
Bài tập nghiên cứu ngày 15 tháng 5 năm 2025
Sức mạnh cơ bắp và thể lực tim mạch ảnh hưởng đến khả năng sống sót của bệnh nhân ung thư như thế nào: Tổng quan có hệ thống và phân tích tổng hợp

Giới thiệu
Thể lực, đặc biệt là sức mạnh cơ bắp và sức khỏe tim mạch (CRF) đóng vai trò quan trọng trong việc sống sót sau ung thư. Bằng chứng mới xuất hiện cho thấy những yếu tố này có thể ảnh hưởng đáng kể đến nguy cơ tử vong ở những bệnh nhân đã được chẩn đoán mắc bệnh ung thư, tuy nhiên hầu hết các nghiên cứu đều tập trung vào nhóm dân số khỏe mạnh trước khi phát triển bệnh ung thư. Các đánh giá đơn giản, khả thi về mặt lâm sàng như sức mạnh cầm nắm (HGS) và bài kiểm tra đi bộ 6 phút (6MWT) cho thấy giá trị tiên lượng mạnh mẽ, trong khi các biện pháp tiên tiến như bài kiểm tra gắng sức tim phổi (CPET) cung cấp thông tin chi tiết sâu hơn. Các nghiên cứu gần đây chỉ ra rằng sức mạnh cơ bắp cao hơn có thể làm giảm tỷ lệ tử vong do mọi nguyên nhân lên đến 39% (Ezzatvar, 2021) và CRF vượt trội có thể làm giảm nguy cơ tới 48% (Ezzatvar, 2021) nhưng vẫn còn nhiều khoảng cách - đặc biệt là liên quan đến tỷ lệ tử vong do ung thư, loại khối u và giai đoạn bệnh.
Bài đánh giá có hệ thống và phân tích tổng hợp này nhằm mục đích làm rõ những mối liên hệ này, giúp các nhà vật lý trị liệu tối ưu hóa các biện pháp can thiệp bằng bài tập cho bệnh nhân ung thư ở các giai đoạn tiến triển khác nhau bằng cách làm rõ mối quan hệ giữa thể lực và khả năng sống sót sau ung thư.
Phương pháp
Tiêu chuẩn đủ điều kiện
Các nghiên cứu được lựa chọn dựa trên việc đánh giá thể lực và kết quả sống sót sau ung thư ở bệnh nhân trưởng thành. Các nhà nghiên cứu đã tiến hành tìm kiếm có hệ thống trên các cơ sở dữ liệu khoa học sức khỏe lớn để xác định các nghiên cứu theo dõi quan sát triển vọng nhằm điều tra mối quan hệ giữa sức mạnh cơ bắp, sức khỏe tim mạch hô hấp (CRF) và tỷ lệ tử vong ở bệnh nhân ung thư trưởng thành (≥18 tuổi). Chỉ những nghiên cứu báo cáo tỷ lệ tử vong do mọi nguyên nhân hoặc do ung thư mới được đưa vào, trong khi những nghiên cứu trình bày tỷ lệ chênh lệch (OR), ấn phẩm không phải bằng tiếng Anh hoặc dữ liệu không đủ sẽ bị loại trừ.
Thể lực được đánh giá bằng hai phương pháp phân tích:
- Phương pháp cắt bỏ (ví dụ: so sánh nhóm có sức mạnh cơ/CRF cao so với thấp).
- Phương pháp tăng dần đơn vị (ví dụ: đánh giá rủi ro tử vong trên mỗi mức tăng 1-MET trong CRF).
Nghiên cứu này nhằm xác định mức độ thể lực ban đầu và những cải thiện gia tăng ảnh hưởng như thế nào đến kết quả sống sót ở bệnh nhân ung thư.
Trích xuất dữ liệu và đánh giá chất lượng nghiên cứu
Các nhà đánh giá độc lập đã thực hiện trích xuất dữ liệu. Nhóm nghiên cứu đã thu thập một cách có hệ thống: đặc điểm nghiên cứu (quy mô mẫu, thiết kế, thời gian theo dõi); thông tin nhân khẩu học của người tham gia (tuổi, BMI); các thông số lâm sàng (loại ung thư, giai đoạn, phác đồ điều trị); và các biện pháp thể lực (sức mạnh cơ bắp và/hoặc phương pháp đánh giá CRF với giá trị ngưỡng). Đối với kết quả, Tỷ lệ nguy cơ (HR) với khoảng tin cậy 95% hoặc sai số chuẩn đã được trích xuất cho cả tỷ lệ tử vong do mọi nguyên nhân và do ung thư từ các phân tích đơn biến và đa biến có sẵn. Chất lượng của các nghiên cứu sau đó được đánh giá bằng thang đánh giá chất lượng Newcastle-Ottawa cho các nghiên cứu theo nhóm. Thang đo này đánh giá ba lĩnh vực: Lựa chọn nhóm đối tượng nghiên cứu, khả năng so sánh giữa các nhóm đối tượng nghiên cứu và xác định kết quả mong muốn.
