
Research
Exercise
September 22, 2025
Превенција повреда при трчању: Како оптерећење тренинга и скокови током једне сесије утичу на ризик од повреда

Увод
Running remains one of the most accessible and widely practiced forms of physical activity worldwide. Despite advances in monitoring technology, including the widespread use of GPS wearables to track training load, the incidence of running-related injuries has not declined. Injury continues to be the primary factor leading individuals to discontinue running, underlining the importance of understanding the mechanisms underlying these conditions.
Traditionally, training load has been assessed within a weekly framework, most commonly using the Acute:Chronic Workload Ratio (ACWR), which is calculated by comparing the training load from the most recent week with the average weekly load from the preceding month. Traditional workload models may not capture the most effective running injury prevention strategies assuming that excessive increases in load across one week predispose athletes to overuse injuries. However, emerging evidence suggests that the period of vulnerability in running may be considerably shorter. Specifically, abrupt increases in running distance within a single session appear to play a critical role in injury development.
This explorative study introduces a potential paradigm shift: moving from a weekly to a single-session model for understanding training load and injury risk in runners. Such a framework may provide physiotherapists with more precise tools for running injury prevention guiding load management and rehabilitation in clinical practice.
Methods
This longitudinal exploratory study used data from the Garmin-RUNSAFE Running Health study with an 18-month follow-up period (July 2019 to January 2021). Enrollment took place between July and December 2019. The study was reported in accordance with the STROBE guidelines for observational studies, and the statistical analysis, interpretation, and reporting were verified using the CHAMP checklist.
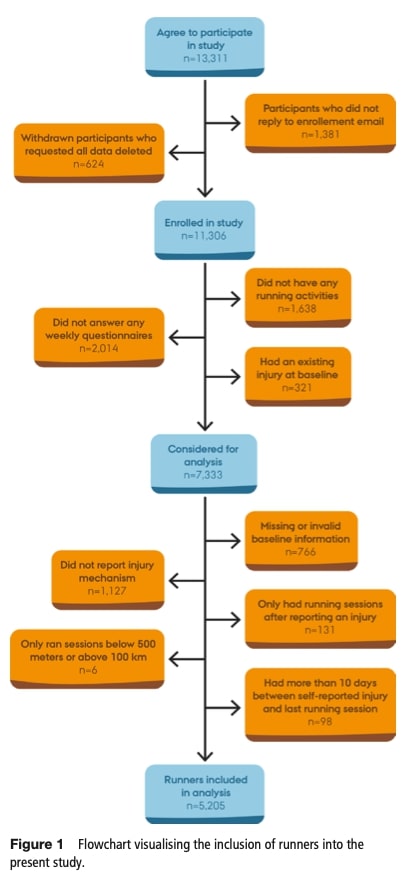
Runners were recruited through Garmin newsletters, European running clubs, and magazines. Those who consented and completed enrollment questionnaires were considered for inclusion.
Inclusion criteria:
- Use of a Garmin GPS device with data uploaded via the Garmin Connect app.
- Willingness to complete weekly questionnaires on injury status and anatomical location.
Exclusion criteria:
- Presence of a musculoskeletal problem at baseline.
- Failure to complete baseline or weekly questionnaires.
- No recorded running activity.
- Reporting an injury during follow-up without specifying whether it was traumatic or repetitive in origin.
- More than 10 days between a self-reported injury and the last recorded running session.
- Only performing running sessions below or above the predefined distances (inferior to 500m or superior to 100km).
Procedure
Baseline questionnaires collected demographic data (age, sex, height, weight), running experience, and history of previous injuries. Weekly questionnaires captured injury status and anatomical location of problems. Running activity data, including distance per session, was automatically recorded using Garmin GPS-enabled devices and transferred via the Garmin Connect app. Through an API-based system (Health API), these data were securely transmitted to Aarhus University servers and the RUNSAFE research group.
Exposure
The study measured exposure primarily as the ratio between the distance of a given running session and the longest session completed in the preceding 30 days. This ratio reflected how much a runner exceeded or fell short of their previous maximum. For example, running 12 km after a prior maximum of 8 km equalled a ratio of 1.5 (a 50% increase).
To better capture injury risk, relative changes were classified as follows:
- Regression or ≤10% increase (reference)
- Small spike (>10–30% increase)
- Moderate spike (>30–100% increase
- Large spike (>100% increase, i.e., doubling distance)
- Not possible (NP) – if no prior reference session existed
In addition to single-session changes, traditional workload measures were also calculated:
- Acute:Chronic Workload Ratio (ACWR): 1-week total distance ÷ average of prior 3 weeks.
