Research
Ankle/Foot
February 23, 2026
Strength Training along with Aerobic Exercise for Improving Peripheral Arterial Disease Outcomes

Увод
Peripheral arterial disease is a condition affecting a significant number of people living in Western countries. It leads to a cascade of reduced walking tolerance and deconditioning, accompanied by muscular loss and fat mass increases, further negatively contributing to the disease. In the previous research review, we aimed to improve clinical recognition of peripheral lower limb arterial disease and highlight vascular screening procedures that may be underused in physiotherapy. Today, we will highlight the possible interventions that a physiotherapist may incorporate.
Aerobic exercise programs like (supervised) (treadmill) walking have been proposed to counter the negative effects associated with the condition. Others have proposed strength training. To date, neither of the two options has been examined when integrated. The addition of strength training can be an interesting perspective for the physiotherapy-led exercise program, especially since sarcopenia is common in individuals affected by peripheral arterial disease. Therefore, the authors examined whether a combination of strength training along with aerobic exercise helps improve peripheral arterial disease outcomes.
Методе
This was a pilot study involving male participants with peripheral arterial disease, resulting in claudication. Eligible candidates had a resting Ankle-Brachial Index (ABI) of 0.90 or less and reported claudication limiting their maximal walking distance to less than 500m.
Participants were (not randomly) assigned to either the 6-month supervised exercise program (SUP), where a combination of progressive treadmill walking and resistance training exercises was performed, or to usual care (UC).
Supervised exercise program (SUP):
During 6 months, the participants were training 3 times per week. Sessions of treadmill walking started at 20 minutes and progressed to 40 minutes. They were asked to rest (on a chair) when mild-to-moderate claudication pain arose and could complete further walking when pain subsided. The work-rest cycle was repeated until the total walking time was achieved or when the total session (including rest periods) achieved 50 minutes. The intensity was gradually increased by increasing the speed and the inclination, based on the claudication pain level. After the walking part, the subjects performed strength training exercises, which were progressed from 1 set of 10 repetitions to 3 sets of 15 repetitions. Emphasis was placed on movement quality and the complete range of motion of the exercise.
Usual care
The usual care group was advised to walk for at least 40 minutes, 3 times per week. They also received guidance on how to adjust the intensity of walking (speed, duration, routes with varying grades), based on their claudication intensity at the follow-up moments.
Participants in both groups received the advice to adopt a more active lifestyle and manage known risk factors for peripheral arterial disease.
Outcomes
All participants were asked to come to the testing in a fasting state in the morning, and all measures were obtained after consuming a light meal (crackers and water). The primary outcome was the walking ability of the participant. This was quantified using the six-minute walk test (6MWT). Using the 6MWT, the following variables were derived:
- Claudication onset distance (COD): The total distance walked until the claudication was reported
- Absolute claudication distance (ACD): The distance at which the participant stops walking due to claudication pain
- Maximal walking distance (MWD): The maximal distance covered during the 6MWT
The minimal clinically important difference (MCID) of the 6MWT is reported to range between 54m and 80m.
Secondary outcomes included:
- Derived from the 6MWT:
- Claudication onset time (COT): The time until claudication is reported
- Absolute claudication time (ACT): The total time spent walking with claudication
- Maximal walking time (MWT): The effective walking time, without pauses
- Pause duration
- Average walking speed
- Walking speed without claudication
- Walking speed with claudication
- Physical fitness:
- Handgrip strength: measured using a hand dynamometer, with the highest value from three attempts
- Lower body strength: assessed with the 30-second chair stand test
- Lower body and back flexibility: evaluated using the chair sit-and-reach test
- Body composition was analyzed with a bioimpedance scale, measuring body weight, fat mass, fat-free mass, and the total body water
- Peripheral vascular outcomes:
- Ankle-Brachial Index: this was obtained after a 15-minute resting period in a supine position. Three consecutive systolic blood pressure measures were taken in the A. Brachialis, and the A. Dorsalis Pedis and A. Tibialis Posterior, bilaterally.
