
Research
Exercise
December 1, 2025
Рехабилитација упорне постуралне перцептивне вртоглавице: Увиди из систематског прегледа са мета-анализама.

Увод
Persistent Postural-Perceptual Dizziness (PPPD) is a chronic functional vestibular disorder characterized by persistent non-rotational dizziness, unsteadiness, and vertigo lasting at least three months. Symptoms typically worsen with upright posture, movement, or exposure to complex visual environments, and often follow an event that initially caused acute vertigo or imbalance. PPPD stems from maladaptive postural control and central vestibular processing rather than structural vestibular damage.
Although Selective Serotonin reuptake inhibitors (SSRIs) and psychotherapy can offer short-term benefit, side effects and limited evidence restrict their effectiveness. Vestibular rehabilitation therapy (VRT) uses graded eye, head movements, and exercise to promote vestibular compensation, adaptation, and habituation. It can improve dizziness, balance, and daily function, and is considered a safe and non-invasive option. While some studies support VRT for PPPD, current evidence is limited by small samples and methodological inconsistencies. Previous reviews have been largely descriptive. The present meta-analysis quantitatively synthesizes available studies using the Dizziness Handicap Inventory (DHI) as the primary outcome to provide stronger evidence for the efficacy of Persistent Postural Perceptual Dizziness rehabilitation.
Методе
The research was conducted in accordance with PRISMA guidelines.
Inclusion criteria
The search included publicly available, English-language studies that met the following criteria:
- Participants: Individuals of any age, sex, or country diagnosed with PPPD according to clinical presentation and the Bárány Society diagnostic criteria.
- Intervention: Patients received vestibular rehabilitation therapy (VRT) following confirmation of PPPD. Baseline and post-treatment outcome measures—particularly Dizziness Handicap Inventory (DHI) scores—had to be reported.
- Outcomes: Studies assessed PPPD-related symptoms using measures of vestibular function, quality of life, physical performance, functional balance, or emotional well-being, with the DHI as the preferred outcome metric. The DHI minimal clinically important difference is 18 points.
Exclusion criteria
Two reviewers independently extracted data, with disagreements resolved through consultation with a third author. Studies were excluded if they:
- Were duplicates or irrelevant to the research question;
- Consisted of reviews, letters, case reports, or commentaries;
- Did not present original research data;
- Involved non-human subjects.
Data extraction
Using a standardized data collection form, two independent reviewers extracted key information from all eligible studies, including author name, year of publication, participant characteristics, intervention and control conditions, intervention duration, and reported outcome measures. Effect estimates and their 95% confidence intervals were recorded based on the analyses adjusted for the highest number of confounding factors.
Quality assessment
Two reviewers independently assessed the methodological quality and risk of bias of the included studies using the Newcastle–Ottawa Scale (NOS), selected for its suitability in evaluating non-randomized research, particularly regarding selection bias and outcome ascertainment. Any disagreements were reviewed in detail, and unresolved issues were resolved through consultation with a third reviewer to reach a consensus.
Statistical analysis
Continuous outcomes were summarized as mean ± standard deviation. When studies reported medians and quartiles instead of means and standard deviations, these values were estimated following the method of Wan et al. Statistical significance was defined as p < 0.05 with 95% confidence intervals.
The weighted mean difference (WMD) was used as the effect measure. WMD represents the average difference in an outcome (e.g., DHI scores) between pre- and post-intervention or between intervention and control groups, while assigning greater weight to studies with larger sample sizes or lower variance.
Study heterogeneity—the degree to which study results differ from one another beyond what would be expected by chance—was evaluated using the Cochrane Q statistic and the I² index. Heterogeneity may arise from differences in study populations, intervention protocols, measurement tools, or methodological quality. When significant heterogeneity was detected (p < 0.05 for Q or I² > 50%), a random-effects model was applied, assuming that the true effect varies across studies. When heterogeneity was low (I² < 50%), a fixed-effects model was used, assuming a single underlying true effect. Publication bias was assessed visually using funnel plots.
