
Research
Muscle & Tendon
April 3, 2025
กลไกทางชีวภาพของการวิ่งเร็วที่เกี่ยวข้องกับการบาดเจ็บกล้ามเนื้อต้นขาด้านหลังในนักฟุตบอลชาย

การแนะนำ
Hamstring strain injuries (HSIs) remain one of the most prevalent musculoskeletal injuries in elite football, with incidence rates doubling over the past two decades. While traditional risk factors for hamstring strains – including previous injury, eccentric hamstring strength deficits, and running load – are well-established, however the relation between sprinting mechanics and hamstring strain risk remains controversial – despite being frequently targeted in prevention programs.
This gap between clinical practice and evidence highlights the need for practical, field- based assessment tools. While the three-dimensional motion capture (3DMoCap) technology is the gold standard for biomechanical assessment, Sprint Mechanics Assessment Score (S-MAS) offers a more clinically feasible solution, using simple video analysis to evaluate potentially risky movement patterns.
This study investigates whether the S-MAS can help clinicians predict and prevent hamstring injuries, bridging the gap between biomechanical research and real-world sports medicine practice.
Method
This 6-month prospective cohort study tracked elite football players to investigate sprinting mechanics and hamstring strain risk. The methodology adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for rigorous observational research reporting.
This prospective study included outfield players from professional English football clubs who were medically cleared for full participation and at least 18 years old. Goalkeepers were excluded and players returning from recent surgery (within 6 months) were also excluded to avoid confounding factors. Nine clubs initially participated, with one excluded for not meeting age criteria.
To determine how many players were needed for the study, researchers first analyzed injury data from one soccer club. They used this pilot data – which showed a 22% injury rate – to run a power calculation with G*Power software. The analysis indicated they needed 100 total participants to have a 90% chance of detecting true injury pattern
differences while keeping the false alarm rate at 5%. The study was designed to include four uninjured players for every one injured player (1:4 ratio) to ensure proper comparisons could be made.
Data collection
Participants performed two maximal 35m sprints following a standardized warm-up and submaximal build-up runs (80-90% effort). Testing occurred either preseason (June- August) or in-season (October-March) on natural grass or artificial turf, with players wearing their preferred football boots. The two sprint trials were recorded to ensure that right and left limbs were recorded properly.
S-MAS scoring
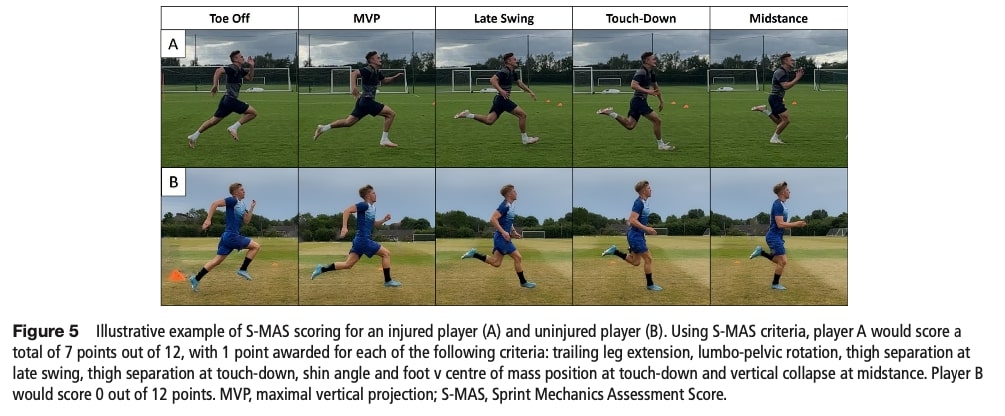
A single biomechanist with 10 years of experience, blinded to injury outcomes, assessed all sprint trials using the 12-item Sprint Mechanics Assessment Score (S-MAS). The analysis was conducted frame-by-frame using Kinovea video analysis software. Each of the 12 kinematic features was scored dichotomously: one point for the presence of a suboptimal movement pattern and zero points for its absence. This yielded a total score ranging from 0 (indicating optimal sprint mechanics) to 12 (reflecting multiple observable deficits), with higher scores corresponding to progressively poorer movement quality.
