization for disc herniation regression have been suggested, as highlighted in this Physiotutors review.
Furthermore, this article provides a comprehensive, evidence-based overview of lumbar disc herniation, exploring the underlying mechanisms and effective management strategies.
Thẩm quyền giải quyết
CẢI THIỆN ĐÁNG KỂ KIẾN THỨC CỦA BẠN VỀ ĐAU LƯNG DƯỚI MIỄN PHÍ
5 bài học cực kỳ quan trọng mà bạn sẽ không được học ở trường đại học, giúp cải thiện việc chăm sóc bệnh nhân đau lưng dưới ngay lập tức mà không phải trả một xu nào