Statistical analysis
Nghiên cứu này sử dụng phân tích tổng hợp để kiểm tra sức mạnh cơ bắp và sức khỏe tim mạch (CRF) ảnh hưởng như thế nào đến tỷ lệ tử vong do mọi nguyên nhân và do ung thư. Các nhà nghiên cứu đã tổng hợp tỷ lệ nguy cơ (HR) từ các nghiên cứu trước đây bằng cách sử dụng mô hình hiệu ứng ngẫu nhiên. Họ so sánh nhóm có cường độ/CRF cao so với thấp dựa trên ngưỡng xác định trước và phân tích những thay đổi trên mỗi đơn vị tăng (ví dụ, trên mỗi 1 kg hoặc cải thiện 1-MET). Ý nghĩa thống kê được đặt ở mức *p* ≤ 0,05 và tính không đồng nhất được đánh giá bằng cách sử dụng I² và kiểm định Cochran's Q. Phân tích độ nhạy và độ lệch công bố đã được thực hiện. Các phân nhóm bao gồm giai đoạn và loại ung thư.
Kết quả
Đặc điểm của người tham gia và can thiệp
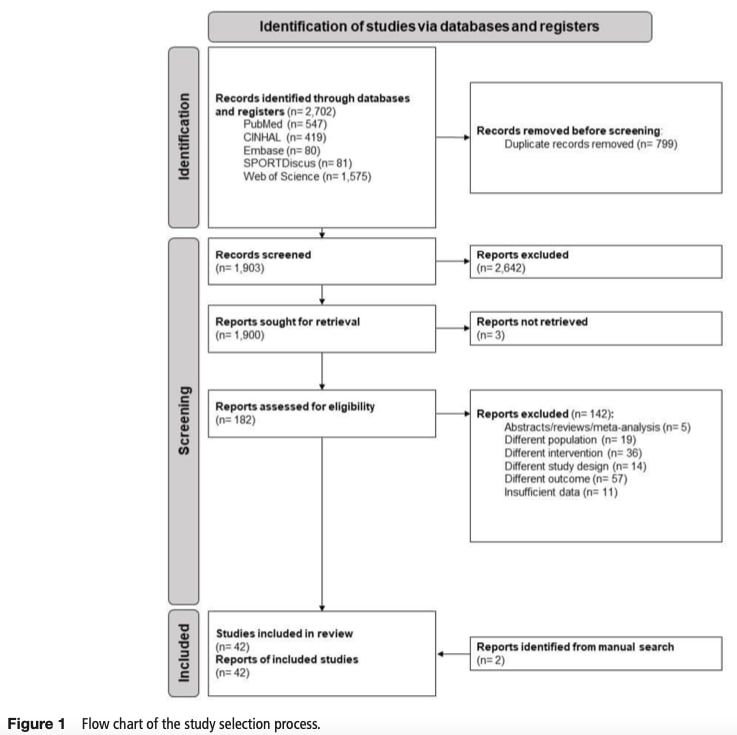
Quá trình đánh giá có hệ thống đã xác định được 2702 nghiên cứu điều tra về thể lực và khả năng sống sót sau ung thư, trong đó có 42 nghiên cứu đáp ứng tiêu chí đưa vào phân tích tổng hợp. Các nghiên cứu này đã tuyển chọn 46.694 bệnh nhân ung thư trưởng thành có độ tuổi trung bình là 64 và BMI trung bình là 24,8 kg/m². Các nghiên cứu được đưa vào đại diện cho nhiều loại ung thư khác nhau, bao gồm ung thư phổi (9 nghiên cứu), dạ dày (2), tuyến tụy (1), vú (1), u thần kinh đệm (1) và ung thư ruột kết/bàng quang (mỗi loại 1), với 26 nghiên cứu kiểm tra nhiều loại ung thư.