Results
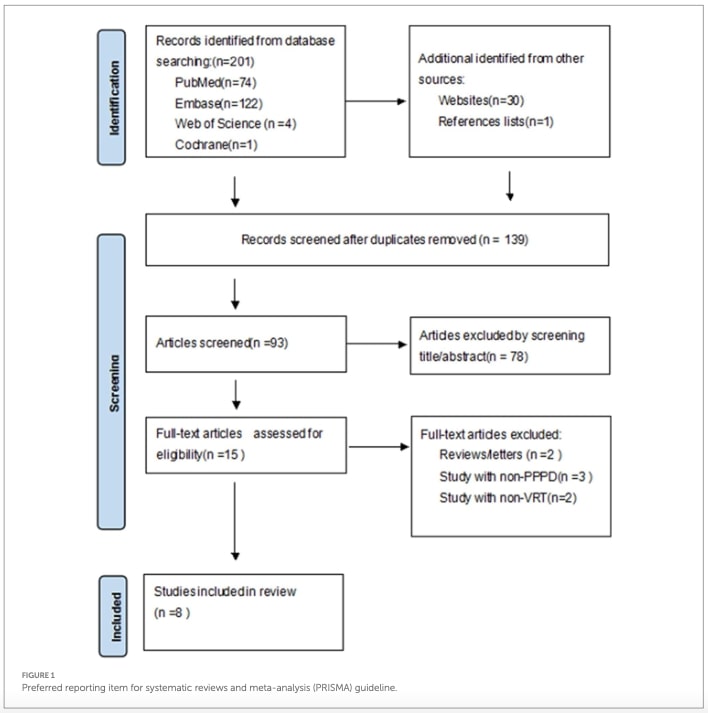
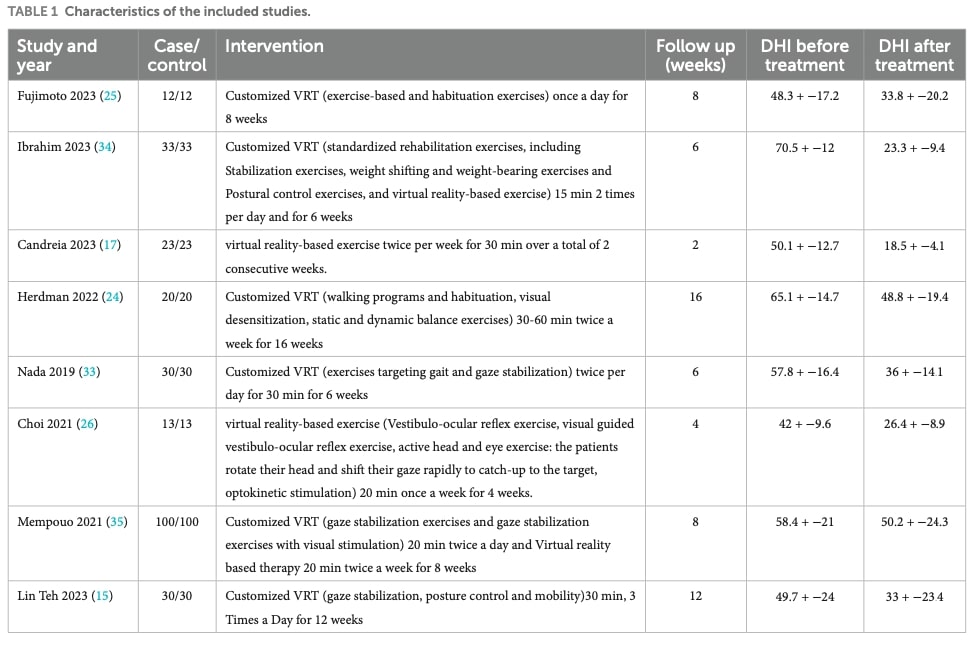
Figure 1 illustrates the study selection process, showing how the eligible studies were identified and screened before being included in the quantitative analysis and subsequent meta-analysis. Table 1 is further providing details about each included study.