Hamstring injury reporting
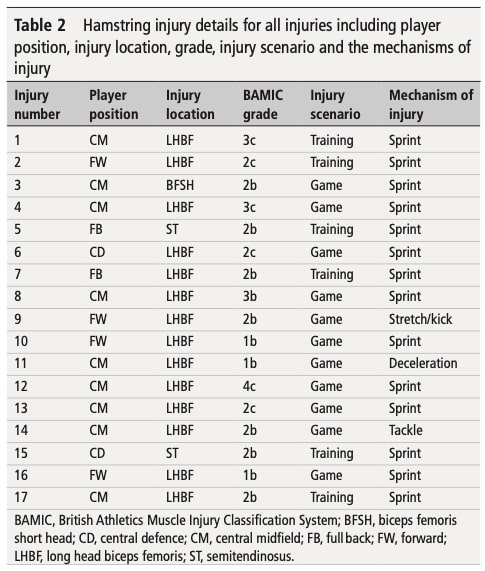
The study analyzed both retrospectively reported (12-month recall, medically verified) and prospectively occurring (6-month follow-up, MRI-confirmed) sprint-related HSIs. Retrospective data captured injury mechanism and laterality through player interviews and medical record review. Prospective injuries were clinically documented with MRI- based muscle localization and graded using the British Athletics classification. To minimize confounding, athletes sustaining severe non-hamstring injuries (>28 days absence) were excluded from controls, ensuring comparable training exposures between groups. Combining retrospective and prospective analyses allowed researchers to reliably associate specific sprinting mechanics and hamstring strain risk.
Statistical analyses
Analyses (Stata/JASP) included normality/variance testing (Shapiro-Wilk, Levene’s), with group comparisons via t-tests or Mann-Whitney U tests. Retrospectively, S-MAS scores differed between previously injured and uninjured players (Mann-Whitney U). Prospectively, MRI-confirmed HSIs were linked to S-MAS (primary predictor) using similar methods, with injured limbs compared to randomly selected uninjured limbs. Effect sizes (Hedges’ g) quantified magnitude. Kruskal-Wallis tests compared S-MAS across