Research
Diagnosis & Imaging
February 26, 2026
Prevalence of Incidental Rotator Cuff Abnormalities and Implications for Routine Shoulder Imaging

Introduksjon
By now, many clinicians are well aware that MRI-observed lesions are not always correlated with pain. Already in 1994, Jensen et al. demonstrated that the lumbar spine of asymptomatic individuals frequently shows disc bulges and protrusions. This was later confirmed by Brinjikji et al. 2015. In 1998, Matsumoto et al. were able to show that asymptomatic subjects also had high rates of cervical spine disc abnormalities. In 2008, similar findings emerged for the knee when Englund et al. pointed to a high number of incidental meniscal findings on knee MRI in middle-aged and elderly persons. Later on, the study by Okada et al. (2019) concluded after a 10-year follow-up that, in the thoracic spine, disc changes were also common in people without pain. These findings led to an increased understanding of the influence of aging and the development of age-related changes in the spine.
A majority of these studies have been observed in the spine. A lot less research has been conducted in other body regions. For example, similar studies have been conducted on this topic in the shoulder, but they were methodologically weaker, resulting in less certainty. Therefore, the current study wanted to determine the prevalence of incidental rotator cuff abnormalities in a general sample of asymptomatic subjects, taking into account the need for robust evidence.
Metoder
This cross-sectional observational study was conducted in Finland from 2023 to 2024 and included participants from the Health 2000 survey, which is a nationally representative longitudinal study conducted in Finland since 2000. The cohort of people is longitudinally followed, and their data serve as an important epidemiological resource.
The participants included in this study were drawn from the Health 2000 survey and had to be a maximum of 75 years old at the time of inclusion. It was required that these participants be able to access one of five university hospitals for obtaining Magnetic Resonance Imaging (MRI).
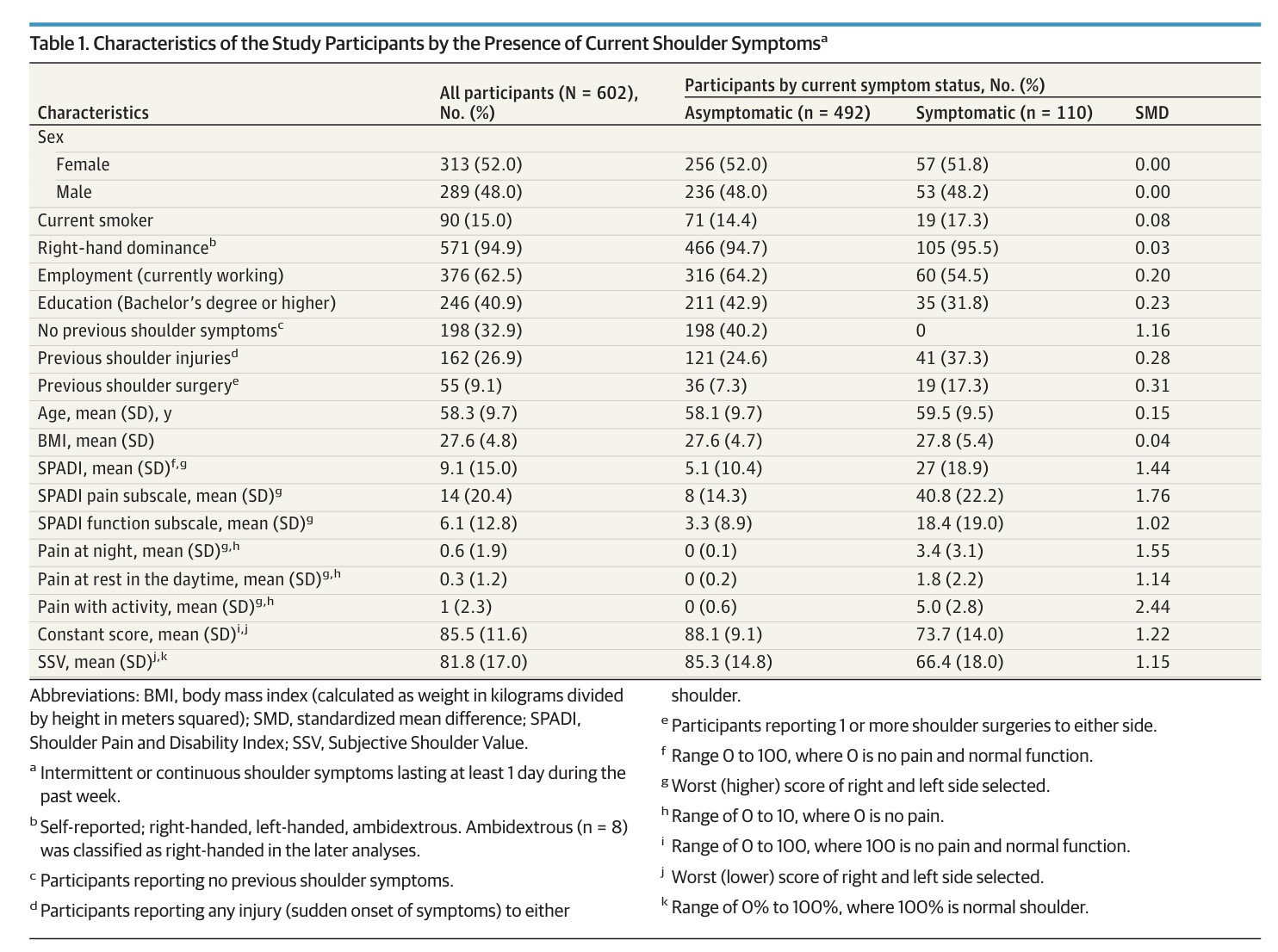
Participants who consented to participate in this study underwent a standardized assessment of their medical history and shoulder symptoms, both via questionnaires and a structured interview. They were asked if they had experienced shoulder symptoms lasting for more than 24 hours (either persistent or intermittent) during the past week. Based on their response, the participants were classified as asymptomatic or symptomatic. The history of shoulder symptoms in the past was obtained from all participants.
