
Research
Ankle/Foot
February 19, 2026
Identifying Lower Limb Arterial Disease: Clinical Takeaways and Tests That You May Have Overlooked in Your Clinical Practice

Увод
Peripheral arterial disease (PAD) is a common vascular condition with a prevalence estimated at approximately 7% among individuals aged 55 to 59 years, increasing progressively with age and reaching up to 25% in those aged 95 to 99 years. Despite its high prevalence, PAD remains under-recognized in musculoskeletal practice. Clinically, it may present with lower limb pain and functional limitations that can mimic neurological conditions such as lumbar radiculopathy, leading to potential misdiagnosis.
Given its frequency and the overlap of symptoms with neuromusculoskeletal disorders, PAD should be considered in patients who fail to respond to conventional physiotherapy interventions for presumed radicular or mechanical lower limb pain. Early identification of lower limb arterial disease is essential to ensure appropriate referral and management.
This narrative review aims to provide an overview of peripheral arterial disease relevant to physiotherapy practice and to outline key clinical screening tests for lower limb arterial insufficiency, thereby supporting more accurate differential diagnosis and optimizing patient care.
Методе
This narrative review was conducted by a panel of experts. However, the review does not report a detailed search strategy, including the databases consulted, search terms used, or inclusion and exclusion criteria applied. Furthermore, limited information is provided regarding the academic and professional backgrounds of the authors, making it difficult to assess the expertise informing the review process.
Резултати
Peripheral arterial disease
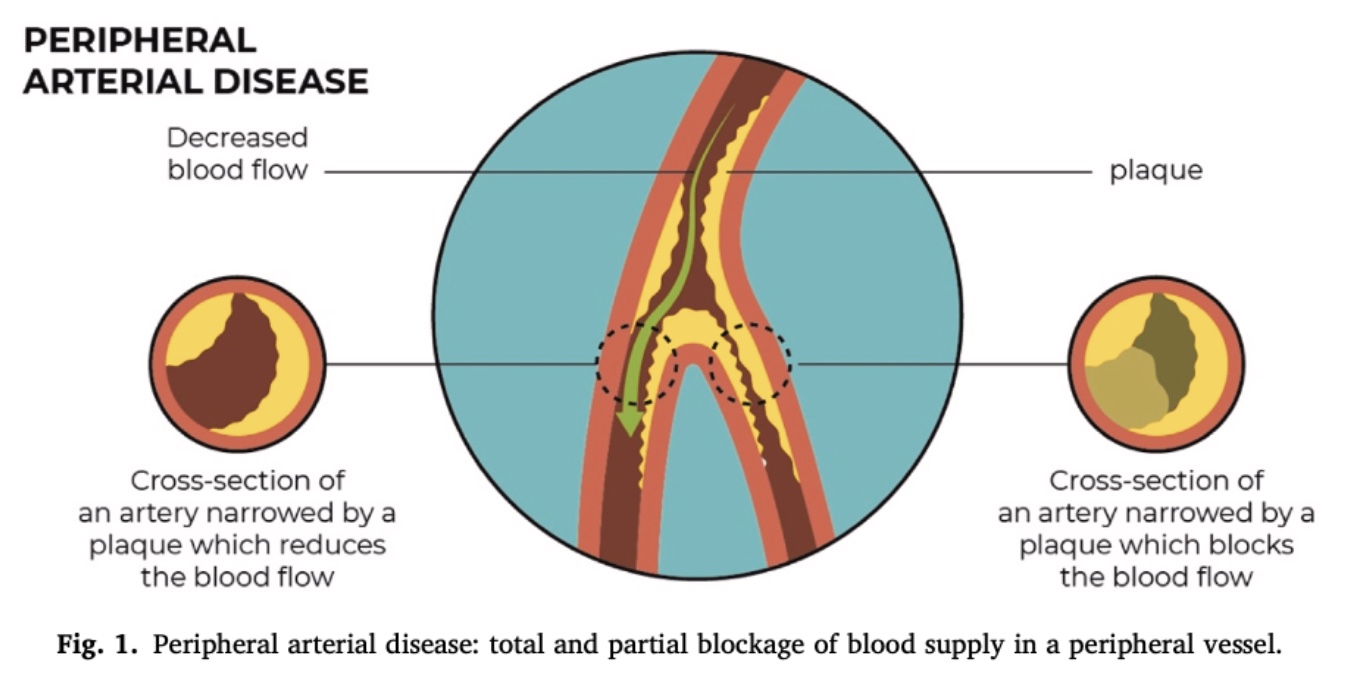
PAD is a vascular condition characterized by the narrowing or obstruction of arteries that supply blood from the heart to the peripheral tissues. Although PAD most commonly affects the lower limbs, the upper extremities may also be involved.