Đo sức mạnh cơ bắp
Tất cả các nghiên cứu đều đánh giá sức mạnh cơ bằng phương pháp đo lực nắm tay (HGS). Mười chín nghiên cứu đã sử dụng giá trị ngưỡng để phân loại bệnh nhân thành nhóm có sức mạnh cao so với nhóm có sức mạnh thấp, với ngưỡng dao động từ <13 kg đến <25,1 kg đối với phụ nữ và <19,87 kg đến <40,2 kg đối với nam giới. Một số nghiên cứu sử dụng các phương pháp phân loại thay thế bao gồm chỉ số suy nhược hoặc phần trăm điều chỉnh theo độ tuổi. Các nghiên cứu phân tích sức mạnh như một biến liên tục (thay đổi theo đơn vị gia tăng), đã kiểm tra nguy cơ tử vong trên mỗi 1 kg gia tăng.
Đo lường CRF
Thể lực tim mạch được đánh giá thông qua thử nghiệm gắng sức tim phổi (CPET) (14 nghiên cứu) và thử nghiệm đi bộ 6 phút (4 nghiên cứu). CRF thấp được xác định bằng nhiều tiêu chí bao gồm VO₂peak <13-16 mL/kg/phút, tỷ lệ thông khí phút (VE) so với lượng carbon dioxide thải ra (VCO₂) VE/VCO₂ ≥31 hoặc khoảng cách 6MWT <358,5m đến <400 m. Bảy nghiên cứu đã xem xét CRF như một biến liên tục trên mỗi đơn vị gia tăng trong VO₂peak, MET hoặc khoảng cách đi bộ.
Sức mạnh cơ bắp: tử vong do mọi nguyên nhân.
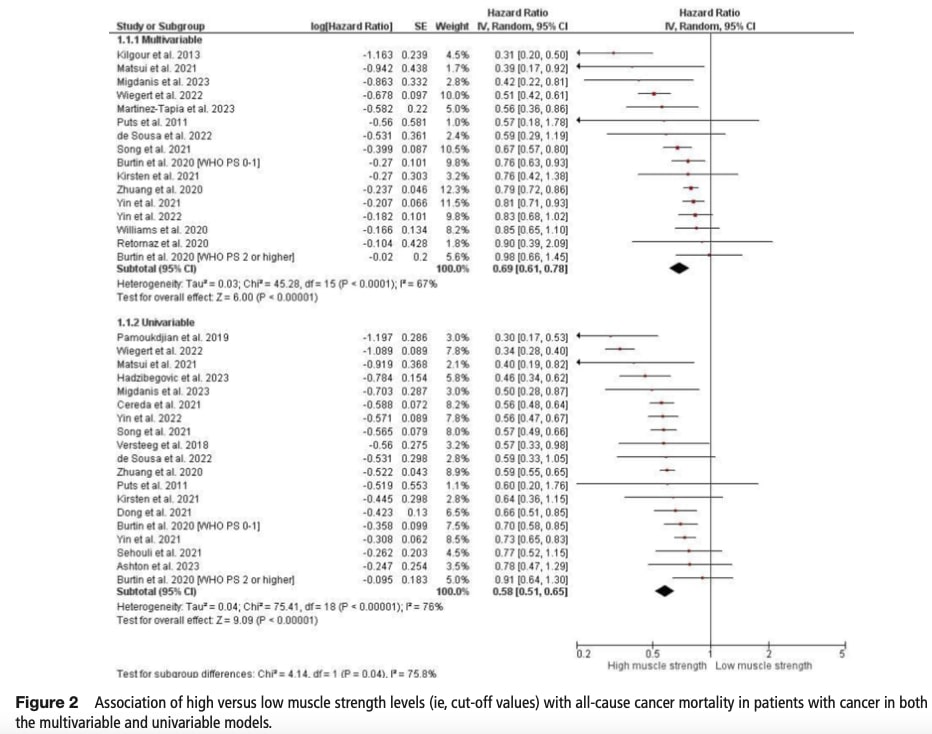
Giá trị cắt bỏ
Trong phân tích đa biến của 22 nghiên cứu, sức mạnh cơ bắp cao có liên quan đến nguy cơ tử vong thấp hơn 31%. Độ không đồng nhất ở mức trung bình (I2 = 67%). Mối liên hệ bảo vệ này rõ rệt hơn ở những bệnh ung thư giai đoạn tiến triển (giảm nguy cơ 23-46%) so với bệnh giai đoạn đầu (không