
Research
Knee
June 19, 2025
Post-Surgery Meniscus Rehabilitation: 2024 Consensus on Best Practices for Post-Op Physiotherapy (Meniscectomy, Repair & Reconstruction)

Introduction
This is the first of two articles examining the latest evidence-based approaches for post-surgery meniscus rehabilitation, with this installment focusing on post meniscectomy, repair, and reconstruction management. The follow-up will delve into conservative management of meniscal tears, ensuring a comprehensive guide for clinical practice.
Meniscus surgery remains one of the most frequently performed orthopedic procedures, yet rehabilitation protocols vary widely—often influenced by surgeon preference, regional practices, or outdated traditions. Contemporary surgical philosophy has shifted toward prioritizing meniscal preservation (repair and reconstruction) over menisectomy, necessitating updated evidence-based rehabilitation strategies that reflect these evolving approaches. However, clear guidelines for post-operative care—particularly in progression, load management, and functional recovery—have been lacking.
The first part of the consensus, reviewed here, delivers practical, surgery-specific recommendations to optimize recovery after meniscus procedures, while the second review, scheduled next week, will cover prevention, non-operative care, and return-to-sport criteria. By bridging research and clinical application, this consensus empowers Physiotherapists to move beyond anecdotal practices and align with globally endorsed standards.
Methods
To develop the first unified EU-US guidelines for post-surgery meniscus rehabilitation meniscus rehabilitation, European Society for Sports Traumatology and Arthroscopy (ESSKA), American Orthopedic Society for Sports Medicine (AOSSM), and American Academy of Sports Physical Therapy (AASPT) convened a diverse panel of orthopedic surgeons, physiotherapists, and sports medicine experts from Europe and the United States. Their goal was to bridge gaps in post-surgery meniscus rehabilitation protocols—ranging from meniscectomy to repair and reconstruction—using evidence-based consensus.
A Transparent, Two-Tiered Approach
The project leveraged a proven methodology from prior ESSKA consensus efforts:
Question Development: A clinical expert panel first identified critical rehabilitation priorities for meniscus injuries. Subsequently, an independent literature review team systematically evaluated 395+ studies from MEDLINE, Web of Science, and Scopus (without time restrictions) to address the specific research questions formulated by the clinical panel
Evidence Grading: Recommendations were crafted, based on questions raised by the “question group” and classified by level of evidence (LOE), from Grade A (high scientific support), Grade B (scientific presumptions), Grade C (low level of scientific support to Grade D (expert opinion).
The guideline development process employed rigorous methodology. First, an independent rating committee evaluated 29 clinical statements (addressing 19 key post-surgery meniscus rehabilitation questions) through a standardized 9-point Likert scale assessment of scientific validity and clinical applicability. Initial consensus criteria required a median score ≥7 for statement inclusion.
Statements falling below this threshold (median score <7) underwent a second round of focused refinement. Following this iterative process and final approval by the governing committees of ESSKA, AOSSM, and AASPT, the finalized clinical practice guidelines were optimized for worldwide implementation.
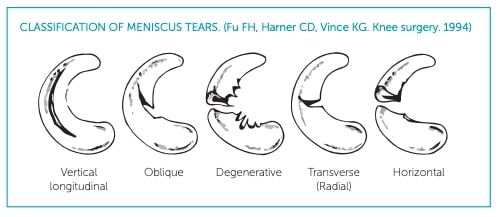
The following figure illustrates the meniscal tear classification system adopted for this consensus guideline.