The condition is asymptomatic in approximately 20–50% of cases. Symptoms typically arise when arterial blood flow becomes insufficient to meet the metabolic demands of the tissues, particularly during physical activity. This mismatch may result in pain and functional limitation.
Patient interview
Suspicion of lower limb arterial disease often arises during the patient interview. Symptom onset is typically insidious and progressively worsening over time. PAD is a multifactorial condition and is frequently associated with at least one cardiovascular risk factor.
Patient’s Characteristic
Individuals aged over 65 years, as well as those aged 50–64 years with established cardiovascular risk factors (detailed below), are considered at increased risk for lower limb arterial disease. Epidemiological data also indicate a higher prevalence of PAD among males.
Medical history
A thorough medical history is essential. The clinician should screen for cardiovascular and metabolic risk factors known to be associated with PAD, including:
- Diabetes mellitus
- Tobacco use
- Hypertension
- Dyslipidemia
- Hyperhomocysteinemia
- Elevated C-reactive protein levels
- Chronic renal insufficiency
The presence of atherosclerotic disease in other vascular territories (e.g., coronary or carotid arteries) further increases the likelihood of PAD.
Symptoms presentation
PAD may present with three main clinical patterns: claudication, ischemia, and atypical pain.
Claudication
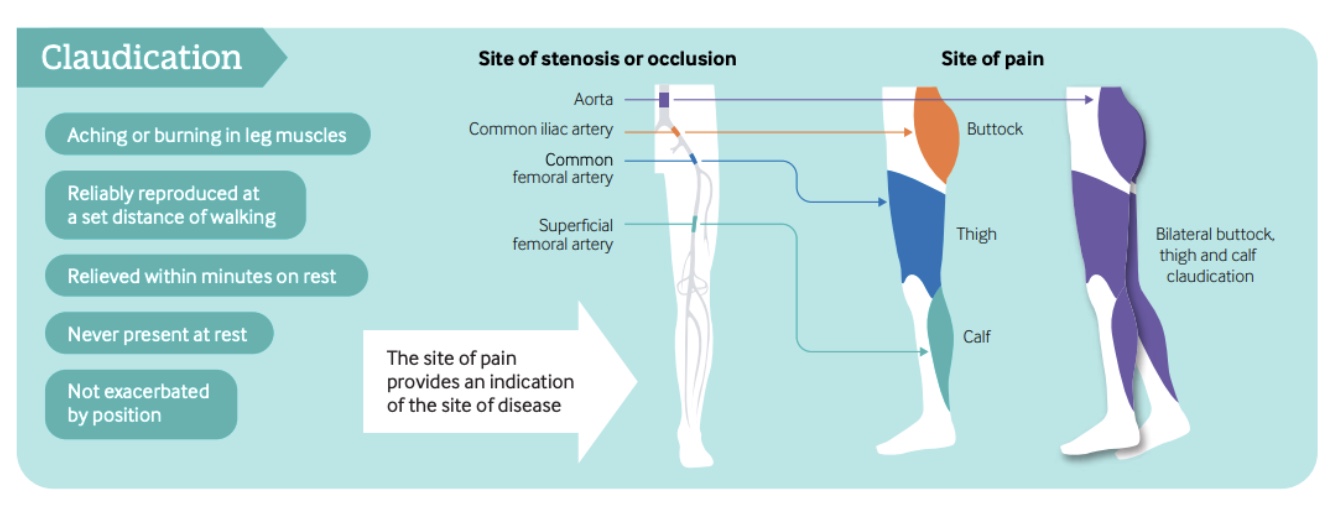
Intermittent claudication occurs in approximately 10–35% of symptomatic patients with peripheral arterial disease (PAD). It is characterized by exercise-induced pain, typically described as cramping, fatigue, or burning, that is relieved by rest.