đáng kể). Các mô hình đơn biến cho thấy hiệu quả tương tự nhưng mạnh hơn với nguy cơ tử vong thấp hơn 50% đối với các nghiên cứu có hơn 75% người tham gia mắc bệnh ung thư giai đoạn tiến triển. Tỷ lệ tử vong giảm liên tục chứng minh giá trị tiên lượng của mối liên hệ giữa thể lực và khả năng sống sót sau ung thư, đặc biệt là ở giai đoạn tiến triển của bệnh . Những bệnh nhân ung thư tiêu hóa có sức mạnh cơ bắp cao có nguy cơ tử vong thấp hơn 41% so với những người có sức mạnh cơ bắp thấp hơn. Tương tự như vậy, trong số những bệnh nhân ung thư phổi, sức mạnh cơ bắp cao hơn có liên quan đến việc giảm 19% nguy cơ tử vong do mọi nguyên nhân. Khi xem xét các phân tích đơn biến đối với các loại ung thư này, nguy cơ tử vong giảm 38% đối với ung thư tiêu hóa và 26% đối với ung thư phổi. Đáng chú ý, tính không đồng nhất giữa các nghiên cứu về các loại ung thư này là không có (I² = 0%), cho thấy những phát hiện nhất quán.
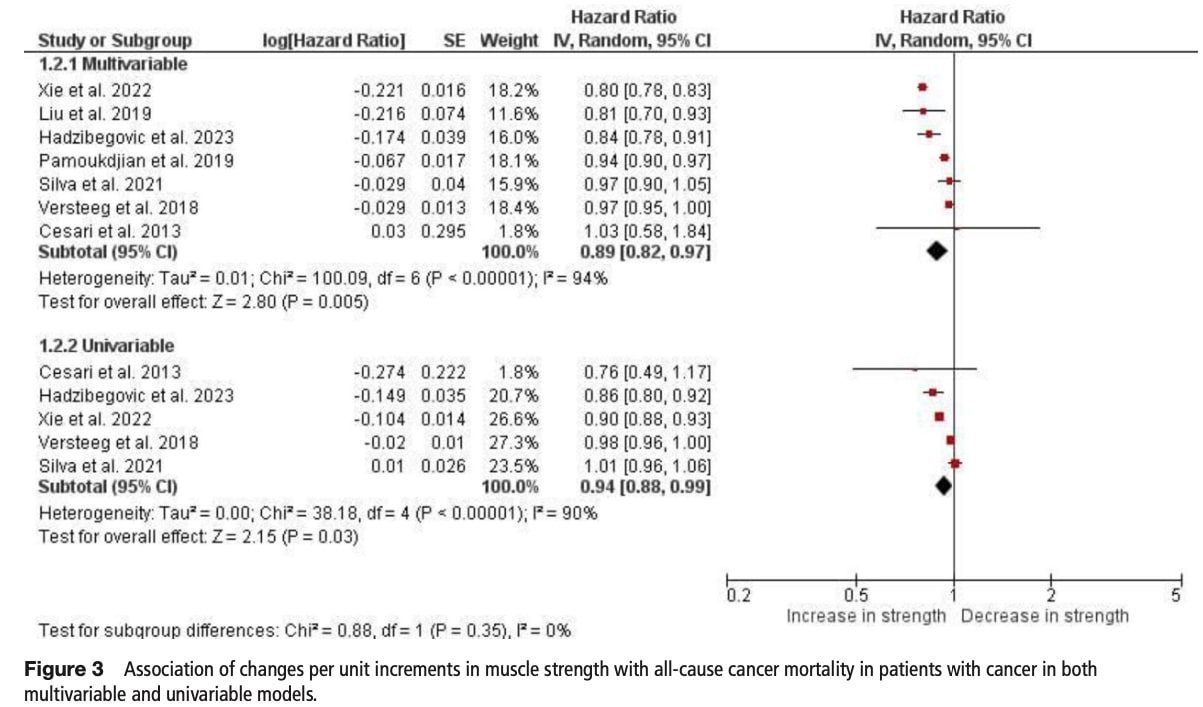
Giá trị gia tăng
Mỗi lần tăng thêm 1 kg sức mạnh có liên quan đến việc giảm 11% tỷ lệ tử vong trong các mô hình đa biến mặc dù có sự không đồng nhất đáng kể (I2 = 94%). Những phát hiện tương tự đã được tìm thấy trong phân tích đơn biến (giảm 6%). Lợi ích rõ ràng nhất ở những bệnh ung thư ở giai đoạn tiến triển trung bình (giảm 20% cho mỗi đơn vị gia tăng). Không có đủ số lượng nghiên cứu xem xét những thay đổi về tỷ lệ tử vong trên mỗi đơn vị gia tăng khi phân tầng theo loại ung thư.