Results
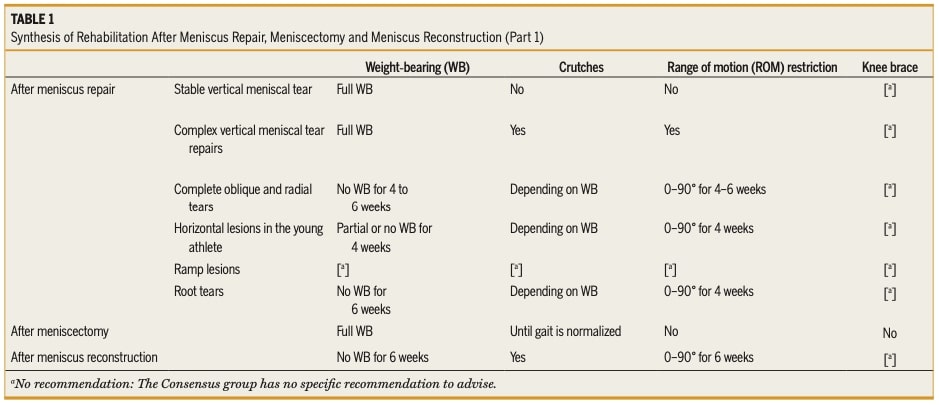
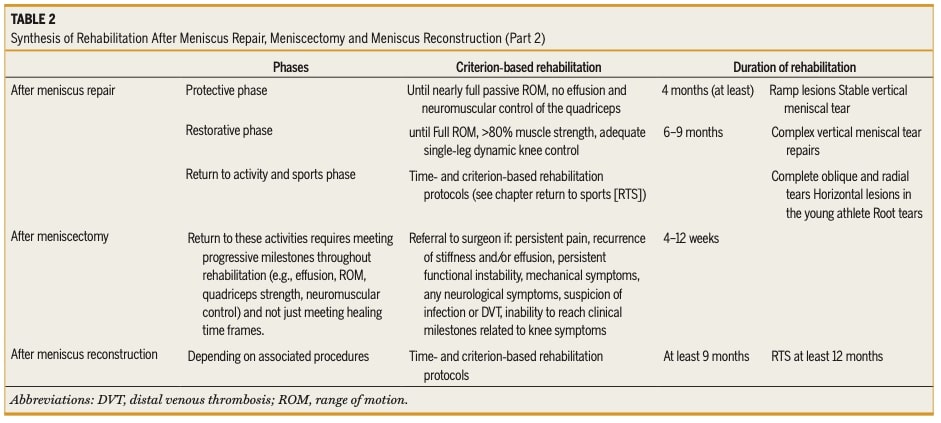
Rehabilitation guidelines are presented in table 1 and 2.
Rehabilitation management after partial meniscectomy
Currently, there is no standardized evidence-based rehabilitation protocol following partial meniscectomy, but a criterion-based approach focusing on functional milestones is recommended. Patients are typically permitted immediate full weight-bearing (FWB) and full range of motion as tolerated, with symptom guidance (Grade C).
While significant effusions are uncommon postoperatively, they may occur in certain populations—such as older individuals, those with a high BMI, or patients with comorbidities—and can lead to quadriceps inhibition, potentially necessitating temporary assistive devices (Grade D).
To address strength and neuromuscular control deficits, rehabilitation should incorporate neuromuscular electrical stimulation (NMES), open kinetic chain, and closed kinetic chain exercises, similar to protocols used after ACL reconstruction (Grade C). Agreement: Mean 8.4 ± 1.45, Median 8 (5–9), Relative agreement.
When comparing medial versus lateral partial meniscectomy, no distinct rehabilitation protocols exist. However, lateral meniscectomies may present more postoperative complications, including persistent swelling, pain, and a higher risk of early chondrolysis, which could delay return to high-impact activities compared to medial meniscectomies (Grade D). Agreement: Mean 7.8 ± 1.36, Median 8 (5–9), Relative agreement.
Regarding traumatic versus degenerative meniscus lesions (DMLs), there is no evidence supporting different rehabilitation protocols. However, patients with degenerative lesions may require a slower progression in rehab due to factors such as age, tissue quality, and associated joint degeneration (Grade D). Agreement: Mean 8.3 ± 1.51, Median 8 (5–9), Relative agreement.
Weight-bearing recommendations emphasize that full weight-bearing is allowed immediately after surgery (Grade A), though some patients may benefit from crutches temporarily until gait normalizes (Grade D). Agreement: Mean 8.4 ± 1.00, Median 8 (5–9) Relative agreement).
