Research
EBP & Statistics
June 16, 2025
Lateral Epicondylalgia and Heavy Slow Resistance Training - How Not To Conduct Research

Увод
Heavy slow resistance (HSR) training has emerged as a treatment option for tendinopathies. While there is an abundance of trials examining the effectiveness of HSR training in the lower limb, evidence in the upper limb is scarce. Today, we will look at the findings from a pilot study about HSR training for lateral epicondylalgia. At first, I wanted to write something about this pilot study, to learn about the preliminary findings from this pilot study, and in which direction the evidence on HSR for lateral epicondylalgia may be heading. But when I read the article, several flaws and shortcomings emerged, and I came across another study also looking at the feasibility of HSR for the same condition. Therefore, I shifted my focus to present this research review as the first part of a two-part series. In this research review part 1, we will look into a pilot study examining the effectiveness of HSR for lateral epicondylalgia, or tennis elbow, as a starting point for evidence gathering about this training and rehabilitation method in the upper limb. But, based on the article, we’ll also discuss its methodological shortcomings and how to avoid common research pitfalls.
Методе
Today, we will discuss the pilot study of Divya Mary et al. (2025), which compares the effects of HSR training to conventional exercise in people who have unilateral lateral epicondylalgia. The pilot randomized controlled trial was carried out from January to April 2022 in Chennai, India. The major goal was to determine the superiority of HSR training over conventional exercise for managing lateral epicondylalgia.
The study included 24 individuals with unilateral lateral epicondylalgia recruited from an outpatient physiotherapy department. Participants were 45 to 65 years old and had a clinical diagnosis of lateral epicondylalgia, as verified by positive Cozen’s and Mill’s tests, with symptoms lasting more than a year.
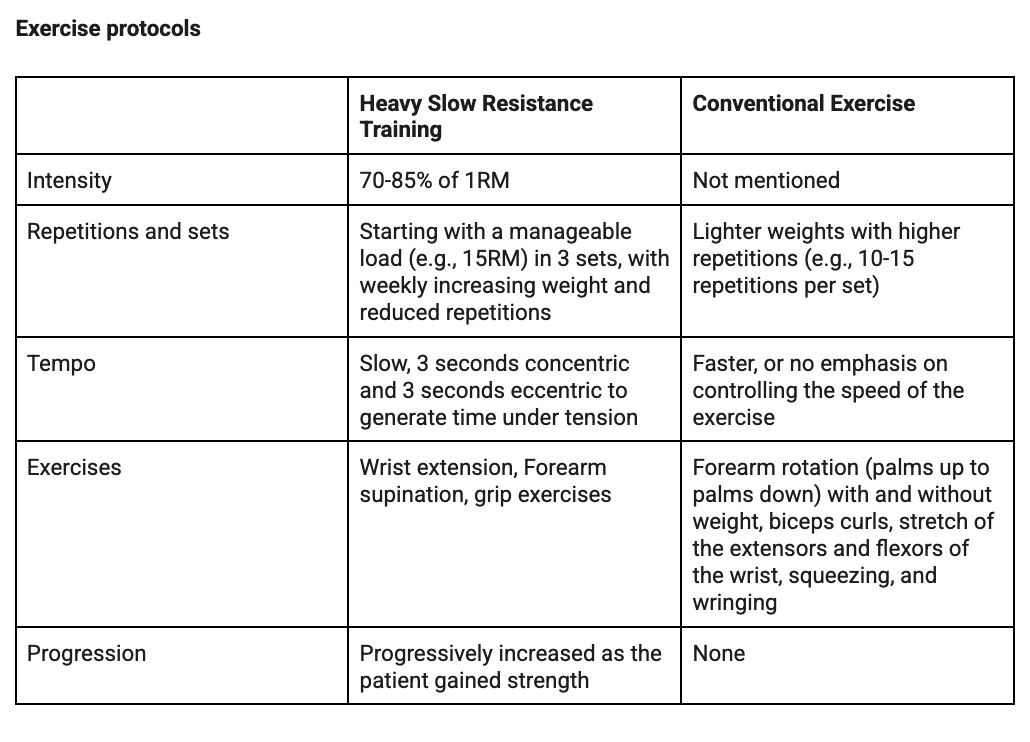
Using simple random sampling, the participants were divided evenly into two groups: the Heavy Slow Resistance Training Group (n=12) and the conventional exercise group. The intervention lasted 12 weeks, with three 30-minute exercise sessions per week.
