
Research
Education & Career
April 17, 2025
Оштећење моторике и неупотреба: Кључни предиктори васкуларних компликација након можданог удара.

Увод
Stroke leads to significant declines in cardiorespiratory fitness, reducing functional capacity. Post-stroke, patients spend 78% of their waking hours in sedentary behaviors— far exceeding recommended physical activity levels—which heightens risks for cardiovascular and metabolic diseases. Compounding this issue, emerging evidence reveals maladaptive vascular changes post stroke, including impaired perfusion in the paretic limb due to vascular remodeling.
Current physical therapy interventions in acute settings prioritize neuroplasticity, which is essential for motor recovery. However, targeting cardiorespiratory fitness is equally critical to enhance patients’ ability to engage in daily activities and mitigate long-term vascular complications.
This study aims to investigate vascular changes post stroke by comparing arterial and intramuscular blood flow between the paretic and non-paretic upper limbs. Additionally, we will examine the relationship between these vascular parameters and clinical assessments of stroke-related impairment.
Method
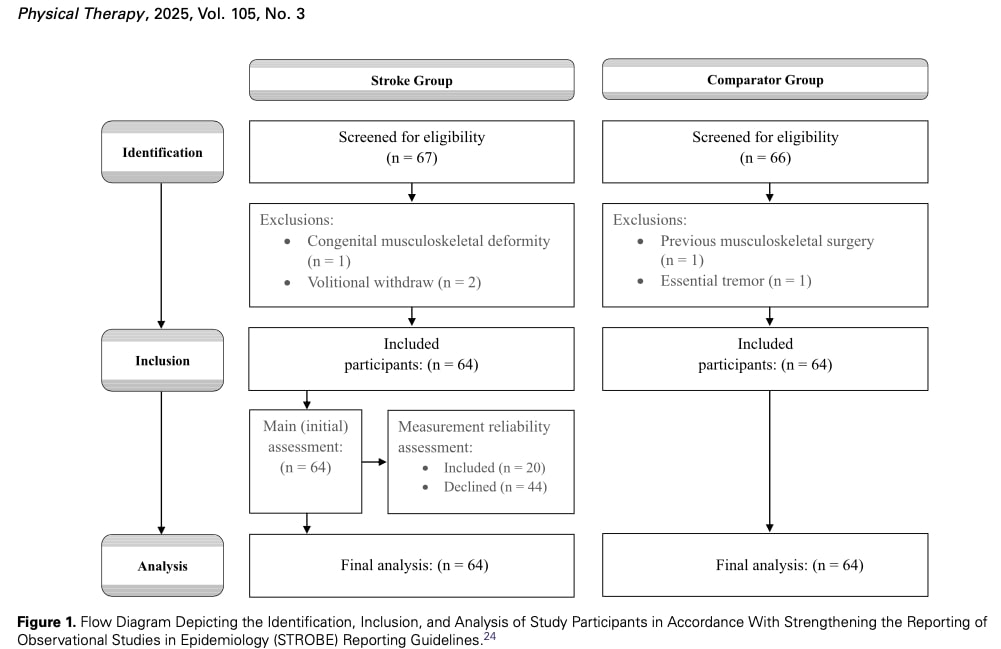
The study included 64 chronic stroke patients (>6 months post-stroke) and 64 matched controls. Participants were community-dwelling adults (≥18 years) with sufficient elbow mobility (60° flexion) and cognition (Abbreviated Mental Test ≥6) for testing. Individuals with other neurological conditions, severe contractures limiting testing, or serious contraindications for participation were excluded. Controls met identical criteria without stroke history.
The Fugl-Meyer Assessment (FMA) quantified upper limb motor impairment (scores 0- 66, higher=worse). Spasticity was measured using the Composite Spasticity Index (CSI; 0- 16), combining biceps tendon reflex (0-4), resistance to passive stretch (0-8), and wrist clonus (1-4), with scores 0-9=mild, 10-12=moderate, and 13-16=severe spasticity. The Motor Activity Log (MAL) assessed real-world arm use through Quality of Movement (MAL-QOM) and Amount of Use (MAL-AOU) subscales (lower scores=greater impairment).