Sức khỏe tim mạch: tất cả nguyên nhân gây tử vong.
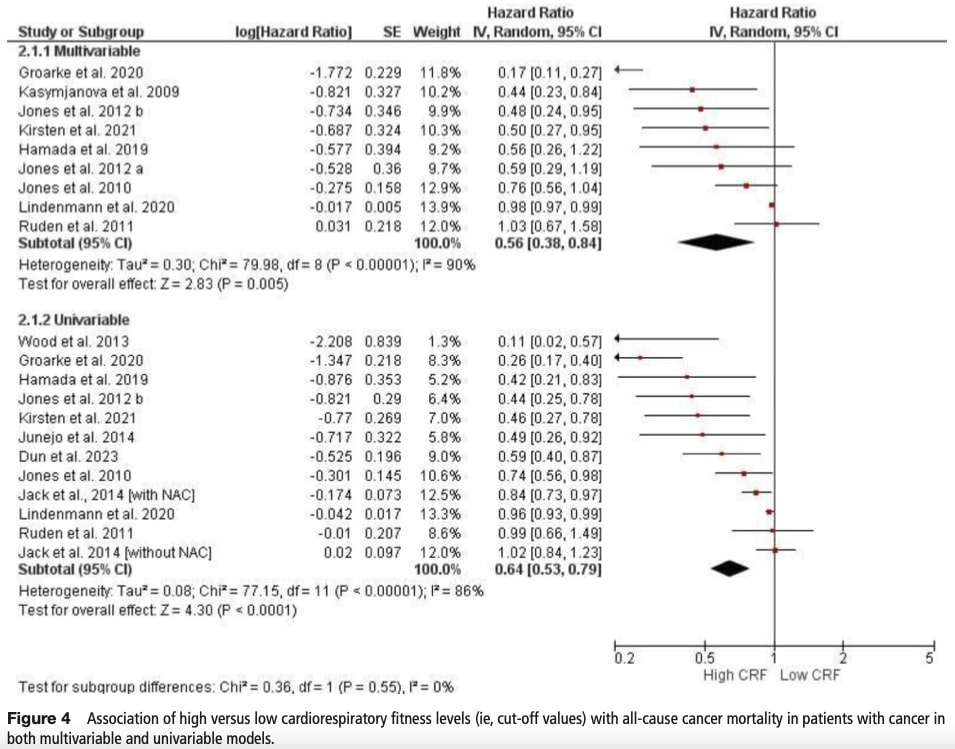
Phân tích cắt bỏ
Trong phân tích đa biến, mức CRF cao cho thấy nguy cơ tử vong thấp hơn 46% so với những người có mức CRF thấp hơn. Tuy nhiên, tính không đồng nhất là đáng kể I2=90%. Các mô hình đơn biến cho thấy tác động giảm nhẹ nhưng đáng kể (giảm 36%). Phân tích đa biến báo cáo rằng bệnh nhân ung thư phổi biểu hiện lợi ích đặc biệt mạnh mẽ (giảm 31%). Phân tích đơn biến cho thấy hiệu quả tương tự nhưng mạnh hơn một chút, với mức giảm 35% nguy cơ tử vong. Đối với ung thư tiêu hóa và huyết học, chỉ có các mô hình đơn biến và không báo cáo mối liên hệ đáng kể giữa tình trạng tim mạch và tỷ lệ tử vong. Ở những bệnh ung thư giai đoạn đầu, CRF cao cho thấy khả năng giảm tỷ lệ tử vong không đáng kể trong các mô hình đã điều chỉnh, với tính không đồng nhất vừa phải cho thấy tác động phụ thuộc vào quần thể.