- Week-to-week ratio: 1-week total distance ÷ previous week’s total distance.
The same cut-offs (10%, 30%, 100%) were applied for categorizing spikes in both models.
The primary outcome was the first self-reported overuse running-related injury. Traumatic injuries (e.g., from falls or twists) were treated as competing risks.
Outcomes
Injury status was assessed weekly via automated questionnaires. Runners classified themselves as:
- Injury-free
- Uninjured but with problems (pain/irritation without reducing running)
- Injured (pain/irritation with reduced running volume, intensity, or frequency)
For analysis, only runners who classified themselves as injured (category 3) were considered as having reached the outcome. Each participant was further asked to specify whether the injury was due to overuse (non-traumatic) or traumatic causes. When an injury was not reported on the exact day of a running session, it was instead linked to the most recent session completed within the previous 10 days, while any injuries reported more than 10 days after the last session were excluded. This definition of outcome was consistent with the Running Injury Consensus Statement and the Oslo Trauma Research Center questionnaire.
Confounding variables
The study addressed potential confounding using a directed acyclic graph (DAG) to visualize causal assumptions. The confounders included were previous running-related problems, body mass index (BMI), sex, age, and years of running experience. Previous problems were considered because they are a well-established risk factor for future injury and may influence running distance. Sex differences have been linked to variations in injury risk, intensity, and duration of running. A higher BMI increases mechanical stress on musculoskeletal structures and has consistently been associated with elevated injury risk. Age and running experience were also included, given their established associations with injury development. The large number of injuries in the dataset ensured sufficient statistical power to account for these variables.
Statistical analyses will be further discussed in the Talk nerdy to me section.
Резултати
The study included 5205 runners, most of whom were from Europe and North America. The majority were men (77.9%), with an average age of 45.8 years and a mean BMI of 24.2 kg/m². On average, participants had nearly a decade of running experience and were followed for a median of 80 running sessions, accounting for more than half a million sessions in total.
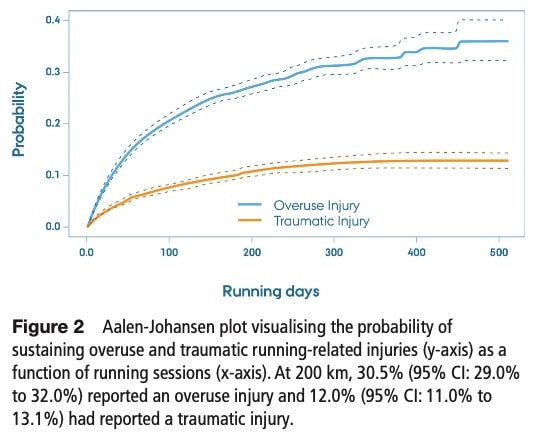