Pain may be unilateral or bilateral and commonly affects the buttock, thigh, or calf. Symptom location often reflects the level of arterial occlusion: aortic involvement typically produces bilateral symptoms, whereas iliac or femoral artery disease more commonly causes unilateral pain localized to the buttock, thigh, or calf, respectively.
Ischemia
Pain is typically localized to the forefoot and may be present at rest, reflecting severe arterial insufficiency. Symptoms often worsen with lower limb elevation, which can complicate differentiation from neurological conditions.
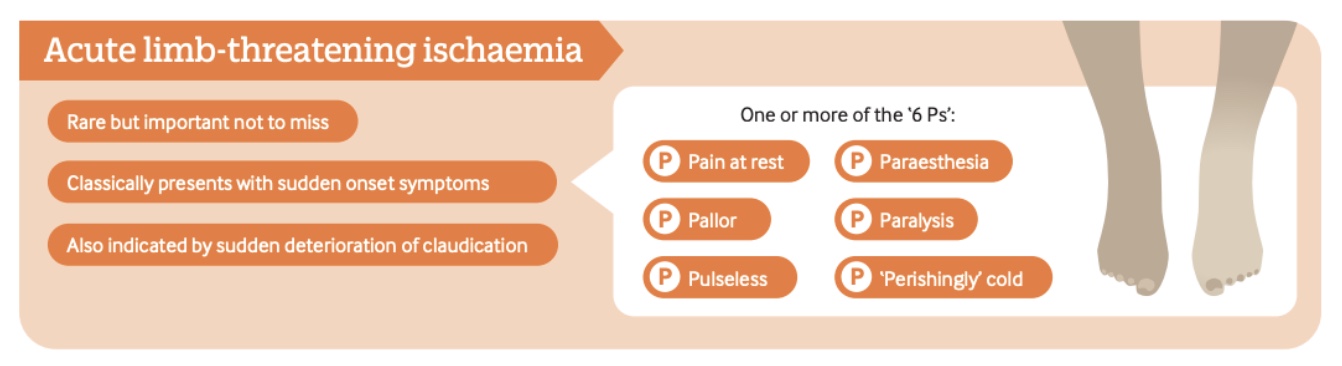
Clinical presentation may include the classic “six Ps”: pain, pallor, pulselessness, paresthesia, paralysis, and perishingly cold limb. This presentation constitutes a vascular emergency and may indicate impending limb loss if not promptly managed.
Atypical pain
Atypical presentations of lower limb arterial disease may involve unilateral or bilateral discomfort in the buttock, thigh, or calf. Symptoms are often described in vague terms, such as “calf discomfort” or a “burning sensation in the quadriceps,” rather than classic cramping pain. Patients commonly report reduced walking capacity.
Atypical PAD-related pain is less well characterized than intermittent claudication, making clinical identification more challenging. Further research is needed to better establish the relationship between atypical lower limb pain and underlying ischemic changes.