Vascular assessments were conducted using an ultrasound system to evaluate bilateral biceps brachii intramuscular blood perfusion and brachial artery hemodynamics (diameter, flow volume). Imaging focused on the distal third of the biceps (66% of humeral length between coracoid process and cubital fossa) and medial brachial artery. Three measurement trials per parameter were averaged.
Blood flow volume (Vflow; mL/min) was measured using pulse-wave Doppler ultrasound at the previously described anatomical site. Arterial diameter (AD; cm) was determined from endothelial borders within the same image. To assess intramuscular blood perfusion, ultrasound imaging was used to calculate the vascularity index (VI), defined as the ratio of color pixels to total pixels within a specified region of interest.
Data analysis
Sample size was determined using G*Power (n=64/group) based on prior vascular studies (Cohen’s d=3.4 for between-group differences, r=0.35 for correlations). SPSS v28.0 analyzed data with Shapiro-Wilk/Levene tests for normality. Vascular parameters were compared using two-way repeated measures ANOVA (ηp2 effect sizes), with post- hoc t-tests (Bonferroni-corrected). Correlations (Pearson/Spearman) assessed relationships between vascular measures and clinical assessments (FMA, MAL, CSI). Hierarchical regression identified determinants of vascular asymmetry (%SSD), controlling for demographics and limb dominance (separate models for collinear variables). Effect sizes were reported as Cohen’s d (between-group) and correlation coefficients (non-parametric tests).
We will explore the analytical methods in greater depth in the “Talk nerdy to me” section.
Резултати
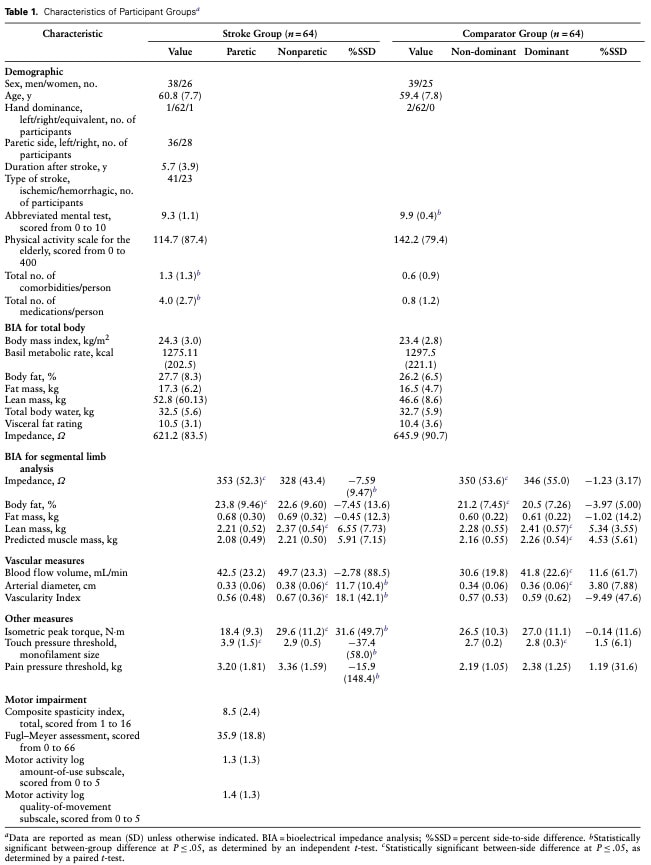
The study included 64 chronic stroke survivors (mean age 62.4 ± 10.1 years, 70% male) and age-/sex-matched controls. Participants were on average 5.7 ± 3.9 years post- stroke, with predominantly ischemic strokes (64%, n=41); 36% (n=23) had hemorrhagic strokes. They presented with moderate motor impairment (FMA-UE: 35.9 ± 18.8), mild spasticity (CSI: 8.5 ± 2.4), and minimal functional arm use (MAL-AOU: 1.3 ± 1.3). Basic cognition was preserved (Abbreviated Mental Test ≥6). Controls showed significantly fewer comorbidities and medications (P≤.05). Limb dominance (28 dominant-side affected vs. 36 nondominant) did not influence impairment severity. See Table 1 for full demographics.