Data collection involved pre- and post-intervention assessments at week 0 and week 12 using three primary outcome measures:
- Patient-Rated Tennis Elbow Evaluation (PRTEE) questionnaire: A 15-item self-report questionnaire assessing forearm pain (5 items) and functional limitations (10 items, divided into specific activities and usual activities), scored on a 0-10 scale. A lower score indicates less pain and disability.
- Patient-Specific Functional Scale (PSFS)
- Pain-Free Grip Test (PFGT): Measured using a hand-held dynamometer, with the best of three attempts recorded after a maximum 1-minute break between tests. PFGT is considered more clinically effective for lateral epicondylalgia than maximum grip testing, as gripping is a typical pain-producing activity.
Резултати
The study found statistically significant improvements in both groups after 12 weeks, with the HSR group demonstrating superior effectiveness.
- PRTEE Scores: No significant difference was observed in pre-test PRTEE scores between groups. Whereas, in post-test results, there was a statistically significant difference, with the HSR group showing greater reduction in symptoms. The effect size (Cohen’s d) for PRTEE post-test results between groups was -1.49, indicating a large effect in favor of HSR exercises, suggesting substantially more effective symptom reduction.
- Patient-Specific Activity Scoring Scheme (PSFS): Post-test outcomes revealed a statistically significant disparity between the groups. The effect size (Cohen’s d) was -0.11, indicating a small effect in favor of the HSR group, suggesting only slightly more improvement in patient-specific functional activities compared to CE.
- Grip Strength: The HSR group demonstrated higher mean values post-test compared to the CE group, with a significant increase in the HSR group. The effect size (Cohen’s d) for grip strength was 0.33, showing a small-to-medium improvement for the HSR group.
- Clinical Relevance (NNT): Based on PRTEE score improvement, the NNT for HSR was 5. This means that for every 5 patients treated with HSR, one additional patient would experience significant clinical improvement compared to CE, highlighting HSR’s strong practical impact.
Питања и размишљања
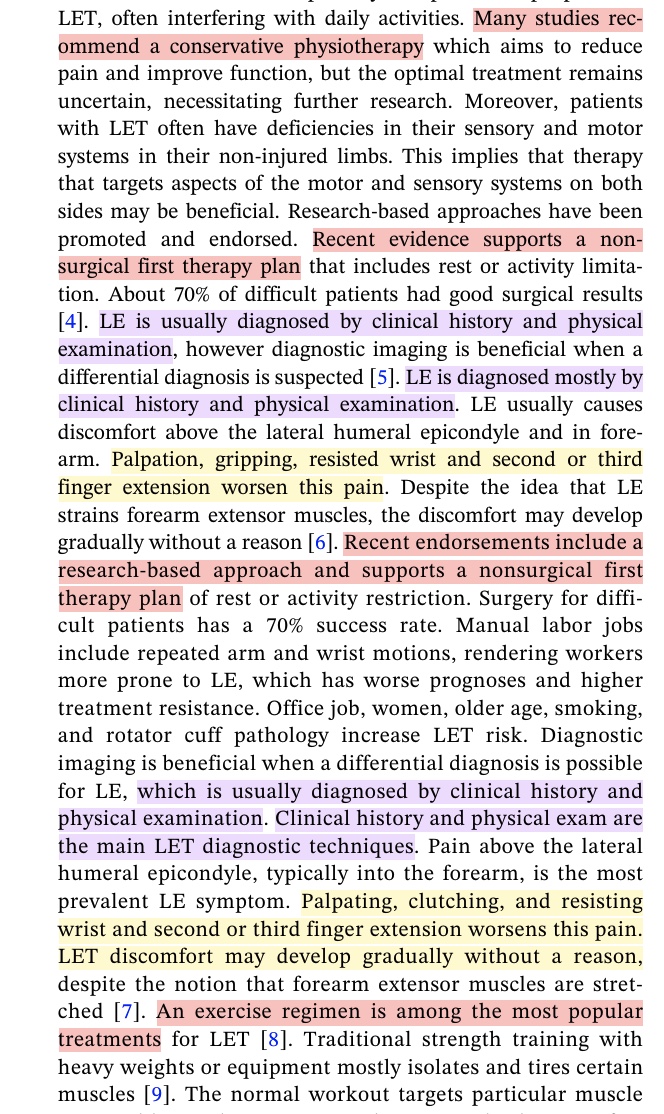
The Health Care Science journal in which this article was published is new and not yet indexed with a Journal Impact Factor rank. I wonder how this article was published, but I assume it may be due to the relatively new Journal wanting to publish often. The title of the paper already contains a typo, which may seem of minor importance, but “conventional” was misspelled as “convectional” which gives a whole different meaning. Further down the article, the author repeats the same text over and over, and the article reads difficultly, as can be seen in the two excerpts below.