Physical examination
Lower limb vascular screening
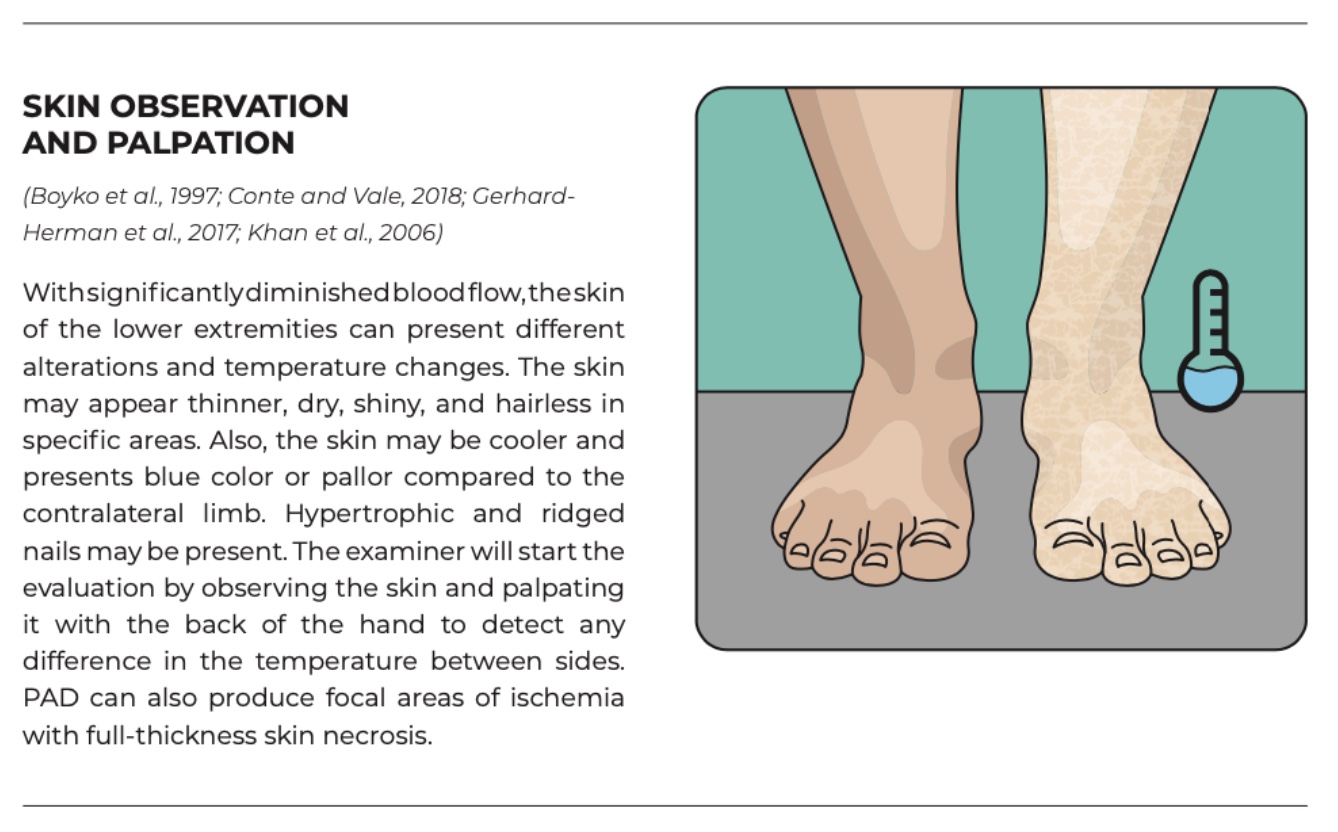
Capillary refill testing has limited diagnostic accuracy and should not be used in isolation. Initial assessment should include vital signs, with blood pressure measured in both arms and heart rate recorded. Pulse