Vascular ultrasound measures:
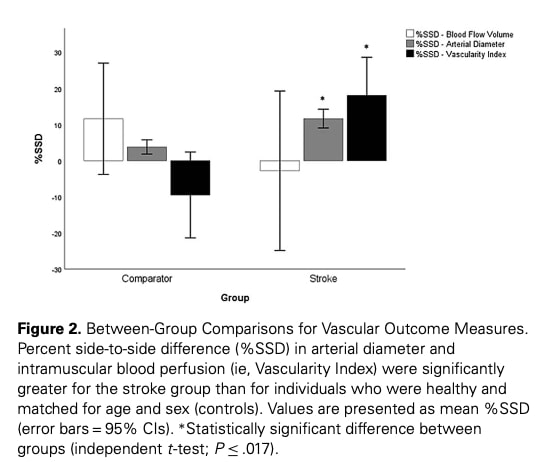
The analysis revealed significant differences in vascular measures between stroke survivors and controls. Notably, the paretic limbs of stroke participants showed reduced arterial diameter (AD) and vascularity index (VI) compared to their nonparetic sides, while controls exhibited expected dominance (handedness)-related variations in blood flow. Stroke survivors demonstrated greater asymmetry in AD and VI between limbs than controls. When examining limb dominance subgroups, both groups (dominant- affected and nondominant-affected) showed reduced AD in paretic limbs, while other differences varied by subgroup—particularly in blood flow asymmetry, which was more pronounced when the dominant side was affected. These results highlight distinct vascular alterations in paretic limbs that persist regardless of dominance.
The study found stroke survivors showed significant asymmetry between limbs, with paretic sides demonstrating weaker strength, higher sensory thresholds, and altered body composition (reduced lean mass, increased fat) compared to non-paretic limbs. These differences exceeded normal dominance-related variations seen in controls. Notably, strokes affecting the non-dominant limb resulted in more pronounced body composition changes than dominant-side strokes. The findings reveal that post-stroke limb changes extend beyond motor impairment to include substantial sensory and structural alterations that differ from natural inter-limb variations.
The study found consistent but modest associations between vascular asymmetries (%SSD) and clinical measures in stroke survivors. Vascular parameters (Vflow, AD, VI) showed weak correlations with motor impairment (FMA) and functional arm use (MAL), suggesting that while vascular changes relate to clinical deficits, other factors likely contribute to these impairments. Similarly, correlations between vascular asymmetries and tissue composition measures ranged from weak to moderate indicating some linkage between blood flow alterations and structural limb changes. These findings collectively suggest that post-stroke vascular changes represent an important, but not exclusive, contributor to overall limb impairment, warranting consideration alongside other physiological and functional measures in clinical assessment and rehabilitation planning.