first-time, recurrent, and uninjured subgroups. Poisson regression modeled S- MAS as an HSI predictor, adjusting for age/prior injury (IRRs reported). ROC curves identified an optimal S-MAS risk threshold.
ผลลัพธ์
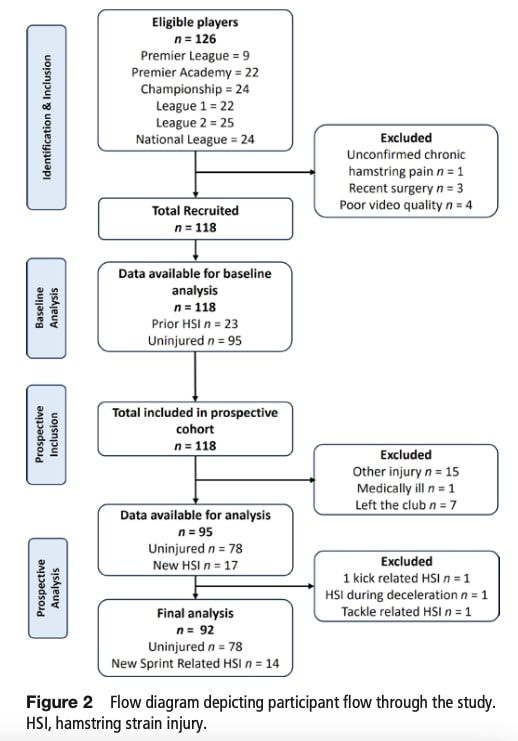
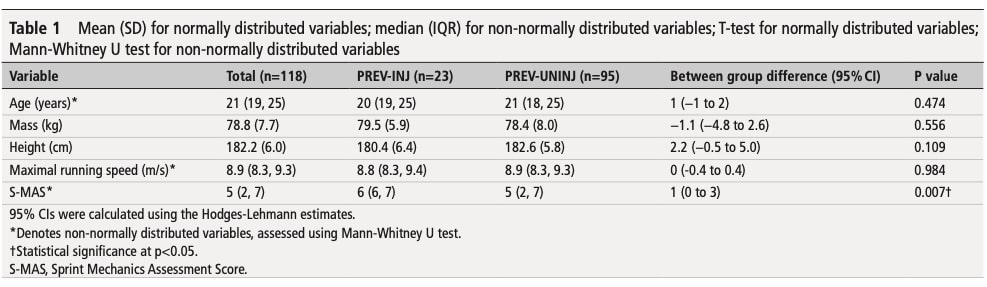
This investigation enrolled 126 male professional footballers from eight English clubs spanning Premier League to National League divisions. The retrospective analysis included 118 players, with 23 classified as previously injured (PREV-INJ) and 95 as uninjured (PREV-UNINJ), showing comparable physical characteristics (height ~181-183 cm, mass ~78-80 kg).
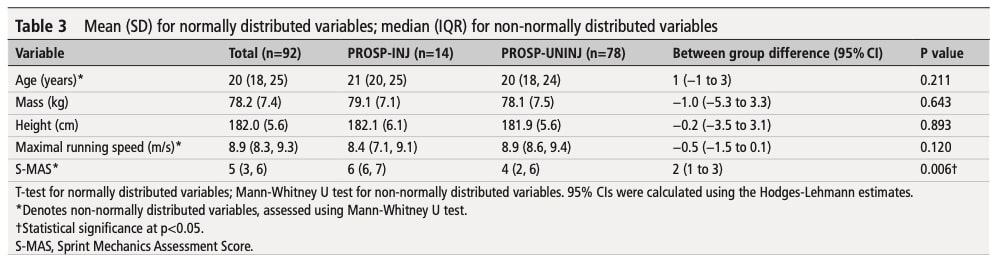
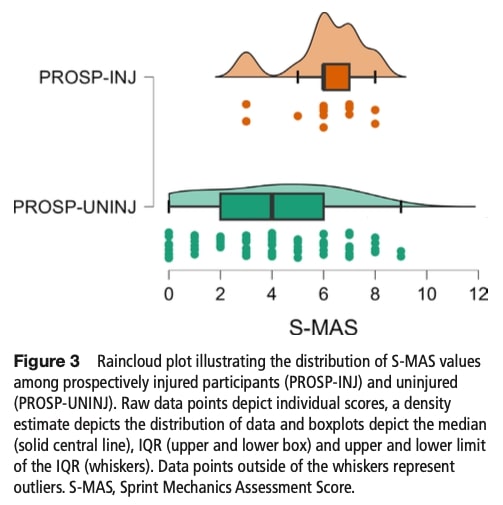
Prospective monitoring over six months retained 111 participants after excluding 7 lost to follow-up and 16 with severe non-hamstring injuries. Among 17 new hamstring injuries, 14 were sprint-related (PROSP-INJ group) and compared against 78 uninjured controls (PROSP-UNINJ). Three non-sprint HSIs were excluded to maintain mechanistic focus.
The retrospective analysis demonstrated that previously injured players (PREV-INJ) exhibited significantly higher S-MAS scores compared to uninjured counterparts (median 6 vs 5, p=0.007), with effect sizes ranging from trivial to large (Hedges’ g=0.17- 1.1).