Giá trị gia tăng
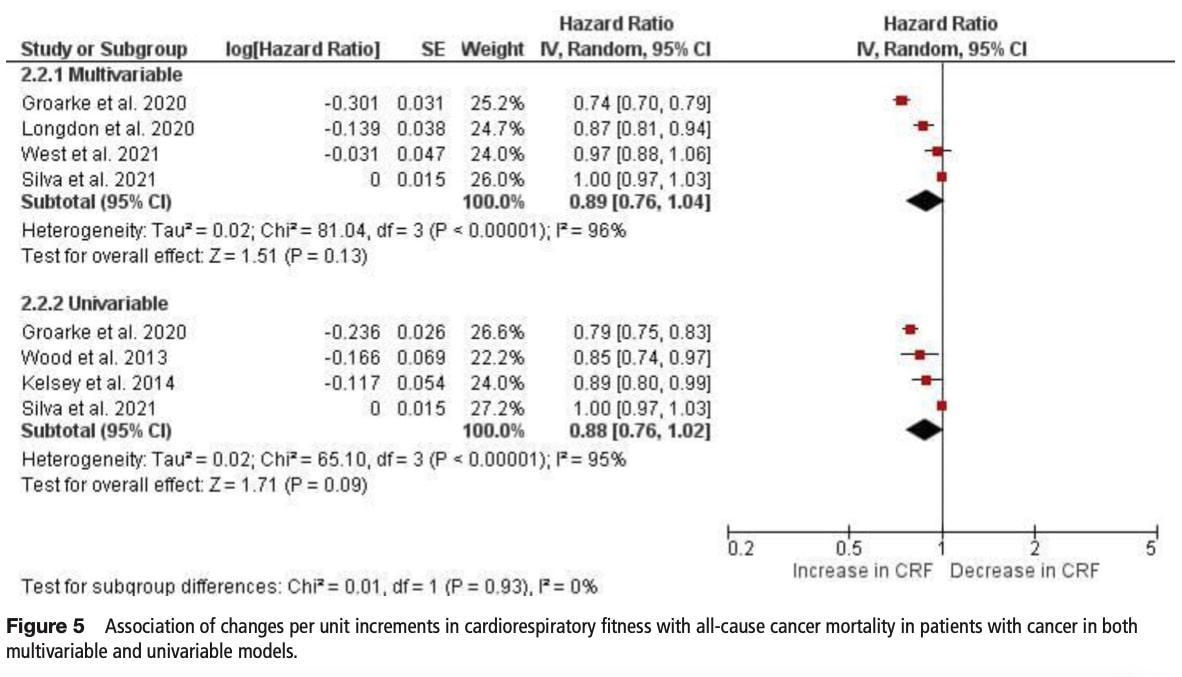
Sự gia tăng CRF trên mỗi đơn vị cho thấy tỷ lệ tử vong giảm không đáng kể (11-12%) trong cả mô hình đa biến và đơn biến, với sự không đồng nhất đáng kể được quan sát thấy (I²>95%). Kết quả tương tự xuất hiện từ mô hình đơn biến. Không đủ số lượng nghiên cứu xem xét những thay đổi về tỷ lệ tử vong do tình trạng tim mạch hô hấp trên mỗi đơn vị gia tăng khi phân tầng theo loại ung thư và giai đoạn ung thư.
Thể lực tim mạch và tỷ lệ tử vong do ung thư.
Phân tích cắt bỏ
CRF cao cho thấy tỷ lệ tử vong giảm không đáng kể (66% trong mô hình đã điều chỉnh, 49% trong mô hình chưa điều chỉnh) với tính không đồng nhất cực độ (I²>94%). Có ít dữ liệu có sẵn để kiểm tra mối quan hệ giữa CRF và tỷ lệ tử vong ở các loại và giai đoạn ung thư cụ thể.
Giá trị gia tăng
Hai nghiên cứu phát hiện ra rằng mỗi đơn vị CRF tăng thêm có liên quan đến nguy cơ tử vong do ung thư thấp hơn 18% trong các mô hình điều chỉnh. Tuy nhiên, tính không đồng nhất là đáng kể (I2 = 90%). Không có đủ số lượng nghiên cứu để kiểm tra nguy cơ tử vong do ung thư trên mỗi đơn vị gia tăng CRF khi phân tầng theo giai đoạn và loại ung thư.