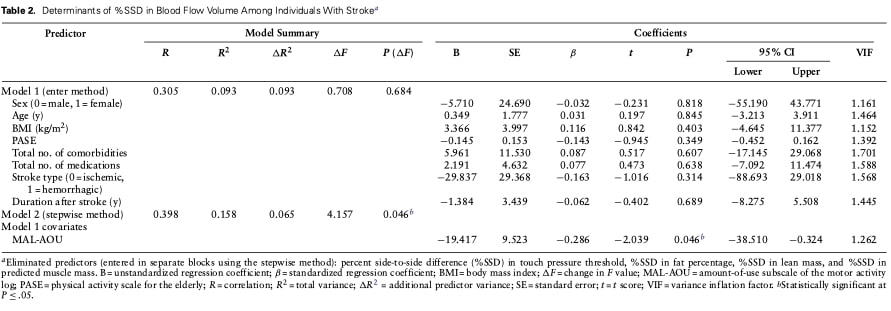
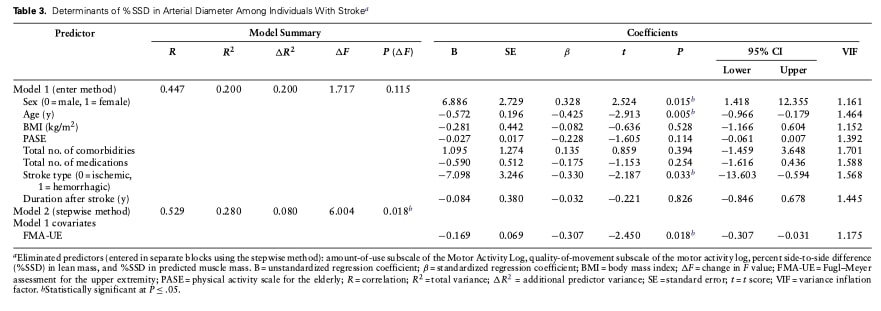
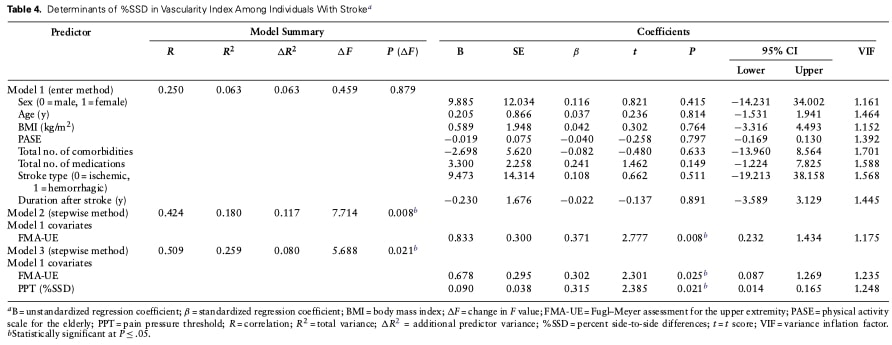
The regression analyses revealed key predictors of vascular asymmetry (%SSD) after controlling for demographic and clinical factors. Reduced paretic arm use (MAL- AOU) predicted blood flow asymmetry but became non-significant after accounting for limb dominance. Motor impairment (FMA) independently predicted arterial diameter asymmetry, explaining 8% of variance. For vascularity index, both motor impairment and sensory changes (pain pressure threshold) were significant predictors, together accounting for nearly 20% of variance. These relationships persisted even after adjusting for limb dominance, highlighting the combined impact of motor and sensory deficits on post-stroke vascular changes.
Питања и размишљања
This study identifies significant vascular changes post stroke and their association with motor impairment in chronic stroke, though the modest correlation strength (ρ=0.25–0.35) suggests vascular factors only partially explain functional deficits. A critical unresolved question emerges: Are these vascular changes post stroke primarily caused by induced structural damage, chronic limb disuse, or both mechanisms?
While prior research confirms stroke-related vascular dysfunction (e.g., reduced arterial elasticity [1]), this study’s observational design cannot distinguish between:
- Structural mechanisms: Endothelial dysfunction or neurovascular remodeling post-stroke, versus
- Disuse mechanisms: Flow-mediated vascular atrophy from reduced paretic limb activity.
Notably, baseline differences in cognition, comorbidities, and medication use between groups (Table 1) may confound these associations, limiting causal interpretations.
