Research
Head/Neck
May 22, 2025
Cervicogenic Dizziness: Can Manual Therapy Decrease Intensity and Restore Neck Motion? A Systematic Review

การแนะนำ
Cervicogenic dizziness (CD) is a complex condition characterized by imbalance triggered by neck movements, often accompanied by pain, stiffness, and restricted cervical ROM. Emerging evidence suggests it stems from sensory-proprioceptive dysfunction in the cervical spine, with contributing factors including muscle tone abnormalities and joint receptor dysfunction. Symptoms—typically non-rotational dizziness, neck pain, and headaches—can last minutes to hours and worsen with stress or fatigue.
While physical therapy interventions (e.g., manual therapy, exercise, dry needling) show promise in reducing symptoms, high-quality evidence remains limited. This systematic review evaluates the effectiveness of manual therapy for cervicogenic dizziness, clarifying its role in improving dizziness intensity and cervical ROM to guide clinical decision-making.
วิธีการ
Two independent researchers conducted a systematic search of medical databases, including PubMed and Medline. Researchers included randomized controlled trials (RCTs) with at least 20 participants that scored ≥7 on the PEDro scale, focusing on adults aged 18+ diagnosed with cervicogenic dizziness. Eligible studies had to evaluate manual therapy for cervicogenic dizziness interventions (such as mobilization or manipulation) compared to control groups receiving placebo, no intervention, or alternative treatments and report outcomes including dizziness intensity, cervical range of motion, pain, disability, or dizziness frequency. Researchers excluded studies that examined non- manual therapies, dizziness from non-cervical causes, or those failing to assess our primary outcomes of dizziness intensity and cervical mobility. Data regarding study population, sample size, and patient characteristics were systematically extracted. The researchers used the PEDro scale to assess the methodological quality of studies, with a higher score out of 10 correlating with better quality in terms of internal validity, external validity, and statistical reporting. Risk of bias was evaluated using the Cochrane RoB 2.0 tool, which assesses selection bias, performance bias, detection bias, attrition bias, and reporting bias.
ผลลัพธ์
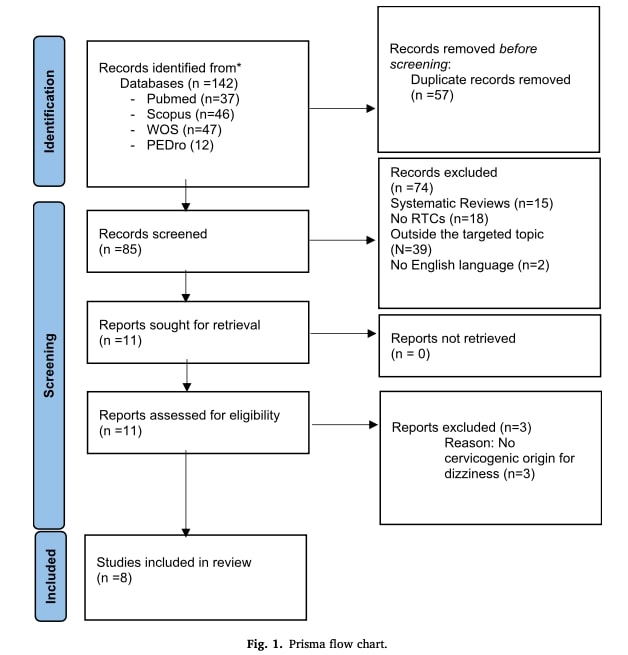
8 publications were included after the studies extraction process. The total number of participants across all studies was 312, with 140 females and 138 males. The mean age of participants was 53.27 years. Studies that did not report specific information on age or gender were excluded from this calculation. Among the eight included studies, four compared manual therapy for cervicogenic dizziness to a placebo treatment. Two studies evaluated a traction protocol combined with a high-speed manual therapy technique. One study investigated the effectiveness of Mulligan’s sustained natural apophyseal glides (SNAGs), while another compared a multimodal approach with and without the addition of a traction-extension maneuver.