Primary results
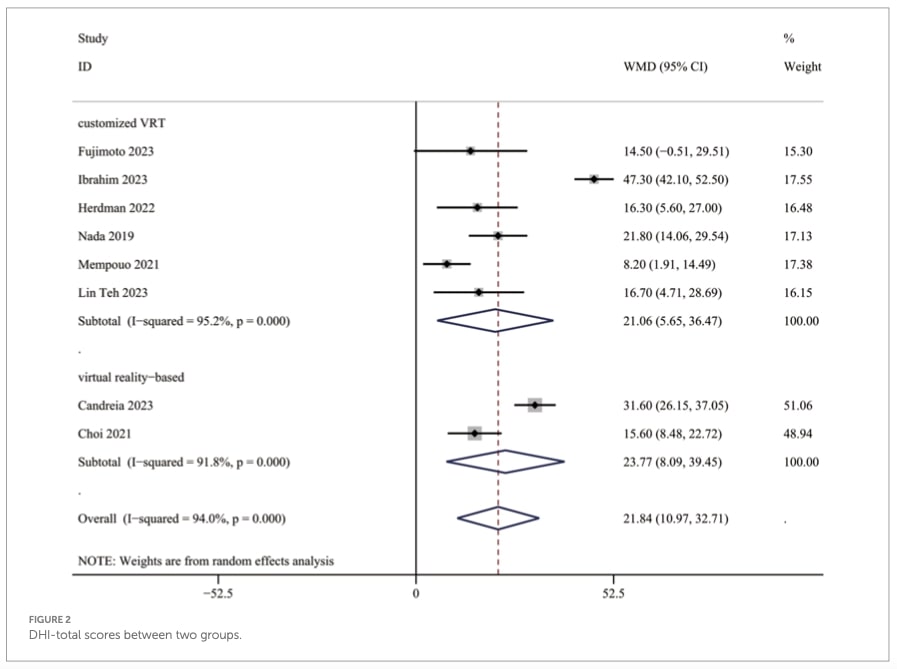
Pooled DHI-total data from all eight studies (522 participants) showed a significant benefit of Persistent Postural Perceptual Dizziness rehabilitation compared with control interventions WMD = 21.84 (see Figure 2).
Subgroup analysis of DHI-total scores
Studies were stratified by Persistent Postural Perceptual Dizziness rehabilitation type: customized VRT and virtual reality–based VRT. Both approaches produced significant reductions in DHI-total scores among patients with PPPD. Customized VRT showed an improvement of WMD = 21.06, while virtual reality–based Persistent Postural Perceptual Dizziness rehabilitation demonstrated a similar benefit WMD = 23.77 (see Figure 2).
Secondary outcomes: meta-analysis of DHI physical, emotional, and functional subscales
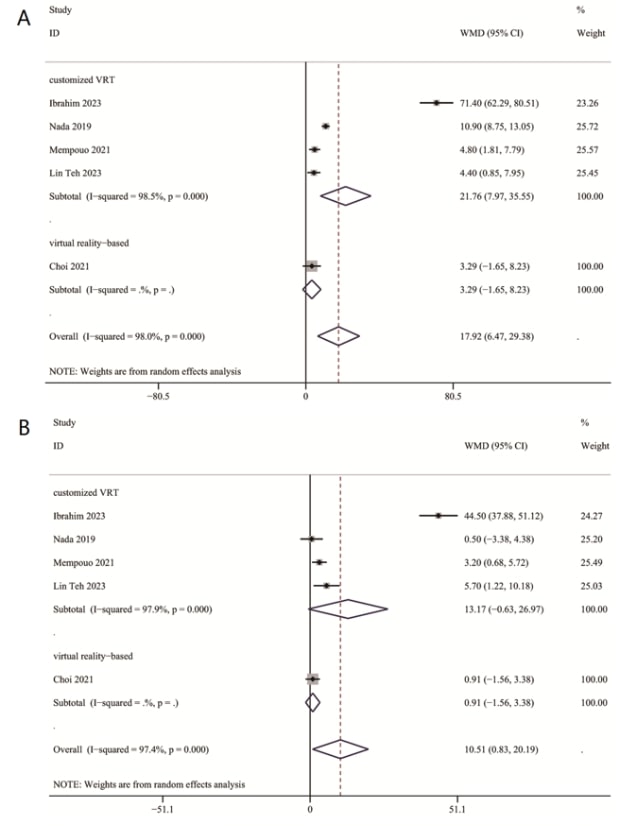
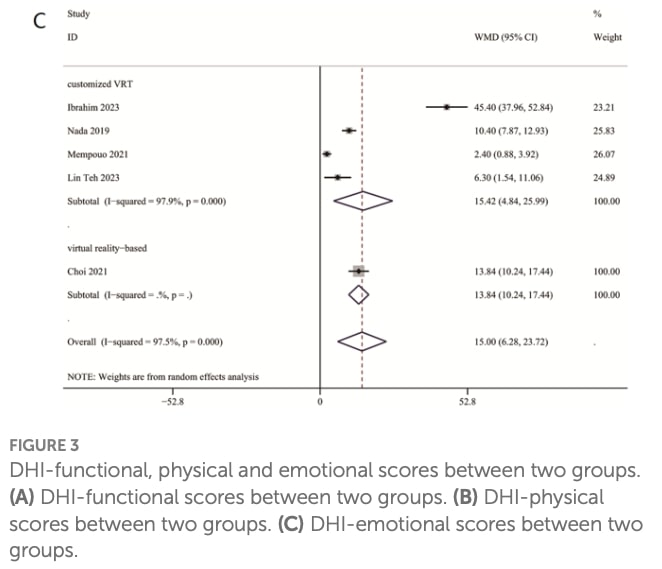
Pooled data from five studies (412 participants) showed that Persistent Postural Perceptual Dizziness rehabilitation significantly outperformed control interventions across all DHI subscales. Improvements were observed in the physical domain, emotional domain, and functional domain (Figures 3A–C).