Câu hỏi và suy nghĩ
Bài đánh giá có hệ thống này đã xem xét cả phân tích đa biến và đơn biến từ các nghiên cứu theo dõi quan sát có triển vọng. Mặc dù các nghiên cứu này tiết lộ những mối liên hệ quan trọng, nhưng điều quan trọng cần nhớ là chúng chỉ có thể xác định mối tương quan chứ không thể thiết lập mối quan hệ nhân quả giữa thể lực và khả năng sống sót sau ung thư. Thiết kế quan sát có nghĩa là chúng ta phải giải thích kết quả một cách thận trọng, đặc biệt là vì các phân tích đơn biến có xu hướng đánh giá quá cao tác động của sức mạnh và thể lực tim mạch lên nguy cơ tử vong do không tính đến các biến số gây nhiễu tiềm ẩn.
Một số hạn chế xuất hiện từ những bằng chứng hiện tại. Tính không đồng nhất cao giữa các nghiên cứu (với giá trị I² thường vượt quá 50%) cho thấy sự thay đổi đáng kể trong quần thể bệnh nhân, phương pháp đánh giá và biện pháp đánh giá kết quả. Sự không đồng nhất này, kết hợp với báo cáo không đầy đủ về các biến phụ thuộc đã điều chỉnh trong một số biến đa
phân tích, khiến việc phân lập các tác động cụ thể của thể lực trở nên khó khăn. Hơn nữa, sự hiểu biết chưa đầy đủ của chúng ta về tất cả các yếu tố ảnh hưởng đến tỷ lệ tử vong do ung thư làm phức tạp thêm nỗ lực xác định vai trò chính xác của sức mạnh và điều hòa tim mạch.
Việc triển khai thực tế gặp phải những rào cản thực tế. Bệnh nhân ung thư thường bị mệt mỏi do điều trị và các tác dụng phụ khác gây ra những thách thức đáng kể trong việc duy trì hoặc cải thiện thể lực. Những thực tế lâm sàng này phải được xem xét khi áp dụng những phát hiện này vào việc chăm sóc bệnh nhân, vì quần thể nghiên cứu có thể không đại diện đầy đủ cho trải nghiệm chung của bệnh nhân ung thư.
Nói chuyện với tôi một cách ngớ ngẩn
Để phân tích mối liên hệ giữa sức mạnh cơ bắp và sức khỏe tim mạch (CRF) với tỷ lệ tử vong, nghiên cứu đầu tiên đã thu thập tỷ lệ nguy cơ (HR) từ các nghiên cứu hiện có. Các HR này—cùng với khoảng tin cậy 95% (CI) của chúng—đã được điều chỉnh về mặt toán học để đảm bảo so sánh công bằng. Sau đó, một mô hình hiệu ứng ngẫu nhiên được sử dụng để kết hợp các kết quả, mô hình này giải thích rõ ràng sự khác biệt giữa các nghiên cứu bằng cách giả định rằng hiệu ứng thực sự của chúng thay đổi tự nhiên (ví dụ, do quần thể bệnh nhân khác nhau hoặc phương pháp đo lường khác nhau). Mô hình này bảo thủ hơn mô hình hiệu ứng cố định vì nó mở rộng khoảng tin cậy để phản ánh sự không chắc chắn này. Mô hình này gán trọng số lớn hơn cho các nghiên cứu chính xác hơn thông qua trọng số phương sai nghịch đảo, một phương pháp ưu tiên các ước tính có sai số chuẩn nhỏ hơn.
Đối với các nghiên cứu so sánh các hạng mục thể lực “cao so với thấp”, các ngưỡng giới hạn được xác định trước (như >19,1 kg đối với sức mạnh cơ bắp) sẽ chia những người tham gia thành các nhóm. Khi các nghiên cứu sắp xếp dữ liệu thành phần ba hoặc phần tư, chỉ có nhóm trên cùng và nhóm dưới cùng được phân tích để tối đa hóa độ tương phản. Một cách tiếp cận khác tập trung vào những thay đổi gia tăng, chẳng hạn như cách mỗi cải thiện 1-MET trong CRF ảnh hưởng đến nguy cơ tử vong.