palpation is a key component of the vascular examination and is considered one of the most sensitive clinical signs of arterial insufficiency.
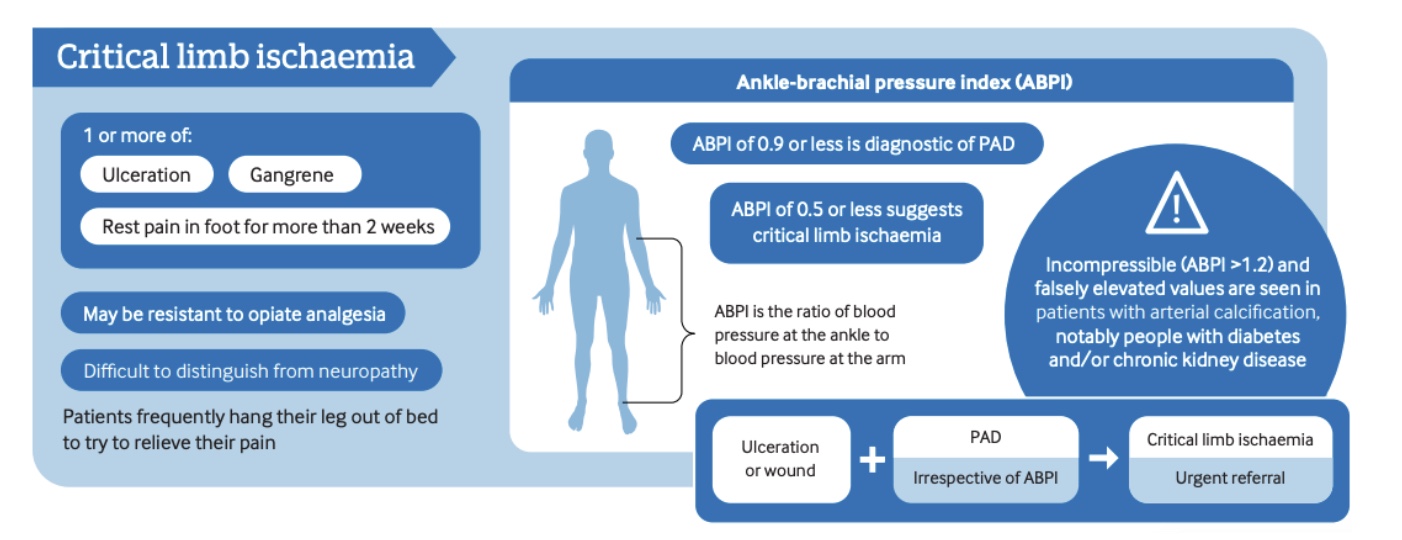
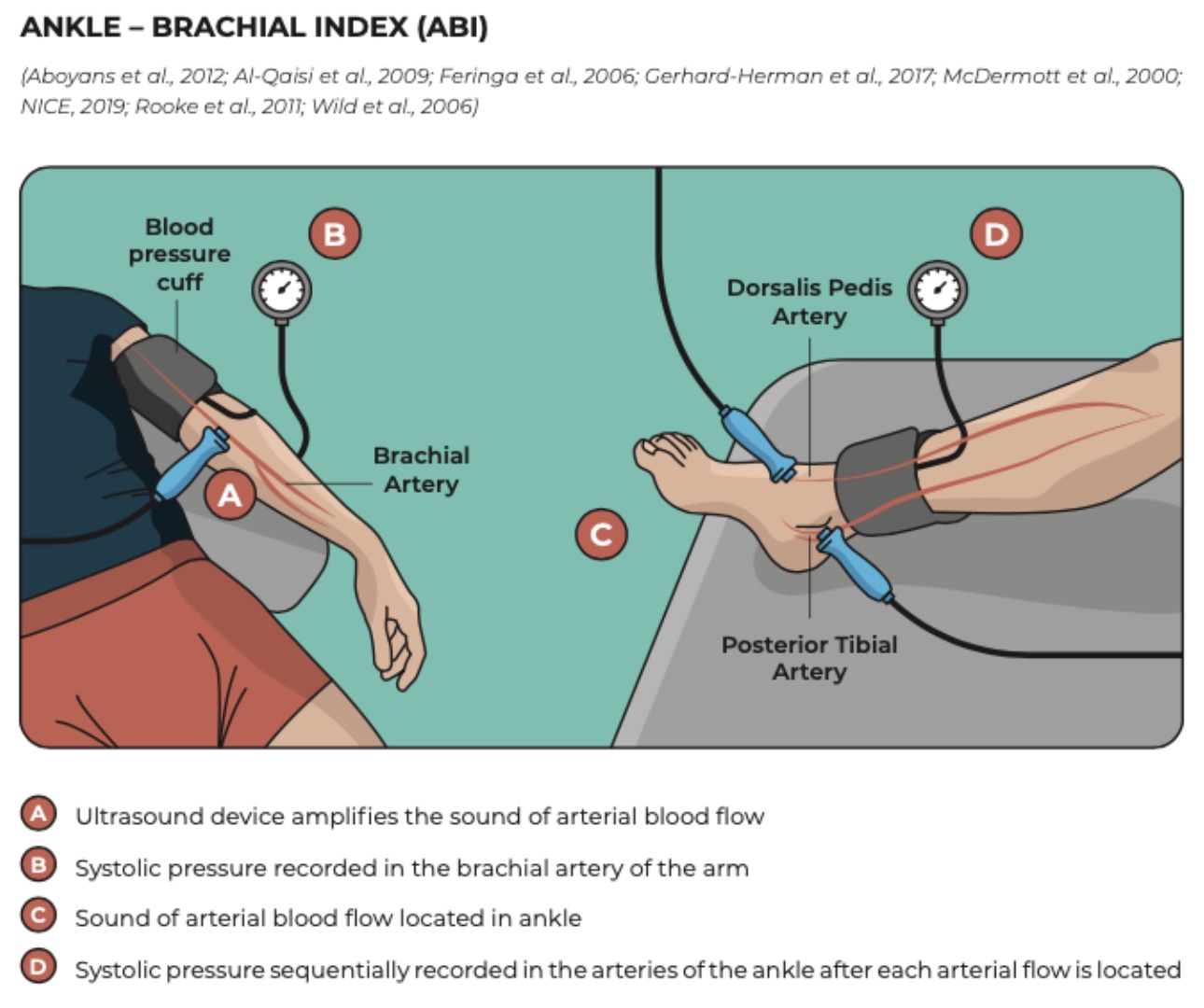
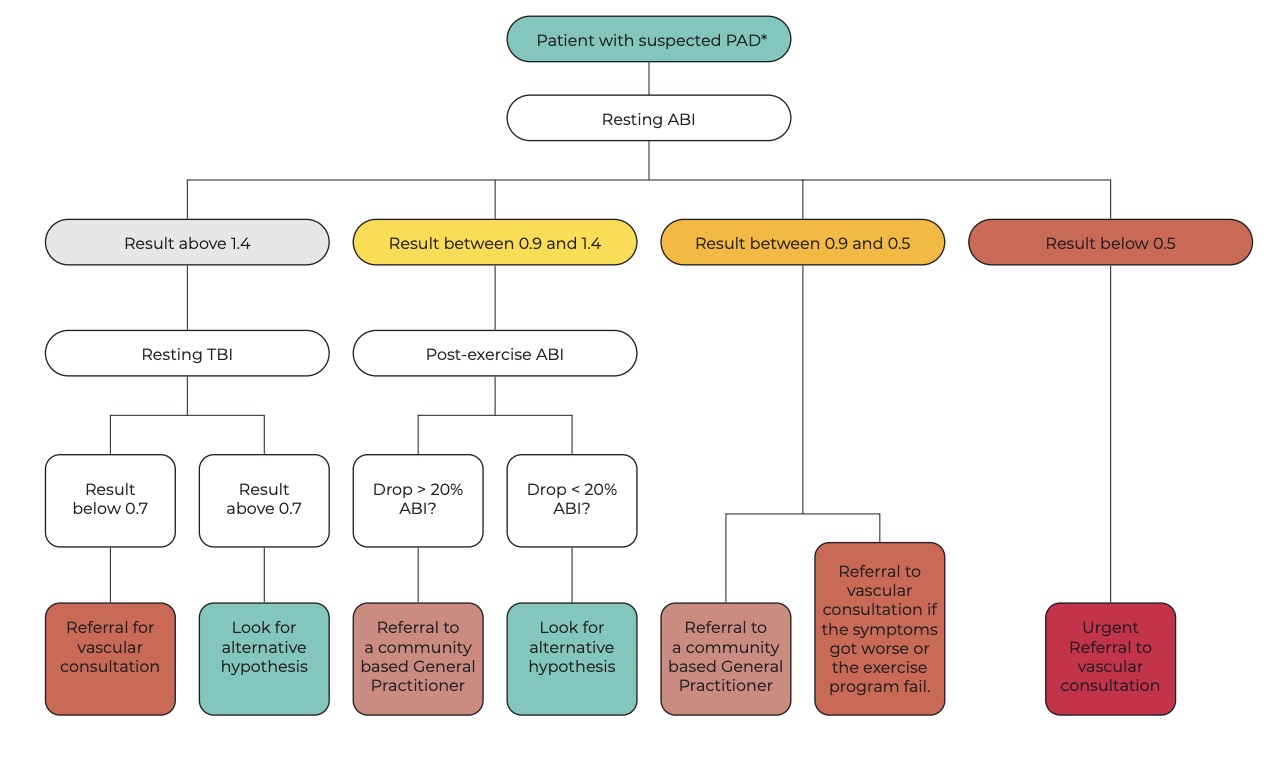
The Ankle–Brachial Index (ABI) should then be measured at rest. An ABI < 0.90 demonstrates high sensitivity and specificity for peripheral arterial disease (PAD). ABI values also provide information regarding disease severity: values between 0.5 and 0.9 are typically associated with claudication, 0.2 to 0.5 with rest pain, and 0.0 to 0.2 with tissue loss.