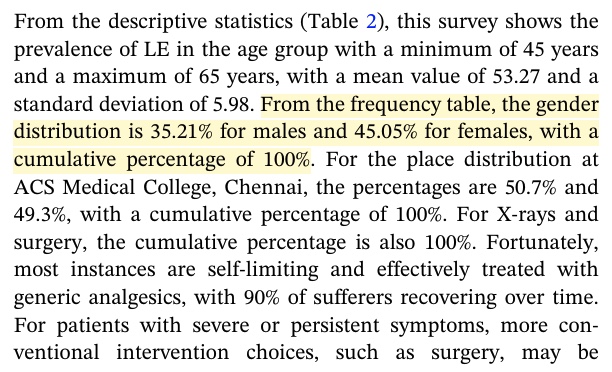
Mistakes are made throughout the article, 35.21% + 45.05% equals 80.26% and not 100%. This leaves me wondering whether subjects were purposely excluded for data analyses.
The HSR training for lateral epicondylalgia assumes a, what’s in a name, heavy resistance protocol. While the authors aim for a heavy weight, they let the participants perform 3×15 repetitions, indicating that a lower weight was used. This invalidates the HSR training protocol that was the aim of this research.
Furthermore, the text contains weird explanations about the exercises, for example:
- Using the anatomical terminology and landmarks would enhance readability. Instead, the authors describe movements and positions in an odd language:
- “In a right angle, the elbow is bent.”
- “With the elbow flexed at a straight angle, the hand stretched outward with the palm facing up, and the wrist flexed inward toward the body..”
- The concept of heavy slow resistance training has nothing to do with age and having to do slower exercises
- “Utilizing a slow training approach is a very efficient strategy for middle‐aged and older individuals to enhance their muscular strength.”
Причај ми штреберски
There is a lot to discuss about the Divya Mary et al. (2025) publication.
Firstly, the study does not mention any trial registration or provide a registration number. This is a significant omission, as trial registration is crucial for transparency, preventing selective reporting, and reducing publication bias.
Secondly, while the abstract and discussion mention that blinding procedures were in place, the study does not specify who was blinded (e.g., participants, therapists, outcome assessors) or how blinding was implemented.
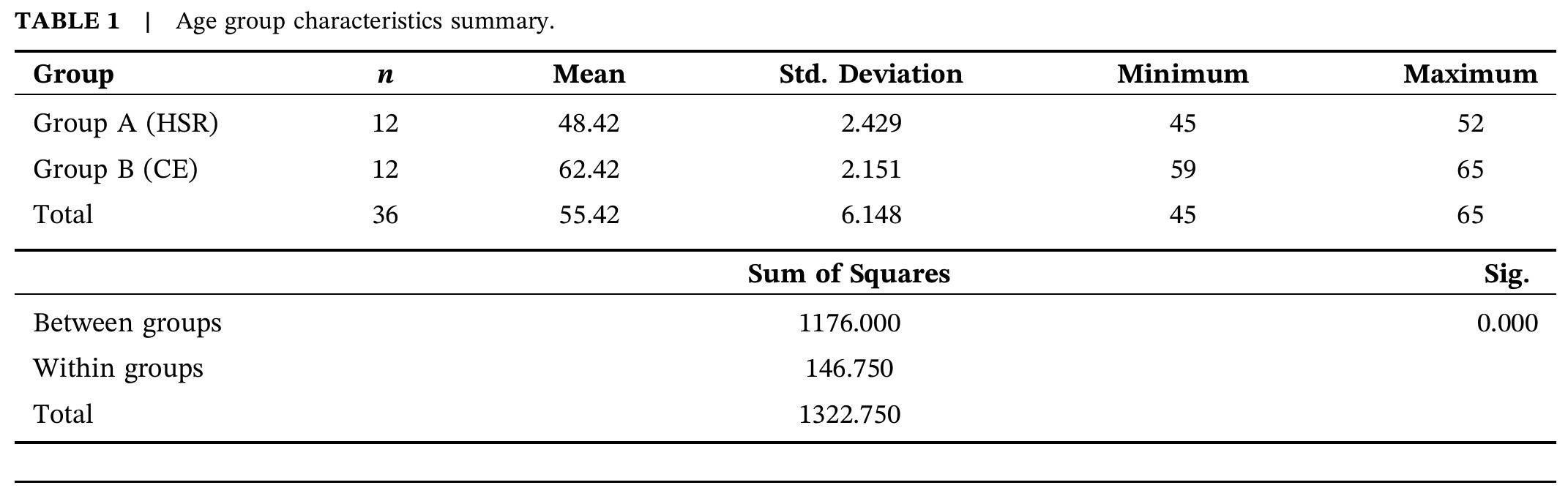
Thirdly, the study lacks a detailed flow diagram illustrating the number of participants at each stage. While a basic diagram shows n=24 randomized into two groups of 12, it lacks the initial stages of participant recruitment, including how many were screened, eligible, and excluded with specific reasons. This missing information prevents a clear understanding of the representativeness of the sample and potential selection bias. In Table 1, 12 participants in the HSR group and 12 in the conventional group are mentioned, and the total study population is summed to 36 participants, indicating that a potential bias in selective recruitment took place.