Nhóm nghiên cứu đã đánh giá ý nghĩa thống kê bằng cách sử dụng ngưỡng giá trị *p* là 0,05. Để đánh giá xem kết quả nghiên cứu có mâu thuẫn hay không, họ đã tính toán tính không đồng nhất thông qua thống kê I² (giá trị trên 50% chỉ ra sự khác biệt đáng kể) và kiểm định Q của Cochran. Ví dụ, I² là 90% (như được thấy trong một số phân tích tại đây) cho thấy >90% sự khác biệt quan sát được giữa các nghiên cứu phản ánh sự không nhất quán thực sự chứ không phải lỗi ngẫu nhiên. Khi tính không đồng nhất cao, các ước tính gộp trở nên kém tin cậy hơn, các phân tích nhóm con có thể giải thích một phần những khác biệt này khi thấy ung thư giai đoạn đầu và giai đoạn tiến triển có kết quả khác nhau.
Các giá trị ngoại lệ tiềm ẩn được đánh dấu bằng phương pháp phân tích độ nhạy , trong đó mỗi nghiên cứu được tạm thời loại bỏ để kiểm tra tác động của nó ( phương pháp loại trừ một ). Độ lệch trong công bố - nguy cơ bỏ sót các nghiên cứu tiêu cực - được đánh giá bằng biểu đồ phễu và kiểm định Egger , giúp phát hiện sự mất cân bằng trong các tác động của nghiên cứu nhỏ.
Phân tích nhóm con khám phá xem kết quả có khác nhau theo giai đoạn ung thư (giai đoạn sớm so với giai đoạn tiến triển) hoặc loại ung thư (ví dụ, ung thư phổi đơn thuần so với ung thư tiêu hóa theo nhóm). Tất cả các tính toán đều được thực hiện bằng Review Manager (RevMan) và gói metafor của R, các công cụ tiêu chuẩn cho phân tích tổng hợp.
Những thông điệp mang về nhà
Bằng chứng hiện tại cho thấy rõ ràng rằng việc cải thiện sức mạnh cơ bắp và sức khỏe tim mạch (CRF) ở bệnh nhân ung thư có thể làm giảm đáng kể nguy cơ tử vong do ung thư và do mọi nguyên nhân, mặc dù tác dụng bảo vệ chính xác cần được định lượng thêm do những hạn chế của nghiên cứu như tính không đồng nhất và quy mô mẫu nhỏ. Các mô hình lâm sàng chính xuất hiện:
- Sức mạnh quan trọng: Sức mạnh cơ bắp cao hơn luôn có liên quan đến nguy cơ tử vong thấp hơn 31-46% ở những bệnh nhân ung thư giai đoạn cuối, với những lợi ích đáng chú ý đối với bệnh ung thư tiêu hóa và phổi.
- Thể lực tim mạch: Mỗi lần tăng 1-MET trong CRF có thể làm giảm nguy cơ tử vong từ 11-18%, thậm chí còn mang lại lợi ích lớn hơn ở bệnh nhân ung thư phổi (giảm 31%).
- Hiệu ứng theo từng giai đoạn: Những mối liên kết bảo vệ này mạnh nhất ở những bệnh ung thư giai đoạn tiến triển, làm nổi bật vai trò quan trọng của phục hồi chức năng ngay cả trong quá trình chăm sóc giai đoạn cuối.
Ý nghĩa thực tế:
- Ưu tiên tập luyện sức đề kháng tiến triển để tăng cường sức mạnh (tập trung vào các nhóm cơ chính).
- Kết hợp các bài tập thể dục nhịp điệu (ví dụ như đi bộ, đạp xe) để cải thiện CRF, ngay cả ở mức khiêm tốn.
- Theo dõi tiến triển của bệnh nhân bằng các biện pháp chức năng (ví dụ: sức cầm nắm, 6MWT) cùng với các triệu chứng.
- Xác định và giải quyết các rào cản đối với hoạt động thể chất để thúc đẩy sự tuân thủ của bệnh nhân.
Mặc dù mối liên hệ giữa thể lực và khả năng sống sót sau ung thư đã được ghi nhận rõ ràng, nhưng các yếu tố lâm sàng khác cũng ảnh hưởng đáng kể đến kết quả. Đánh giá của chúng tôi cung cấp phân tích toàn diện về các yếu tố rủi ro tương tác này.
Thẩm quyền giải quyết
Dinh dưỡng có thể là yếu tố quan trọng đối với sự nhạy cảm trung tâm - Bài giảng video
Xem bài giảng video MIỄN PHÍ này về Dinh dưỡng và Nhạy cảm trung ương của nhà nghiên cứu về chứng đau mãn tính số 1 Châu Âu Jo Nijs. Những thực phẩm mà bệnh nhân nên tránh có thể sẽ khiến bạn ngạc nhiên!