Subgroup analysis of DHI functional, physical, and emotional scores
In the subgroup analysis, customized VRT produced significant improvements in DHI-functional and DHI-physical scores, but not in DHI-emotional scores.
Virtual reality–based VRT led to significant gains only in DHI-functional scores, with no significant changes observed in the emotional or physical domains.
Питања и мисли
The study applied very limited exclusion criteria, and several potentially important factors—such as intervention duration, intervention modality (e.g., virtual reality–based programs), or comorbid diagnoses—were not considered. Because the inclusion criteria were so broad, substantial clinical heterogeneity was introduced, which likely contributed to the high I² values (see Figure 2 and 3) reported and therefore weakened the overall strength and interpretability of the meta-analysis. In addition, the authors provided almost no information about the nature of the control interventions (e.g., sham therapy, wait-and-see, usual care), making it difficult to assess the true magnitude of the treatment effect.
An interesting observation is that virtual-reality–based VRT did not significantly improve DHI-emotional or DHI-physical subscale scores. (Although, as discussed in the Talk to Me Nerdy section, the way the results are presented in the figures introduces confusion and possible labeling errors.) This finding is somewhat unexpected: if the DHI-total score improves, one would generally anticipate proportional reductions in both the physical and emotional subscales. Similarly, customized VRT did not demonstrate improvement in emotional outcomes, which again appears counterintuitive since improvements in physical symptoms would theoretically alleviate emotional distress. The close interaction between physical and emotional symptomatology in PPPD is well recognized, and one might expect improvements in one domain to positively influence the other.
One could interpret these findings as such: emotional symptoms in PPPD may represent an independent contributing factor rather than a secondary consequence of physical dysfunction. Further research is needed to explore the structural and psychological mechanisms linking physical and emotional components in PPPD, and to clarify whether emotional symptoms require targeted interventions beyond conventional VRT.
It is also worth noting that the virtual-reality interventions included in the meta-analysis were of very low intensity: most were delivered only twice per week and over extremely short durations (one study involved just two weeks of treatment). Moreover, very few studies included in this review, investigated VR-based VRT, which makes it difficult to draw firm conclusions about its efficacy for Persistent Postural Perceptual Dizziness rehabilitation. More rigorous, adequately dosed, and longer-term VR interventions are needed before determining their true therapeutic value.
Причај ми штреберски
Although the authors state explicitly in the text that the DHI-emotional (DHI-E) subscale did not show a significant reduction in the VRT subgroup analysis, the corresponding figures appear inconsistently labelled. The article reports the following results:
“In subgroup analysis, customized VRT demonstrated significant reductions in both DHI-F (WMD = 15.42, 95%CI: [4.84, 25.99]) and DHI-P (WMD = 21.76, 95%CI: [7.97, 35.55]) scores, but not in DHI-E (WMD = 13.17, 95%CI: [−0.63, 26.97]). Virtual reality–based VRT showed improvement in DHI-F scores (WMD = 13.84, 95%CI: [10.24, 17.44]), but not in DHI-E (WMD = 0.91, 95%CI: [−1.56, 3.38]) or DHI-P (WMD = 3.29, 95%CI: [−1.65, 8.23]).”
However, in Figure 3C, which is supposed to illustrate the DHI-emotional outcomes, the value reported for the virtual reality subgroup is WMD = 13.84 (95% CI: 10.24–17.44)—a result that actually corresponds to the DHI-functional (DHI-F) subscale. This mismatch strongly suggests that the authors mislabelled or mixed their data when preparing the figures, which markedly undermines the clarity and credibility of the results.