Future directions should employ interventional designs to establish causality. Constraint- induced movement trials with pre/post vascular assessments could clarify whether forced paretic limb use reverses perfusion deficits—supporting a disuse mechanism—or if impairments persist, implicating irreversible structural damage. Such studies would inform whether vascular-targeted therapies (e.g., blood flow augmentation) should complement traditional motor rehabilitation.
Причај ми штреберски
The researchers began by testing key statistical assumptions to guide their analytic choices. Using the Shapiro-Wilk test, they evaluated whether continuous variables followed a normal distribution, which determined whether parametric tests (assuming normality) or non-parametric alternatives would be appropriate. Simultaneously, Levene’s test assessed homogeneity of variance across groups, ensuring comparable variability between stroke patients and controls. These preliminary checks were critical for validating subsequent analyses.
When examining relationships between variables, the team distinguished between different types of associations. A monotonic relationship—a consistently increasing or decreasing trend between two variables that isn’t necessarily linear—was assessed using Spearman’s ρ. This became particularly important when data violated normality assumptions or when analyzing ordinal measures. For normally distributed data showing linear patterns, Pearson’s r quantified the strength and direction of straightforward linear relationships.
The core analysis employed mixed-design ANOVA to evaluate complex group differences. This approach simultaneously assessed within-subject effects (comparing paretic versus nonparetic limbs in stroke patients), between-group effects (stroke versus control participants), and interaction effects (whether limb differences varied by group status). The ANOVA was complemented by effect size calculations (η2) to quantify the magnitude of observed differences.
Significant findings were further investigated through post-hoc tests:
- Paired t-tests identified specific within-group limb differences
- Independent t-tests compared the degree of asymmetry (%SSD) between stroke and control groups
- All post-hoc tests employed Bonferroni correction (adjusted α = 0.017) to limit the probability of false positives (family-wise error rate) to ≤0.05 across all comparisons.
Additional analyses included:
- Hierarchical regression to identify predictors of vascular asymmetry while controlling for covariates
- Subgroup analyses based on limb dominance
- Reliability testing (ICC) evaluated the consistency of repeated ultrasound
measurements for vascular parameters (Vflow, AD, VI)
The comprehensive approach ensured robust examination of both the magnitude and clinical relevance of observed effects while maintaining appropriate control for Type I error inflation.
Понесите поруке кући
Chronic stroke survivors show measurable vascular changes post stroke (reduced blood flow, arterial diameter, and tissue perfusion) in paretic limbs, which correlate—albeit modestly—with motor function. While these changes likely contribute to disability, their exact cause (stroke-induced vascular damage vs. disuse atrophy) remains unclear. Clinically, this underscores:
- The value of monitoring vascular health alongside motor recovery, and
- The potential for combined rehabilitation approaches targeting both mobility and perfusion (e.g., activity-based therapies to combat disuse). Future research should clarify whether vascular interventions could augment functional gains.
Assessment:
Vascular screening (e.g., ultrasound) may help identify patients at risk for poor recovery due to perfusion deficits. A multidisciplinary approach (e.g., integrating vascular and motor assessments) could clarify relationships between vascular changes and functional impairment.
Rehab Implications:
Intensive limb use (e.g., Constraint-Induced Movement Therapy/CIMT) may counteract disuse-related vascular changes post-stroke. Virtual reality could serve as a valuable clinical tool to address these adaptations.
Combined interventions targeting both perfusion (e.g., aerobic exercise) and motor function could synergistically improve metabolic and muscular adaptations in the paretic limb.
Caution: The modest correlations suggest vascular factors are part of a multifactorial impairment puzzle.
Референце
ИЗАЗОВ: РЕШИТЕ КВИТ КОЈИ 75% ФИЗИОТЕРАПУТА НЕ ПАЖЕ
Одговорите на ових 10 кратких питања о основном знању које сваки физиотерапеут треба да зна и сазнајте да ли имате бољи резултат