During the observation period, 35% of the runners reported a running-related injury. Among these, 72% were classified as overuse injuries and 28% as traumatic injuries. Injuries were typically reported either on the same day as the run or within one to two days afterwards. After 200 sessions, about 30.5% of runners had experienced an overuse injury and 12% a traumatic injury.
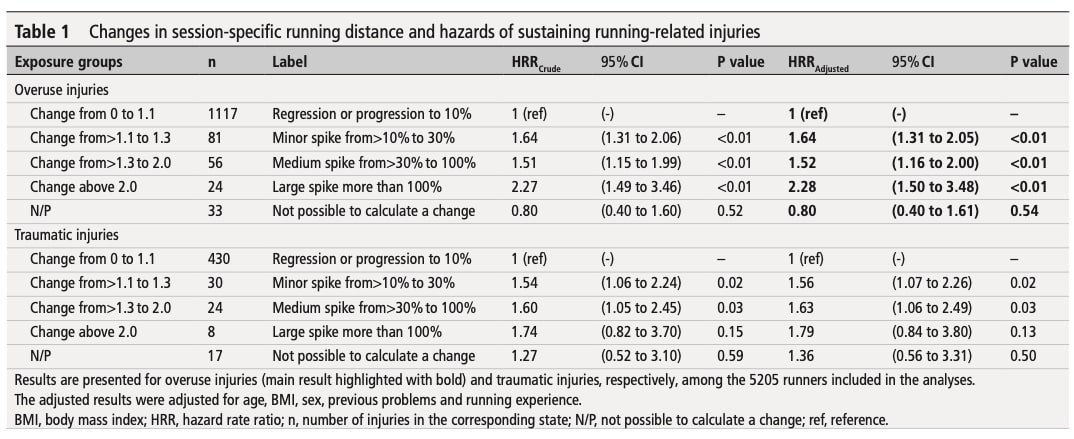
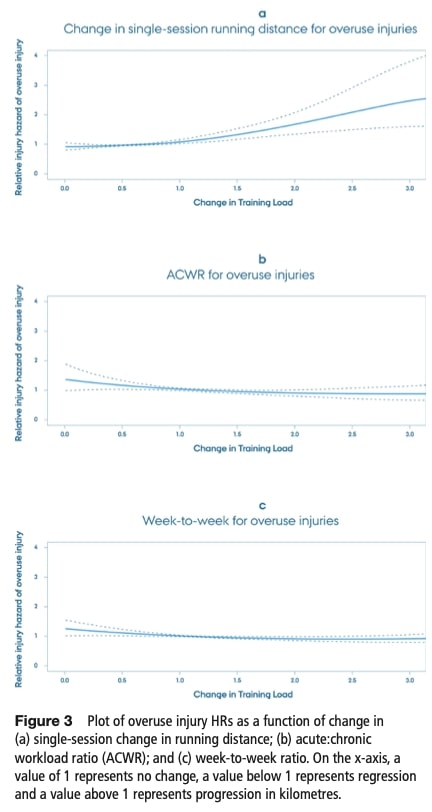
The main finding of the analysis was that sudden increases in the distance covered during a single running session were clearly linked to a higher risk of overuse injuries. When compared with gradual progressions of 10% or less, the risk rose substantially depending on the size of the spike:
- Small spike: risk increased by 64% (HRR = 1.64)
- Moderate spike: risk increased by 52% (HRR = 1.52)
- Large spike: risk more than doubled (HRR = 2.28)
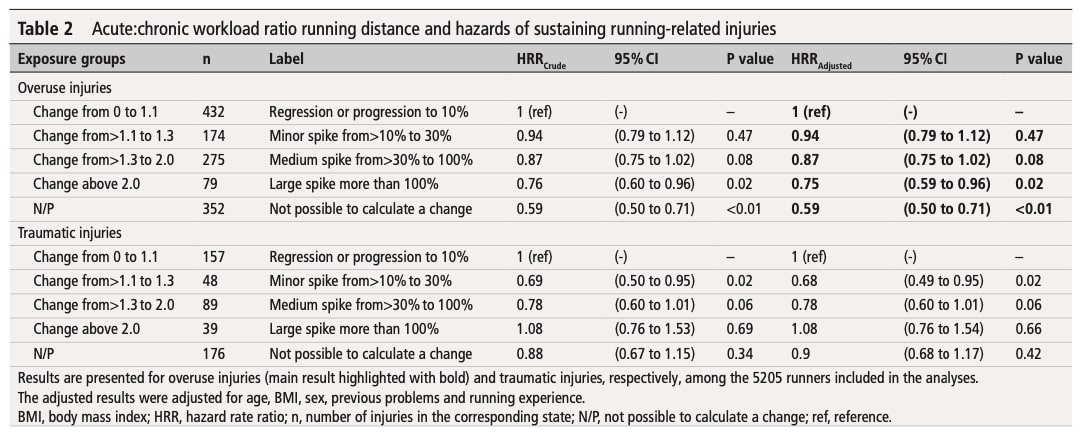
In contrast, when weekly training volume was assessed using the acute:chronic workload ratio (ACWR), spikes in running load appeared protective, being associated with a lower risk of injury. However, when week-to-week change was used as the metric, no significant association with injury risk was found.
Consequently, sensitivity analyses using alternative outcome definitions and cut-offs confirmed that increases in single-session running distance consistently elevated the risk of running-related injuries. Even relatively small increases, from 1% to 10% above previous distances, were associated with higher injury rates.
Питања и размишљања
Interestingly, the link between workload spikes and injury risk does not follow a simple linear trend. Small spikes were associated with a 64% higher injury risk, moderate spikes with a 52% increase, and large spikes with a 128% increase. While this non-linear relationship remains open to debate—something addressed in the following paragraph—the findings still highlight the value of a gradual approach to training progression. For example, after a 10 km run, increasing the next session by no more than 10% (about 1 km) is generally considered safe, whereas larger jumps significantly elevate injury risk. Since distance runners often vary their weekly training by mixing long, low-intensity sessions with shorter, high-intensity workouts (such as intervals), monitoring changes on a session-to-session basis may not be meaningful. In this context, the acute:chronic workload ratio (ACWR) could provide a more appropriate measure for running injury prevention.