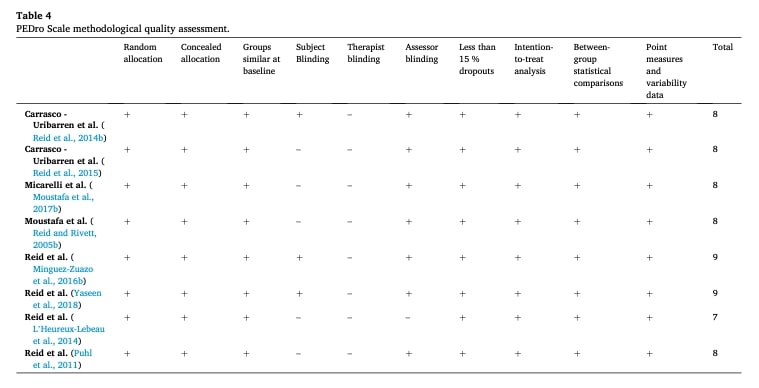
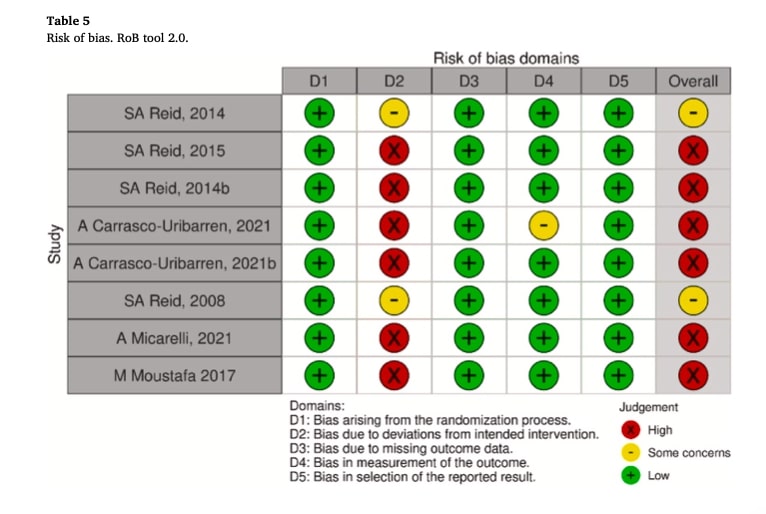
According to the PEDro scale, all included studies were rated as “good” or higher. In none of the studies were the therapists blinded. However, in all studies except one, the examiners were blinded. Table 4 provides more detailed information regarding the methodological quality of the included studies. Regarding the risk of bias, Table 5 highlights the main concerns, which stem from deviations from the intended interventions, resulting in an overall high risk of bias.
The outcome measures used across the four domains—cervical range of motion (ROM), dizziness intensity, pain intensity, and perceived disability—included the Visual Analog Scale (VAS) for assessing pain and disability, and the Dizziness Handicap Inventory for evaluating perceived disability. However, not all studies in this review assessed all four domains.
Dizziness intensity
This outcome measure was reported in six of the included studies. One study reported statistically significant differences between the intervention and control groups at 48 hours and one month after manual therapy treatment. Similarly, three studies conducted by the same authors observed positive outcomes when comparing pre- intervention data to results at 6 and 12 weeks following SNAGs treatment. The same research team examined Maitland mobilization as an alternative approach, finding clinically significant improvements that were sustained through 12 weeks of follow-up. Another research group reported comparable findings at 10 weeks post-treatment and at a one-year follow-up.
Cervical ROM
This variable was assessed in all eight, with statistically significant results favoring manual therapy interventions over the control groups. In one of the studies, two different intervention groups were compared—Mulligan’s SNAGs and Maitland mobilizations—with greater benefits observed in the SNAGs group.
Pain intensity
One study reported low pain intensity scores 48 hours post-treatment in the intervention group, with no significant effect observed in the control group. Similar findings were described by another group of researchers in their study.
Perceived disability degree
In all studies that measured this outcome, Dizziness Handicap Inventory (DHI) scores were significantly lower in the intervention group following manual therapy. Only one study reported similar scores between the intervention and control groups at the 10- week follow-up.
คำถามและความคิด
This systematic review, while valuable, has inherent limitations that temper the strength of its conclusions. The included studies exhibited significant heterogeneity across multiple domains, making it difficult to draw definitive clinical inferences. Most notably, the studied populations varied considerably in age (with mean ages ranging from 43 to 62 years) while providing limited additional demographic or clinical characteristics. This population diversity likely introduced substantial clinical heterogeneity that current analyses cannot fully account for.
The interventions themselves presented another layer of complexity, with studies employing markedly different manual therapy approaches including traction/distraction techniques, Maitland mobilizations, and SNAGs. This technical variability reflects different treatment objectives, further increasing study heterogeneity. Such diversity in therapeutic approaches makes it challenging to identify which specific techniques might be most effective or to generalize the findings across clinical practice settings.
Methodological quality emerged as another significant concern. Six of the eight included studies demonstrated high risk of bias, primarily due to deviations from intended interventions, while the remaining two raised some concerns in this domain. This creates significant uncertainty regarding the specific interventions participants received during these trials. Particularly concerning is our inability to determine whether interventions like patient education or psychosocial support – known factors in dizziness management – were differentially administered across groups.
Despite these limitations, the review identifies a consistent trend suggesting manual therapy for cervicogenic dizziness superiority over no treatment or sham interventions for cervicogenic dizziness. However, the current evidence cannot establish the magnitude of this benefit (as effect sizes were unreported), identify which patients respond best, or determine optimal treatment parameters. While benefits appear consistent across age groups, as reported by this systematic review, we lack precision about which techniques work best for specific clinical presentations.
These limitations highlight critical needs for future research, including standardized reporting of effect sizes, rigorous control of co-interventions, and investigation of patient-specific factors influencing outcomes. The following section will examine methodological approaches that could help overcome these limitations—both to deepen our understanding of manual therapy’s effects and to equip physiotherapists with critical appraisal tools for evaluating statistical concepts (e.g., effect sizes, heterogeneity) in future research.