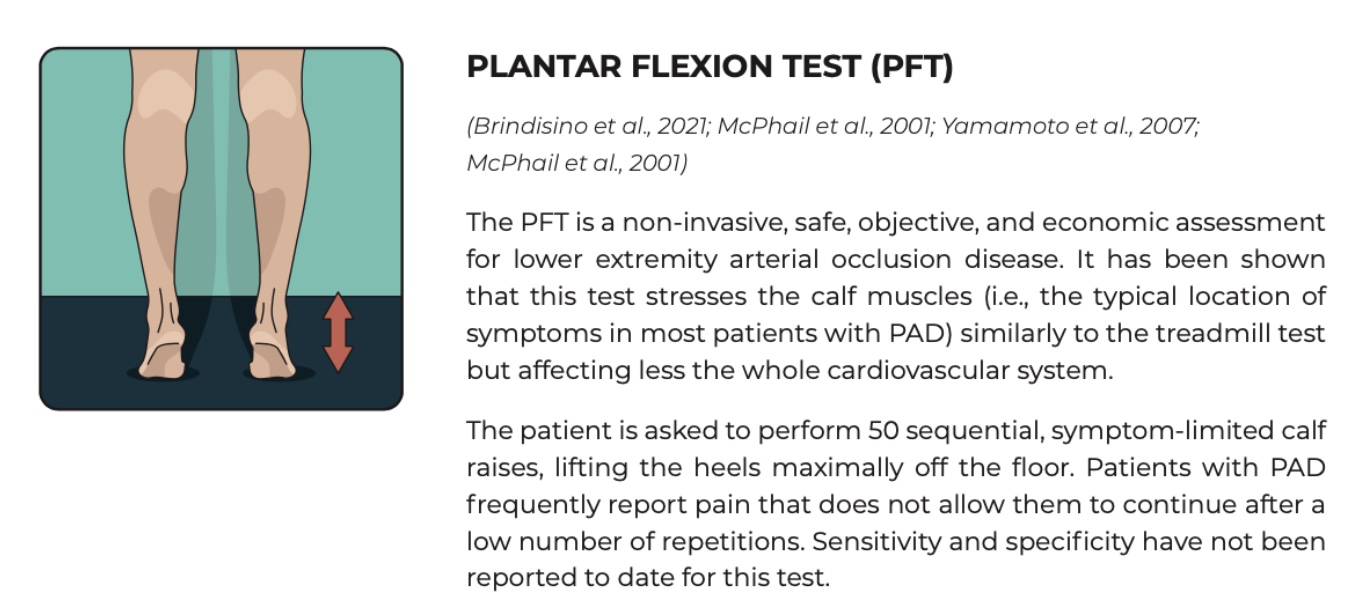
Because resting ABI may fail to detect PAD in some cases, exercise testing—such as a 5-minute treadmill walk or repeated heel raises—can improve diagnostic sensitivity by revealing a post-exercise drop in ABI values. The 6-minute walk test may additionally serve as a baseline measure of functional capacity and help identify the onset of exertional symptoms.
Clinical reasoning
Physiotherapists should recognize that patients’ presentations may result from mixed pathologies or comorbidities. While ABI measurement is not routinely performed in general physiotherapy practice, a thorough patient assessment can guide the clinician toward appropriate vascular and neurological tests.
For example, patients with diabetes and reduced lower limb sensation may benefit from a combination of ABI, monofilament, and nerve mechanosensitivity testing to identify coexisting peripheral arterial and neuropathic conditions. Clinical reasoning should always consider the possibility of overlapping presentations to ensure accurate diagnosis and appropriate management.
Management
Asymptomatic patients or those presenting with intermittent claudication should be referred to primary care for further evaluation. Cardiovascular risk factors—including smoking, hypertension, and weight management—should be addressed as part of comprehensive care.
Exercise therapy is a first-line treatment for PAD, with a focus on improving cardiorespiratory fitness. Walking is the most effective and accessible exercise modality, recommended at least three times per week for a minimum of 12 weeks. For patients who do not respond adequately to exercise, pharmacological options such as vasoactive agents may be considered.