Rehabilitation duration varies, with most guidelines suggesting a 4- to 12-week timeframe for return to walking, work, and sport. However, recovery should be guided by functional milestones (e.g., resolution of effusion, restored ROM, adequate quadriceps strength, and neuromuscular control) rather than strict time-based criteria (Grade B). Persistent symptoms such as pain, recurrent effusion, stiffness, functional instability, mechanical symptoms, or signs of infection/DVT warrant referral back to the surgeon (Grade B). Failure to achieve expected clinical milestones should also prompt reevaluation (Grade D). Agreement: Mean 7.8 ± 1.02, Median 8 (5–9), Relative agreement.
Rehabilitation management after meniscus repair
While no single evidence-based rehabilitation protocol has been established as superior, post-operative rehab should be tailored based on several factors: the type and location of the meniscal tear, tissue quality and vascularity, surgical repair technique, and patient-specific factors that may influence healing (Grade D).
For isolated meniscal repairs, there is no strong evidence favoring specific protocols or adjunct therapies. However, when meniscal repair is performed alongside other procedures (such as ACL reconstruction), neuromuscular electrical stimulation (NMES) may aid early quadriceps reactivation (Grade D).
A combined time- and criterion-based approach is recommended, with effusion management incorporated into the plan. Rehabilitation duration varies by tear type—vertical tears typically require at least 4 months, while complex, radial, root avulsions (where the meniscus detaches from its tibial insertion), or horizontal tears may need 6–9 months of structured rehab (Grade D). Agreement: Mean 8.3 ± 1.59, Median 8 (5–9), Relative agreement.
Tear-Specific Rehabilitation Progression
The location and stability of the tear significantly influence rehab progression. Vertical longitudinal tears often permit full weight-bearing (FWB) with restricted ROM for 6 weeks, whereas complex, horizontal, radial, and root repairs typically require 4–6 weeks of limited weight-bearing and ROM restrictions (Grade C). Ramp lesions, frequently associated with ACL injuries, follow rehab protocols driven by the primary procedure (Grade C).
Unlike partial meniscectomy, which relies on milestones alone, meniscal repair rehab must balance both time-based healing phases and functional criteria: effusion, ROM, quadriceps strength, neuromuscular control (Grade D). Agreement: Mean 7.2 ± 1.96, Median 8 (5–9), Relative agreement.
Exercise Restrictions
Certain movements should be avoided to protect healing tissue. Deep squats, jumping, and rotational knee stresses are contraindicated for at least 4 months. For vertical longitudinal tears, controlled progression is advised:
- Weeks 4–8: Mini squats up to 30° flexion
- Weeks 8–12: Progress to 45° flexion
- Weeks 13–16: Advance to 60–90° flexion (Grade D).
Agreement: Mean 7.6 ± 1.34, Median 8 (5–9), Relative agreement.
Medial vs. Lateral Repairs
Rehab protocols are similar for medial and lateral repairs, with tear type (e.g., radial, root, vertical) being the primary factor influencing progression rather than meniscal laterality (Grade C). Agreement: Mean 7.8 ± 1.70, Median 8 (5–9), Relative agreement.
Rehabilitation Phases & Criteria
Post-surgery meniscus rehabilitation should be structured into protective, restorative, and return-to-activity phases, with clear benchmarks for progression:
- Restorative phase: Initiated once the patient achieves near-full passive ROM, minimal effusion, and quadriceps neuromuscular control.
- Return-to-activity phase: Requires full active ROM, ≥80% strength compared to the contralateral limb, and stable single-leg dynamic control.Strength should be objectively assessed at each phase using isokinetic or handheld dynamometry (Grade D).
Agreement: Mean 7.9 ± 1.44, Median 8 (5–9), Relative agreement.
Concurrent ACL Reconstruction
When meniscal repair is performed with ACL reconstruction, rehab follows similar principles but may delay return to sport (RTS) due to ACL recovery timelines. Most stable vertical tears do not alter standard ACL rehab, though repairs requiring weight-bearing or ROM restrictions may modify the protocol (Grade C).
Post-Operative Precautions
- Weight-bearing: Varies by tear type—some repairs require partial weight-bearing (PWB) or non-weight-bearing (NWB) for 4–6 weeks, while others allow FWB immediately with crutches for gait normalization (Grade C).
- ROM restrictions: Often imposed for 4–6 weeks, depending on tear stability.
- Bracing: Use of a locked or soft brace may be indicated in certain cases, though evidence is limited (Grade C).