พูดจาเนิร์ดกับฉันสิ
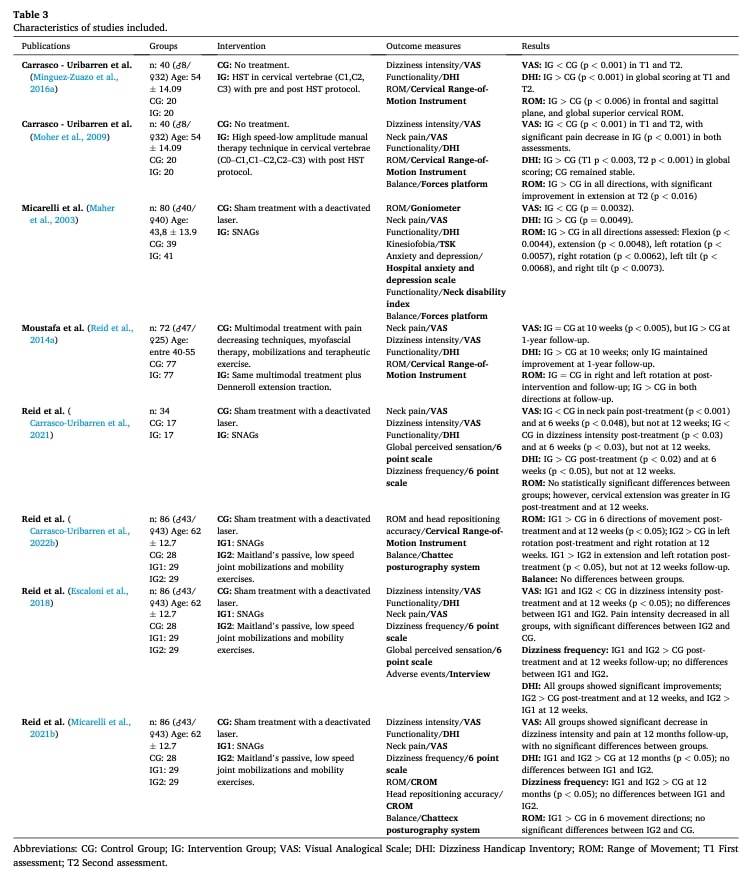
The methodological limitations identified in our previous discussion highlight several opportunities where stronger statistical approaches could have significantly strengthened this systematic review’s findings. While the study extracted basic parameters including patient age, group allocation, therapeutic interventions, and outcome measures (as shown in Table 3), it lacked critical methodological transparency. Most notably, the absence of a sufficiently documented data extraction protocol (including which patient characteristics beyond age were collected) obscures what population data the researchers extracted. Furthermore, the reporting of results focused solely on p-values while omitting crucial effect size metrics that are essential for clinical interpretation.
The substantial heterogeneity observed across studies, stemming from varying populations and intervention approaches, presented an important opportunity for deeper analysis. Formal quantification of this variability through I2 statistics would have provided valuable insight into the consistency of treatment effects. Additionally, planned subgroup analyses examining factors like technique type or age ranges could have helped identify potential moderators influencing outcomes. Such approaches would have clarified whether manual therapy’s benefits remain consistent across different clinical scenarios or are specific to contexts.
Perhaps most critically for clinical application, the review missed opportunities to quantify treatment effects in meaningful ways. Reporting standardized mean differences (SMD) or Cohen’s d values would have allowed physiotherapists to better understand the actual magnitude of expected treatment benefits. These effect size measures are particularly valuable as they help clinicians translate research findings into treatment expectations for their patients. While the review successfully identified statistically significant outcomes through p-values, the lack of these complementary metrics limits our ability to assess the clinical significance of manual therapy for cervicogenic dizziness.
ข้อความนำกลับบ้าน
Current evidence suggests manual therapy may help reduce pain, dizziness, improve function (ROM) and perceived disability degree in cervicogenic dizziness, but the strength of this conclusion is limited. While multiple studies show statistically significant benefits of manual therapy for cervicogenic dizziness, high variability in treatment techniques and patient populations makes it unclear:
- Which specific techniques work best
- How large the treatment effects truly are
- Which patients are most likely to respond
Until higher-quality studies with standardized methods and reporting (especially effect sizes) are available, clinicians should:
- Consider manual therapy as a potential option for cervicogenic dizziness
- Combine it with exercise and education (best current evidence supportsmultimodal care)
- Monitor individual patient responses closely
- Stay critical of claims about superiority of any one technique
Want to master cervicogenic dizziness management? This Physiotutors guide delivers evidence-based diagnosis and treatment strategies you can apply today.
อ้างอิง
5 เทคนิคการเคลื่อนไหว/การจัดการที่จำเป็นที่นักกายภาพบำบัดทุกคนควรเชี่ยวชาญ
เรียนรู้ เทคนิคการเคลื่อนไหว/การจัดการที่สำคัญ 5 ประการ ใน 5 วันที่จะทำให้ทักษะการบำบัดด้วยมือของคุณดีขึ้นทันที - ฟรี 100%!