Figure 1 presents the overall DHI outcomes. For each study, the weighted mean difference (WMD) reflects the change in DHI score between the intervention and control groups. These WMDs are weighted according to sample size and variance. The distribution of effect sizes across studies is relatively consistent; however, the Ibrahim et al. study shows a markedly higher effect size compared with the others. Because the authors provide very limited methodological details for this specific study, it is difficult to determine whether this difference reflects a genuinely stronger intervention effect or the influence of confounding factors such as differences in exercise protocols or control group characteristics.
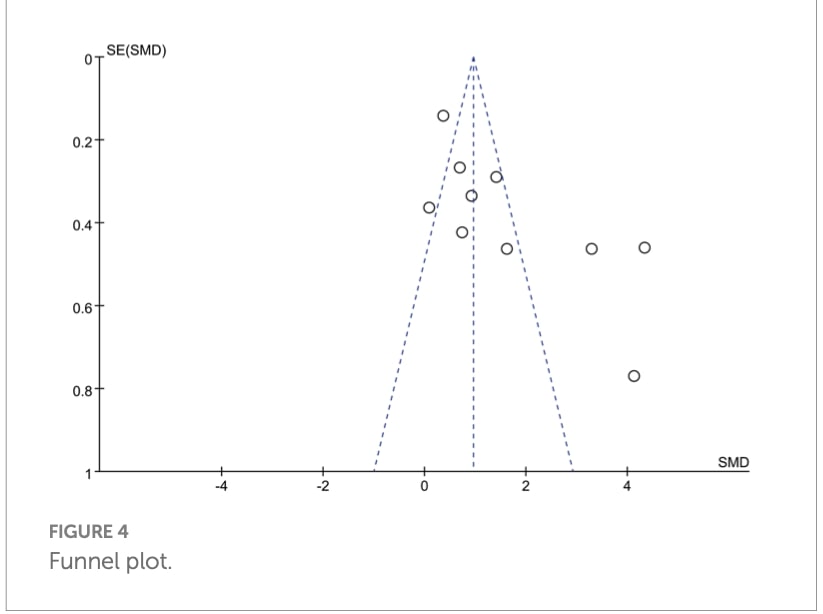
The funnel plots (Figure 4) suggest the possibility of publication bias. Studies reporting strong positive effects of vestibular rehabilitation appear more represented, whereas smaller studies with modest or negative outcomes may be missing from the available literature. This asymmetry is further reflected in the presence of small-study effects: several studies with higher standard errors (i.e., smaller sample sizes) report disproportionately large treatment effects. Such a pattern may indicate that smaller studies tend to overestimate the effectiveness of VRT, or alternatively, that small studies showing null or negative findings were not published.
The overall dispersion of points within the funnel plots also reflects considerable between-study heterogeneity. This variability aligns with the previously noted methodological differences across studies. Together, these tendencies—publication bias, small-study effects, and heterogeneity—highlight limitations in the current evidence base and warrant cautious interpretation of the pooled effect estimates.
Take-home Messages
- Vestibular Rehabilitation Therapy (VRT) is effective in reducing overall dizziness-related disability in PPPD, with consistent improvements in total DHI scores across studies.
- Improvements are primarily driven by the physical (DHI-P) and functional (DHI-F) domains, while emotional symptoms (DHI-E) show less consistent change.
- Customized VRT leads to significant improvements in DHI-P and DHI-F, but not in DHI-E.
- Virtual reality–based VRT improves DHI-F only and shows no significant effect on DHI-E or DHI-P.
- This pattern suggests that emotional distress in PPPD may be partially independent of physical symptoms, aligning with known links between PPPD, anxiety, and emotional dysregulation.
- Virtual reality (VR) shows potential but cannot yet be recommended as a standalone Persistent Postural Perceptual Dizziness rehabilitation treatment; existing studies are scarce, low in intensity (e.g., 2 sessions/week for 2 weeks), and too short to draw firm conclusions.
- High heterogeneity, possible publication bias, and several methodological limitations reduce the overall strength and certainty of the evidence.
This Physiotutors in person courses will further increase your knowledge and your skills with world leading experts in Persistent Postural Perception Dizziness.
Референце
Научите да лечите најчешћи узрок вртоглавице у овој БЕСПЛАТНОЈ мини-видео серији
Водећи стручњак за вестибуларну рехабилитацију Фират Кесгин води вас на тродневни видео курс о томе како препознати, процијенити и лијечити бенигно-пароксизмалну вртоглавицу задњег канала (БППВ)