- Ultrasound peripheral blood flow recorded the time-average-mean velocity, flow volume, and artery caliber of the A. Brachialis, and the A. Dorsalis Pedis and A. Tibialis Posterior, bilaterally.
All outcomes were obtained at baseline (M0), 3 months (M3), and 6 months (M6).
Резултати
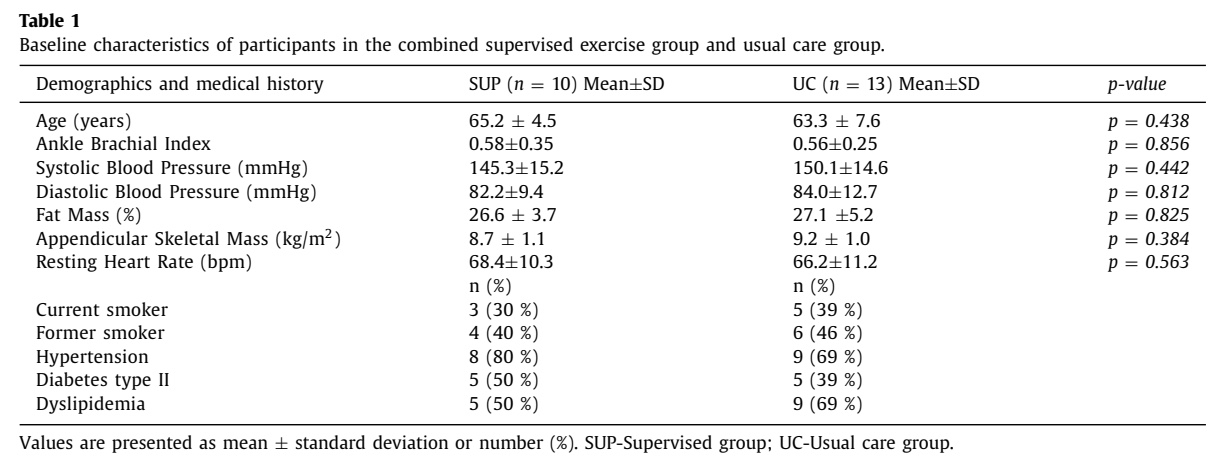
Twenty-three male participants were included in the study. The groups were comparable at baseline.
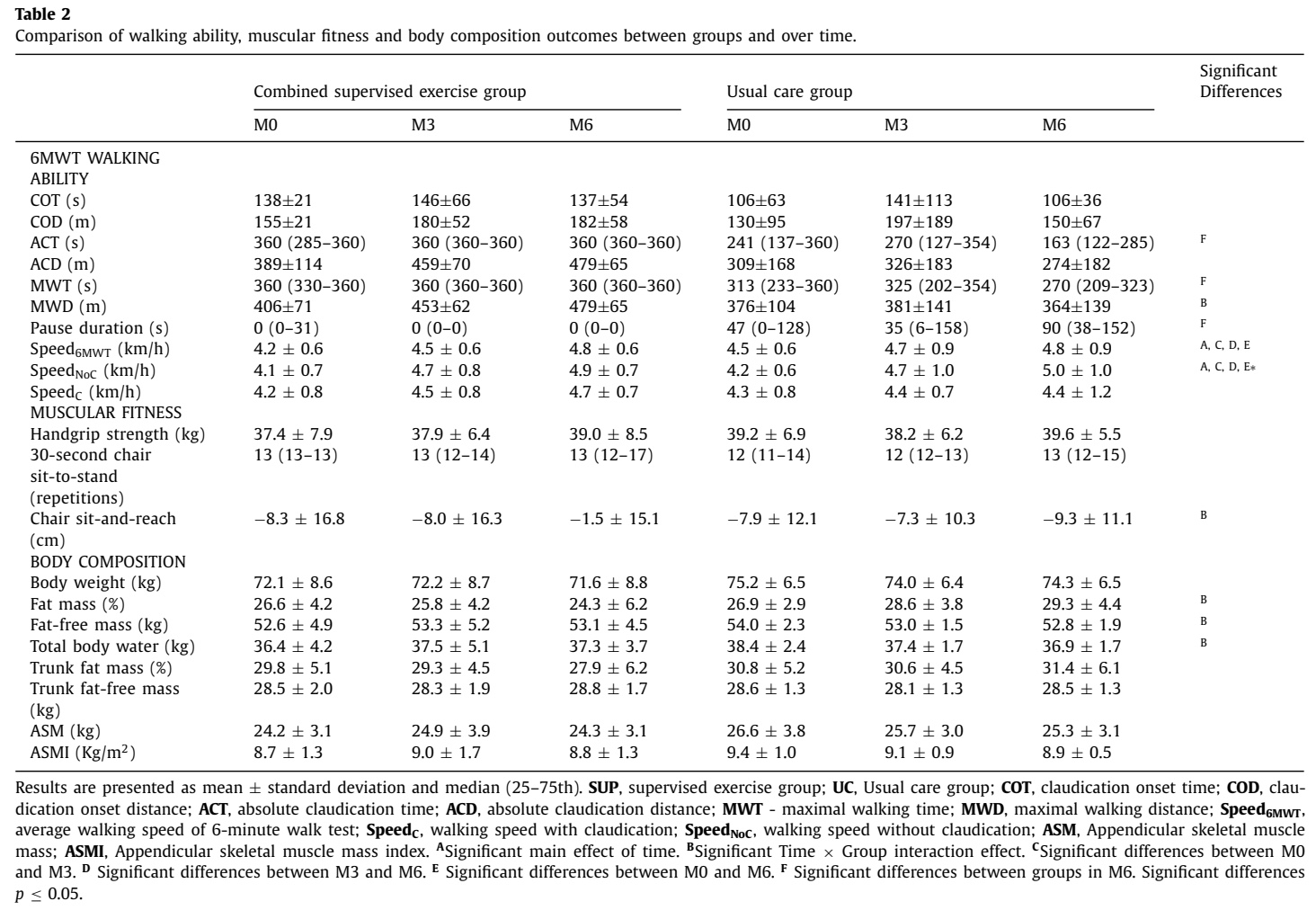
The results regarding the primary outcome, walking ability, revealed a time x group interaction effect in the maximal walking distance (MWD) covered. The supervised exercise group (SUP) could walk 73m more at 6 months, compared to baseline, whereas the covered distance decreased from 376m to 364m in the usual care (UC) group. This difference exceeded the minimal clinically important difference.
Interestingly, the claudication onset distance (COD) did not demonstrate any significant time or time x group interaction effects. Regarding the outcome absolute claudication distance (ACD), the SUP group increased their distance by approximately 90m from 389m (+/- 114m) to 479m (+/- 65m), while the UC group saw a decline from more than 30m, from 309m (+/- 168m) to 274m (+/- 182). Despite the apparent mean difference between the groups, the time x group interaction showed no significant effect.
Питања и размишљања
How is it possible that the participants in the SUP group were able to walk further than those in the UC, despite no changes being seen in the claudication onset distance or absolute claudication distance?
The lack of a significant change in COD and ACD between groups suggests that the underlying vascular pathology (the distance at which blood flow restriction causes pain) did not significantly change. The participants who engaged in supervised progressive aerobic and strength training did not demonstrate a statistically significant difference in the distance at which they reported the onset of claudication symptoms and the distance at which they were compelled to rest, when compared to the usual care (UC) participants. Nonetheless, they were able to cover a significantly greater overall distance compared to both the UC group and their own baseline measurements.
The authors explained that these observations are related to improved pain tolerance or a better understanding of pain. Since everyone received specific pain management guidance during the exercise sessions, the participants got steered on when to stop and when to resume walking. Probably, they experienced less fear, or they had an increased understanding of the nature of their symptoms. Or it could be that they knew they were not worsening things, as they could now better tolerate certain pain levels. Their threshold for stopping became higher.