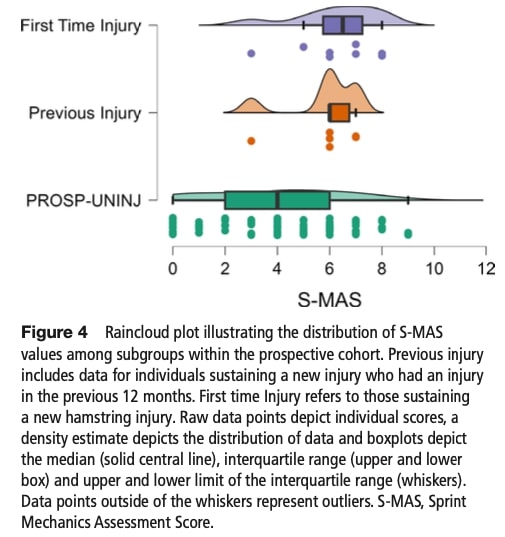
In the 6-month prospective analysis, players who sustained sprint-related hamstring injuries (PROSP-INJ) demonstrated significantly worse S-MAS scores than uninjured controls (median 6 vs. 4, p=0.006), with first-time injuries showing the most striking disparity (median 7 vs. 4, p=0.017). Each 1-point S-MAS increase raised injury risk by 33% (adjusted IRR=1.33, p=0.044), confirming a dose-response relationship. Receiver operating characteristic (ROC) analysis identified 5.5 as the optimal cutoff (AUC=0.732), with scores ≥6 yielding a clinically meaningful—though not statistically significant (p=0.065)—2.8-fold higher injury risk (95% CI: 0.94–8.35) compared to scores ≤5. Notably, the tool’s sensitivity (78.6%) outperformed its specificity (65.4%), prioritizing detection of true positives. Collectively, these results validate the S-MAS as a pragmatic screening tool to flag high-risk sprinting mechanics, particularly for first-time injuries, while underscoring the need for cautious interpretation of borderline significant thresholds.
Question and thoughts
This study offers important evidence linking poor sprinting mechanics and hamstring strain, providing clinicians with a practical field-based assessment tool. However, some limitations should be noted. Most significantly, the S-MAS hasn’t been validated against 3D motion capture systems – the gold standard for biomechanical analysis. The demonstrated correlation between higher S-MAS scores and injury occurrence is promising for clinical use, particularly given the tool’s simplicity and accessibility. However, before implementing it widely, we need larger prospective studies to: 1) establish definitive cutoff values, 2) verify its predictive accuracy across diverse populations, and 3) determine how it complements existing injury risk assessments. The current findings justify the S-MAS’s use as a screening tool, but practitioners should interpret scores cautiously and combine them with other clinical measures.
The prospective analysis, while methodologically sound, faces inherent challenges due to the smaller sample of injured players compared to uninjured controls—a common limitation in injury prediction studies. This imbalance, though unavoidable in prospective designs, may reduce statistical power to detect subtle but clinically meaningful differences. Despite limitations, the S-MAS provides a clinically useful composite evaluation of multiple biomechanical risk factors, enabling efficient identification of high-risk sprint patterns in field settings.
An important oversight is the lack of monitoring training load variables (volume, intensity), which are known moderators of injury risk. Fluctuations in workload— whether excessive spikes or inadequate conditioning—could confound the relationship between sprint mechanics and injury outcomes. Furthermore, the timing of assessments (preseason vs. in-season) introduces additional variability, as players’ mechanical efficiency and injury susceptibility may shift across different phases of the competitive calendar.
พูดจาเนิร์ดกับฉันสิ
The researchers analyzed S-MAS scores to identify biomechanical risk factors for hamstring injuries. They first confirmed the expected non-normal distribution of scores using Shapiro-Wilk tests and Q-Q plots – anticipating that injury-prone players would show distinct, elevated S-MAS values rather than clustering around the team average. This distribution pattern revealed:
- A majority group with typical mechanics
- A high-risk subgroup with poor technique (higher scores)
Since parametric tests would be inappropriate for this skewed data, they used Mann- Whitney U tests to reliably compare scores between injured and uninjured players. This approach specifically targeted detection of clinically significant biomechanical outliers rather than average population trends. For continuous variables like age or height that were normally distributed, they used t-tests.