Agreement: Mean 8.1 ± 1.39, Median 9 (6–9), Relative agreement.
Rehabilitation After Meniscus Reconstruction (Transplantation or Scaffold)
Rehabilitation following meniscus reconstruction—whether using scaffold-based techniques (synthetic implant) or allograft transplantation (donor-derived) —follows similar principles, with no significant differences in protocol between the two approaches (Grade D).
The process should integrate both time-based healing phases and criterion-based progression, recognizing that recovery often extends beyond 12 months before return to sport (RTS) is considered. Agreement: Mean 7.6 ± 1.82, Median 8 (5–9), Relative agreement.
The recommended approach combines time-based and criterion-based milestones, structured into three phases:
- Protective phase (early): Non-weight-bearing (NWB) for 6 weeks. (Grade C)
- Restorative phase (intermediate): Gradual progression to full weight-bearing (FWB) by 8 weeks. (Grade C). Agreement for both statements: Mean 8.1 ± 1.46, Median 9
- Return-to-sport (RTS): Not before 12 months (Grade D). Agreement: Mean 8.4, Median 9 (7–9), Strong agreement
Notably, these protocols apply equally to both medial and lateral meniscus reconstructions (Grade D). Agreement: Mean 7.9 ± 1.00, Median 8 (6–9), Relative agreement.
Weight-bearing progression requires strict caution, as premature loading elevates graft extrusion risk. Current evidence supports maintaining non-weight-bearing (NWB) status for the initial 6 postoperative weeks, followed by gradual weight-bearing limited exclusively to knee extension exercises (Grade C).Agreement: Mean 8.1 ± 1.46, Median 9 (7–9), Strong agreement.
Concurrently, range of motion should be restricted to 90 degrees of flexion during the NWB period, though these parameters may be modified based on concomitant procedures (Grade D) Agreement: Mean 8.1 ± 1.21, Median 8 (6–9), Relative agreement.
Regarding bracing, the consensus found insufficient evidence to recommend routine use, leaving this decision to surgeon preference and case-specific considerations (Grade D). Agreement: Mean 8.3 ± 1.11, Median 9 (6–9), Relative agreement.
Questions and thoughts
The current evidence guiding post-surgery meniscus rehabilitation—whether repair, reconstruction, or transplantation—remains limited, with most recommendations relying on expert consensus rather than high-level research. While this consensus provides a structured framework, it also highlights gaps in our understanding.
The consensus statements, though not always evidence-backed, offer valuable clinical direction by synthesizing expert insights. Their high agreement scores (e.g., median 8-9/9 for key recommendations) suggest pragmatic utility, even as they underscore the need for further research. For example:
- Early-phase rehab (e.g., weight-bearing restrictions, ROM limits) is relatively well-defined, reflecting broad clinical alignment.
- Later stages, especially RTS, lack specificity due to patient diversity in goals, sports demands, and healing trajectories.
The consensus highlights the efficacy of neuromuscular electrical stimulation (NMES) in addressing post-operative quadriceps inhibition following meniscus surgery. Emerging research suggests blood flow restriction (BFR) therapy may offer comparable benefits, presenting a promising alternative for post-surgery meniscus rehabilitation. For a comprehensive analysis of these modalities, we recommend this article.
The Challenge of Return to Sport
RTS protocols are particularly nebulous. While timeframes (e.g., 4–12 months) are proposed, criterion-based milestones (strength, neuromuscular control, sport-specific testing) are inconsistently applied. This ambiguity calls for:
- Better Assessment Tools: Validated questionnaires like KOOS and functional tests are a start, but they may not capture sport-specific readiness.
- Creative Problem-Solving: Therapists must ask: What does this sport demand? How can we bridge the gap between clinical recovery and dynamic performance?
-
- Example: A soccer player post-lateral meniscus repair might need progressive drills emphasizing cutting, pivoting, and eccentric loading—tasks not addressed by generic protocols
-
- Embracing Uncertainty: Rehabilitation must prepare patients for the unpredictability of real-world activities. This requires graded exposure to variability (e.g., uneven surfaces, reactive movements) to build tissue resilience and confidence.