Physiotherapists should recognize that training distance is only one of many factors influencing running injury prevention. While the study accounted for variables such as BMI and sex (with BMI remaining particularly debated in its relationship to injury), other potential confounders—most notably biomechanical factors—were not included. This is important because one review found no consistent biomechanical risk factors, likely due to heterogeneous study quality and nonspecific injury definitions, whereas another review identified injury-specific biomechanical associations in long-distance runners. Finally, this article review offers practical insights on biomechanical risk factors relevant to preventing running-related injuries.
It could be expected that the relationship between running distance and injury risk would follow a linear pattern, with greater increases in distance leading to proportionally higher injury risk. However, this was not clearly observed in the present study, likely because not all relevant injury-related factors were controlled. In particular, external load variables were not fully considered: elevation changes, running surface, uphill or downhill exposure, cadence, stride length, and footwear could all have influenced the outcomes. For a broader overview of how running injury risks can be assessed, see this study review
Finally, some methodological limitations should be considered. Participants were recruited through the Garmin Newsletter, a subgroup of runners who may not reflect the general running population, as they are likely more informed about training load, running injury prevention, and performance optimization. Furthermore, the categorization of symptoms—for example, the label “uninjured yet with problems”—may have been confusing and could have introduced bias.
Talk nerdy to me
Since this was an exploratory study, the authors did not calculate a required sample size or statistical power beforehand. Changes in running distance were expressed as ratios (based on kilometers run), but the analysis used running sessions as the time unit.
To model the relationship between training load and injury, they applied a multistate Cox regression model. In this framework, runners could move between the five “exposure states” (as defined in the exposure section), until they experienced an injury. Once an injury occurred—whether the main injury of interest or another competing injury—the runner entered a final state from which they could not return, and their follow-up ended there.
They tested whether the model’s assumptions (proportional hazard rates) held true using statistical diagnostics (log-log plots and the Grambsch and Therneau test). To improve model stability, extreme data points (sessions with implausible distance changes, e.g., >900%) were excluded.
Because no power calculation was done and extreme data were excluded, the results should be interpreted as exploratory and hypothesis-generating rather than definitive. The multistate Cox model is a robust method for time-to-event analysis with competing risks, but the absence of full control for all confounders and the exploratory design limit the strength of the causal inferences that can be drawn.
Поруке за понети кући
- Single-session spikes matter more than weekly load: This exploratory study suggests rethinking running injury prevention strategies by focusing on per-session spikes rather than weekly totals. Abrupt increases in running distance during a single session are strongly linked to a higher risk of overuse injury.
- Weekly workload ratios may be misleading: Traditional measures like the Acute:Chronic Workload Ratio (ACWR) did not reliably predict injury risk in this study. This suggests that focusing only on weekly totals may overlook the more immediate risks tied to “too much, too soon” in a single run.
- Gradual progression is safest: When preparing clients for distance goals (e.g., 10 km, half-marathon), advise them to increase per-session mileage by ~1 km at a time, rather than making large jumps. This conservative approach better aligns with running injury prevention evidence.
- Individual risk factors still matter: Factors such as previous injuries, BMI, age, and sex all influence injury risk. While training load is important, physiotherapists should adopt a holistic assessment that includes these personal characteristics.
- Biomechanical and external load variables remain understudied: Running surface, uphill/downhill exposure, footwear, cadence, and stride length were not addressed in this study but may contribute significantly to injury risk. Clinicians should continue to monitor and adjust these factors in practice.
- Educate patients about injury timing: Many overuse injuries appeared within 1–2 days of the “spike run.” Guiding runners to track not only how far they run but also how their body feels in the days after is a practical prevention tool.
- Use findings as guidance, not strict rules: Because this was an exploratory study, the results are hypothesis-generating. Physiotherapists should combine these insights with clinical expertise and patient context rather than applying them as rigid thresholds.
This Physiotutors clinical course will help you enhance your skills in running rehabilitation and optimize patient outcomes.
Референце
НАВЕДИТЕ СВОЈУ ДИФЕРЕНЦИЈАЛНУ ДИЈАГНОСТИКУ У БОЛУ КУКА КОЈИ СЕ ОДНОСИ СА ТРЧАЊЕМ - БЕСПЛАТНО!
Немојте ризиковати да пропустите потенцијалне црвене заставице или да завршите са лечењем тркача на основу погрешне дијагнозе ! Овај вебинар ће вас спречити да почините исте грешке на које многи терапеути постају жртве!