After establishing these foundational comparisons, the researchers further quantified the practical importance of the differences using Hedges’ g effect sizes. While Mann- Whitney U tests confirmed that injured players had higher S-MAS scores, effect sizes revealed whether these differences were trivial (0.2), moderate (0.5), or large (0.8) in real-world terms. To address the nuanced question of how injury history influenced risk, they then employed Kruskal-Wallis tests with Dunn’s post hoc corrections. This allowed comparison across three critical subgroups: first-time injuries, recurrent injuries, and uninjured players—extending the initial injured/uninjured dichotomy. Together, this sequential analysis ensured not only statistical rigor but also clinical relevance, pinpointing exactly which athletes (e.g., those with first-time injuries and high S-MAS scores) faced the greatest risk.
Having established that injured players exhibited higher S-MAS scores through non- parametric comparisons (Mann-Whitney U) and quantified the magnitude of these differences (Hedges’ g), the researchers then addressed two critical clinical questions: How precisely does S-MAS predict injury risk? and What threshold should trigger intervention? To model the relationship between biomechanics and injury incidence over time, they employed Poisson regression—a method tailored for count data like injury events. This analysis revealed that each 1-point S-MAS increase raised injury risk by 33%, even after adjusting for confounders like age and prior injury, confirming its value as an independent predictor. However, to translate this continuous risk into actionable clinical practice, they used ROC curve analysis, which identified ≥6 as the optimal S-MAS cutoff. This threshold balanced sensitivity (detecting 78.6% of true injuries) with specificity (minimizing false alarms), providing coaches and clinicians with a clear benchmark for high-risk mechanics. Together, these advanced tests extended the initial findings beyond group comparisons, offering both granular risk quantification (Poisson) and a practical screening tool (ROC)—directly addressing the study’s goal of bridging sprinting mechanics and hamstring strain.
Take home message
Sprinting mechanics and hamstring strain: The S-MAS (Sprint Mechanics Assessment Score) serves as an effective field tool to detect high-risk athletes for sprint-related hamstring injuries (HSI). While valuable, it should be combined with:
Risk Stratification
A score of ≥6 serves as a preliminary risk threshold, correlating with significantly higher injury incidence in this study.
- Particular attention should be given to athletes with:
- Prior HSI history
- Reduced eccentric strength (Nordic hamstring exercise deficits)
Targeted Interventions
Address biomechanical flaws identified by S-MAS components (e.g., trunk lateral flexion, foot strike patterns) through:
- Technique modification drills (see Mendiguchia et al., 2023 for evidence-based strategies)
- Eccentric-strengthening protocols (e.g., Nordic hamstring curls)
- Pelvic/trunk stability work.
For Injury-Specific Rehabilitation:
Refer to this comprehensive guide on hamstring injury classification and return-to-sport protocols to tailor interventions to injury severity (e.g., British Athletics Muscle Injury Classification grades). https://www.physiotutors.com/fr/hamstring-injury-classification- and-rehabilitation/
Holistic Injury Prevention
While S-MAS focuses on mechanics, integrate these additional factors:
- Training load monitoring: Monitor internal load using both subjective RPE (Rating of Perceived Exertion) and objective on-field tracking data.
- Psychosocial factors: High perceived stress or sleep deprivation may compound biomechanical risks.
- Environmental controls: Surface hardness and cleat design can alter sprint kinematics.
อ้างอิง
ยกระดับการวินิจฉัยที่แตกต่างกันในการวิ่งเกี่ยวกับอาการปวดสะโพกที่เกี่ยวข้อง - ฟรี!
อย่าเสี่ยงต่อการพลาด สัญญาณเตือนที่อาจเกิดขึ้น หรือต้องเข้ารับการรักษาผู้วิ่งเนื่องจาก การวินิจฉัยที่ผิดพลาด ! เว็บสัมมนาครั้งนี้จะช่วยป้องกันไม่ให้คุณทำผิดพลาดแบบเดียวกับนักบำบัดหลายๆ คน!