Fourthly, the explanation regarding sample size calculation and justification is somewhat contradictory and unclear.
- The study states, “From the early published report, it was estimated that 15 patients for each group were sufficient to detect a 40% difference in effect of exercise and its score improvement between the pre- and post-groups at p<0.05 with 80% power.” It then mentions, “But we have used 24 patients sample size which were more than sufficient. The sample size was also calculated using the formula.. and found a power of 0.80.”
- While they state a power of 0.80 was achieved with 24 patients, the exact delta (difference) they aimed to detect with this sample size for each outcome measure (PRTEE, PSFS, grip strength) is not explicitly stated. The statement about “40% difference” seems to refer to a previous study, not necessarily their own specific calculation for the 24 participants.
- It’s stated that 24 patients “were more than sufficient,” which implies they might have aimed for something different than what they ended up with. Clarity here is lacking.
Fifth, regarding baseline data, Table 1 shows a significant difference between groups for age, indicating a failure of randomization to achieve comparable groups at baseline. Table 2 lists demographics as percentages of the total sample, not separately for each group, making it impossible to confirm if other important baseline characteristics were comparable. The difference in age between the groups invalidates the findings since this imbalance implies that the “HSR is superior” conclusion might be heavily influenced by the HSR group being significantly younger and likely having better recovery potential regardless of the intervention.
Sixth, there is no mention of how adherence to the exercise protocols was monitored for either group, which is crucial for a 12-week home-based component and makes it hard to trust that the intervention was delivered as intended. For a 12-week home-based component (implied by “can be done at any time of day without professional supervision”), adherence is crucial, and its absence makes it hard to trust the intervention was delivered as intended.
Seventh, the article does not report any adverse events or harms experienced by participants in either group. While it’s a pilot study, reporting any discomfort, exacerbation of pain, or other negative outcomes is important for safety and generalizability.
Finally, while the discussion acknowledges the limitation of being conducted at a single institution, the severe age imbalance between the two groups is a much larger threat to generalizability and implies the conclusion might be heavily influenced by the HSR group being significantly younger. Yet, this threat is not discussed as a limitation.
Take-home messages
In conclusion, while the study by Divya Mary et al. (2025) attempts to compare two exercise approaches and presents some positive results for Heavy Slow Resistance training for lateral epicondylalgia, its adherence to CONSORT guidelines is weak or non-existent, particularly regarding randomization success, detailed blinding, and comprehensive reporting of baseline characteristics and recruitment flow. The significant age difference between the groups, left unaddressed as a limitation, is a major methodological flaw that compromises the validity and interpretability of the findings. Next week, we’ll discuss another pilot study about the impact of HSR training in lateral epicondylalgia and how to conduct research!
Референце
Сазнајте више
Лечење латералне тендинопатије лакта (познате и као тениски лакат): преглед
Погледајте два 100% бесплатна вебинара о боловима у рамену и боловима у зглобу на страни улне
Побољшајте своје клиничко образложење за преписивање вежби код активне особе са болом у рамену са Ендруом манжетом и навигирајте клиничком дијагнозом и управљањем са студијом случаја голфера са Томасом Мичелом