Secondary outcomes demonstrated that the SUP group showed significant improvements in both ACT and MWT at M6, while the UC group’s performance worsened. Interestingly enough, the SUP group’s ability to cover more distance is strongly supported by their improved 6MWT and the elimination of pauses during the 6-minute walk test (6MWT). The SUP group was able to walk for the entire 6 minutes without stopping. In stark contrast, the Usual Care (UC) group needed to stop to relieve pain, resulting in an average pause duration of over 1 minute at 6 months. This increased resting time directly reduced their MWD. No between-group difference was observed in walking speed.
A significant time x group interaction was observed in the sit-and-reach test in favor of the SUP group. The body composition outcomes demonstrated significant time x group interactions for the fat mass, fat-free mass, and total body water, in favor of the SUP group. This means that the SUP group’s body parameters changed towards becoming more muscular, while the UC group showed an increase in fat mass over the 6 months.
It therefore appears that the combination of aerobic exercise and resistance training is beneficial in improving peripheral arterial disease outcomes.
Причај ми штреберски
The primary limitation of the study is the lack of randomization, as it was a pilot study. Furthermore, there was a possibility for selection bias since the creation of groups was based on those who were able to come to the hospital three times per week for the supervised training, whereas those unable were prescribed the usual care. Without a randomized assignment process, it is impossible to be certain that the characteristics of the participants in the groups were comparable at baseline. This non-random allocation means that systematic differences between the groups, beyond the intervention itself, could be responsible for the observed outcomes, making it difficult to establish a clear cause-and-effect relationship. Researchers must acknowledge that unmeasured confounders, such as baseline disease severity, comorbidity profiles, or socioeconomic factors, may have disproportionately influenced one group over the other, thereby skewing the results.
A further methodological concern is the absence of a correction for multiple comparisons. When numerous statistical tests are performed on the same dataset, the probability of obtaining a statistically significant result purely by chance increases. The failure to apply a suitable correction, such as the Bonferroni correction, means that some of the reported significant findings may be spurious. This compromises the robustness and reliability of the statistical inferences drawn from the data.
Despite these limitations, a notable positive finding was the high adherence rates across both groups. This suggests that the interventions were feasible, well-tolerated, and acceptable to the participant population. High adherence is a critical factor for the internal validity of an intervention study, as it ensures that participants actually received the intended dose and duration of the intervention, thus maximizing the potential for observing a true effect. High adherence outcomes and completion rates in the SUP group (both exceeding 80%), despite a very intensive training program from 3 sessions per week over a significant period of 6 months, showed that the efforts did not hold the participants back. They demonstrated that combining aerobic and resistance training under guidance led to improved peripheral arterial disease outcomes. The observed adherence rates suggest that the evaluated strategies hold promise in a real-world setting, provided future, methodologically sound studies can confirm their efficacy.
Поруке за понети кући
The combination of aerobic exercise and resistance training is beneficial in improving peripheral arterial disease outcomes. A significant increase in the maximal distance covered during the 6-minute walk test, despite no change in claudication onset distance or absolute claudication distance, means that the participants got to tolerate and manage their symptoms more effectively.
Together with improving key body composition parameters, favoring the preservation of or gain in muscle mass, is a crucial effect that walking alone could probably not achieve. This paper is a preliminary research study, but showing promising results that could be investigated further. An important call for engagement in more resistance training exercises is needed, since less than a quarter of adults meet the guidelines for muscle-strengthening exercise. This study demonstrated that improving peripheral arterial disease outcomes is possible when combining regular aerobic training with resistance training exercises.
Референце
100% БЕСПЛАТАН ПАКЕТ ПОСТЕРА
Добијте 6 постера високе резолуције који сумирају важне теме у спортском опоравку за излагање у вашој клиници/теретани.