Питања и размишљања
Physiotherapists are increasingly involved in the primary assessment and classification of patients, yet vascular testing—including the Ankle–Brachial Index (ABI)—remains underutilized in routine practice. Currently, there is limited data on the inter- and intra-rater reliability of these vascular assessment procedures among physiotherapists, highlighting a need for standardized training and evaluation.
Differentiating lower limb arterial disease from neurological conditions can be challenging, as ischemic symptoms are often exacerbated by lower limb elevation. Tests such as the straight-leg raise (SLR) with distal nerve maneuvers may help distinguish the two: symptom reproduction during SLR is more suggestive of nerve mechanosensitivity than vascular insufficiency. Additionally, vascular sclerosis can mimic PAD, and functional tests, such as cycling, may assist in differentiation.
While Doppler ultrasound is a valuable tool for ABI testing, it may not be readily available in all physiotherapy settings. More accessible alternatives, such as auscultation with a stethoscope, are feasible but require more extensive training to ensure accurate assessment.
Overall, while narrative reviews like this provide clinically relevant insights and practical tools, further research is needed to validate vascular testing protocols in physiotherapy, assess reliability, and improve confidence in the primary classification of patients with suspected PAD.
Причај ми штреберски
As with most narrative reviews, the study provides clinically relevant information and offers physiotherapists practical tools to support assessment and management of PAD. However, several methodological limitations must be considered.
Selection bias is a significant concern in this type of study design. The absence of a clearly described literature search strategy raises the possibility of cherry-picking, where studies supporting the authors’ perspectives may have been preferentially included. Consequently, the included studies may not fully represent the available evidence on the topic.
Information regarding the review process, including the roles and contributions of co-authors, is limited. Notably, one study is cited eleven times within the paper, which may suggest a narrow scope of literature screening and reliance on a small subset of available research.
Поруке за понети кући
Consider PAD in musculoskeletal practice: lower limb arterial disease is common, especially in older adults, but often under-recognized. Patients with lower limb pain not responding to standard physiotherapy interventions may have vascular involvement.
Screen high-risk patients: Individuals over 65, males, and those with cardiovascular risk factors (diabetes, smoking, hypertension, dyslipidemia, renal insufficiency, or atherosclerosis elsewhere) should be assessed for PAD.
Know the symptom patterns:
- Claudication: Exercise-induced calf, thigh, or buttock pain, relieved by rest.
- Critical ischemia: Forefoot pain at rest, worsened by limb elevation, with “six Ps” (pain, pallor, pulselessness, paresthesia, paralysis, perishingly cold) indicating vascular emergency.
- Atypical pain: Vague discomfort or burning sensations with reduced walking capacity; harder to identify clinically.
Perform a structured assessment:
- Measure vital signs (blood pressure in both arms, heart rate).
- Palpate pulses—this is a sensitive clinical indicator of PAD.
- Conduct Ankle–Brachial Index (ABI) testing: ABI < 0.90 suggests PAD; values also indicate severity (0.5–0.9: claudication, 0.2–0.5: rest pain, 0.0–0.2: tissue loss).
- Consider exercise ABI (treadmill or heel raises) if resting ABI is normal but symptoms persist.
Consider mixed presentations: Patients may present with coexisting lower limb arterial disease and neuropathic conditions.
Referral and management:
- Refer asymptomatic or claudicant patients to primary care for evaluation.
- Address modifiable cardiovascular risk factors.
- Prescribe supervised exercise therapy (walking, 3×/week for ≥12 weeks) as first-line treatment. Check out this Physiotutors video for intermittent claudication guidelines.
- Consider medical referral for patients who do not respond to exercise treatment.
Appendix
Appendix 1 is a free-access step-by-step guide for peripheral artery disease testing and is available here.
Референце
ОТКРИТЕ ФАСЦИА ОД ЊЕНЕ ИСТОРИЈЕ ДО ЊЕГОВИХ РАЗЛИЧИТИХ ФУНКЦИЈА
Уживајте у овој бесплатној 3к 10-минутној видео серији са реномираним анатомом Карлом Џејкобсом који ће вас одвести на путовање у свет Фасциа