Moving Forward: Research and Reflection
The upcoming second consensus review aims to delve deeper into these questions. Until then, therapists can:
- Advocate for Standardization: Use existing criteria (e.g., ≥80% limb symmetry, effusion-free joint) while pushing for sport-specific benchmarks.
- Document Outcomes: Share case data to build an evidence base for what works (or fails) in complex RTS scenarios.
- Focus on Patient-Centered Creativity: Beyond protocols, rehab should adapt to the individual’s physical and psychological readiness, blending science with clinical intuition.
In essence, while the consensus provides a scaffold, it’s up to clinicians to build the bridge between recovery and full function—one patient at a time.
Talk nerdy to me
This post-surgery meniscus rehabilitation stands out for its rigorous approach to minimizing biases while synthesizing clinical expertise. The process actively addressed two key methodological pitfalls:
To minimize selection bias (the distortion that occurs when non-representative samples are selected), the consensus employed strict selection criteria, assembling a panel of over 100 specialists—including orthopedic surgeons, physicians, and physical therapists—from across the United States and Europe. The process further separated the steering group (question development) from the rating group (evidence evaluation), preventing dominance by any single clinical perspective or regional practice. This structure ensured diverse viewpoints were represented rather than only including experts who might share similar biases.
Confirmation bias (the tendency to favor information confirming preexisting beliefs) was systematically addressed through three key mechanisms: (1) independent literature reviews conducted by a dedicated team using predefined search strategies, (2) multiple rounds of structured debate requiring justification of all ratings, and (3) transparent archiving of all supporting and contradictory evidence. This forced experts to engage with challenging perspectives rather than selectively referencing data supporting their assumptions.
When interpreting these consensus statements, it’s important to understand what this methodology does and doesn’t guarantee. The high agreement scores (median 8-9/9 for many recommendations) indicate strong clinical alignment among experts, but don’t equate to high-level evidence. They represent the field’s current best judgment in areas where rigorous studies are lacking. The transparent process means we can see exactly how conclusions were reached but can’t compensate for gaps in the underlying research.
This represents the gold standard for consensus development when definitive evidence is lacking. It provides a trustworthy clinical framework while clearly identifying where more research is needed – especially valuable for complex rehabilitation decisions requiring individualized judgment. The methodology’s strength lies not in eliminating all uncertainty, but in systematically minimizing bias while mapping the boundaries of current knowledge.
Take-home messages
Partial Meniscectomy:
- Immediate full weight-bearing and full range of motion as tolerated (Grade C)
- Monitor for effusions in high-risk patients (elderly, high BMI) which may require temporary assistive devices (Grade D)
- Lateral meniscectomies may demonstrate slower recovery with higher risk of persistent swelling (Grade D)
- Progress based on functional milestones rather than strict timelines, typically 4 to 12 weeks (Grade B)
Meniscus Repair:
- Vertical tears: Permit full weight-bearing with range of motion restrictions for 6 weeks (Grade C)
- Complex tears (root, radial, horizontal): Maintain non-weight-bearing status for 4 to 6 weeks with protected range of motion (Grade C)
- Avoid deep squats, jumping, and pivoting movements for minimum 4 months (Grade D)
- When combined with ACL reconstruction: Follow ACL protocol while respecting meniscus precautions
Meniscus Reconstruction (Transplant/Scaffold):
- Strict non-weight-bearing for 6 weeks with range of motion limited to 90 degrees initially (Grade C/D)
- Return to sport typically deferred until at least 12 months post-op (Grade D)
Essential Clinical Considerations:
- Early protection is crucial for repairs/reconstructions versus accelerated functional recovery in meniscectomies
- Base progression on objective milestones: resolution of effusion, restored range of motion, adequate strength recovery
- Refer back to surgeon for: mechanical symptoms, persistent swelling, or failure to achieve expected milestones
- These protocols provide structure, but always individualize progression based on each patient’s healing response
The Physiotutors clinical guide provides evidence-informed strategies for optimizing assessment and intervention of meniscal pathologies.
Reference
THE ROLE OF THE VMO & QUADS IN PFP
Watch this FREE 2-PART VIDEO LECTURE by knee pain expert Claire Robertson who dissects the literature on the topic and how it impacts clinical practice.