Further, assessment of shoulder pain and function was done using the Shoulder Pain and Disability Index (SPADI), Constant Murley Shoulder score, and the Subjective Shoulder Value. The latter is a question asking the participant to rate their overall shoulder function from 0 to 100%, with 0 representing “No function” and 100 representing a fully functional (normal) shoulder.
Next, they underwent a clinical examination by a shoulder and elbow surgeon. Only thereafter were the MRI images obtained. These images were rated independently by 2 of 3 radiologists, using standardized assessment forms. These radiologists were blinded to the demographic information and the clinical examinations.
Each of the four rotator cuff tendons (supraspinatus, infraspinatus, subscapularis, and teres minor) was evaluated separately using the Zlatkin classification.
- The criteria for classifying each tendon’s status were:
- Tendinopathy: Indicated by a signal increase and/or inhomogeneity on fluid-sensitive MRI sequences.
- Partial -Thickness Tear (PTT): Interpreted as a fluid-filled defect of the tendon tissue extending to either surface or the tendon insertion on more than two consecutive images.
- Full-Thickness Tear (FTT): Required a defect that extended to both surfaces of the tendon, thereby connecting the subacromial space and the glenohumeral joint.
- Normal: No abnormalities were observed.
- Overall Shoulder Classification:
- The MRI finding for each shoulder was classified based on the most severe abnormality detected in any of the four individual rotator cuff tendons.
- An ordinal severity scale was used to determine the most severe finding:
- Full-Thickness Tear (FTT) (Most Severe)
- Partial-Thickness Tear (PTT)
- Tendinopati
- Normal Tendon
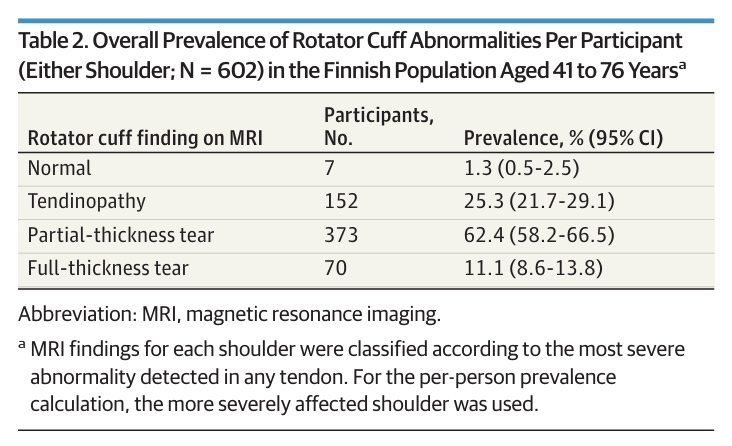
For the purpose of calculating the per-person prevalence of rotator cuff abnormalities in the study’s results, the shoulder with the more severe abnormality was used.
To conclude the evaluation of the MRI, abnormalities of the glenohumeral and acromioclavicular joints, as well as the long head of the biceps tendon, were also investigated.
Resultater
A total of 602 participants were included in the study and underwent clinical shoulder examination and a bilateral MRI. The sample was evenly distributed between males and females. 110 participants (18%) reported current shoulder symptoms, and in the asymptomatic group, 294 (60%) reported a previous history of shoulder symptoms.
Of the 602 participants included, MRI revealed rotator cuff abnormalities in 595 (98.7%) people. Of these, 25% had tendinopathy, 62% had partial-thickness tears, and 11% had full-thickness tears.
Abnormalities were most prevalent in the supraspinatus tendon (590 – 98%), followed by the infraspinatus (517 – 86%), subscapularis (499 – 83%), and the teres minor (68 – 11%) tendons. The presence of a partial or full-thickness tear was more common in the dominant shoulder. Of the 70 participants with full-thickness tears, 26 (37%) had bilateral tears.
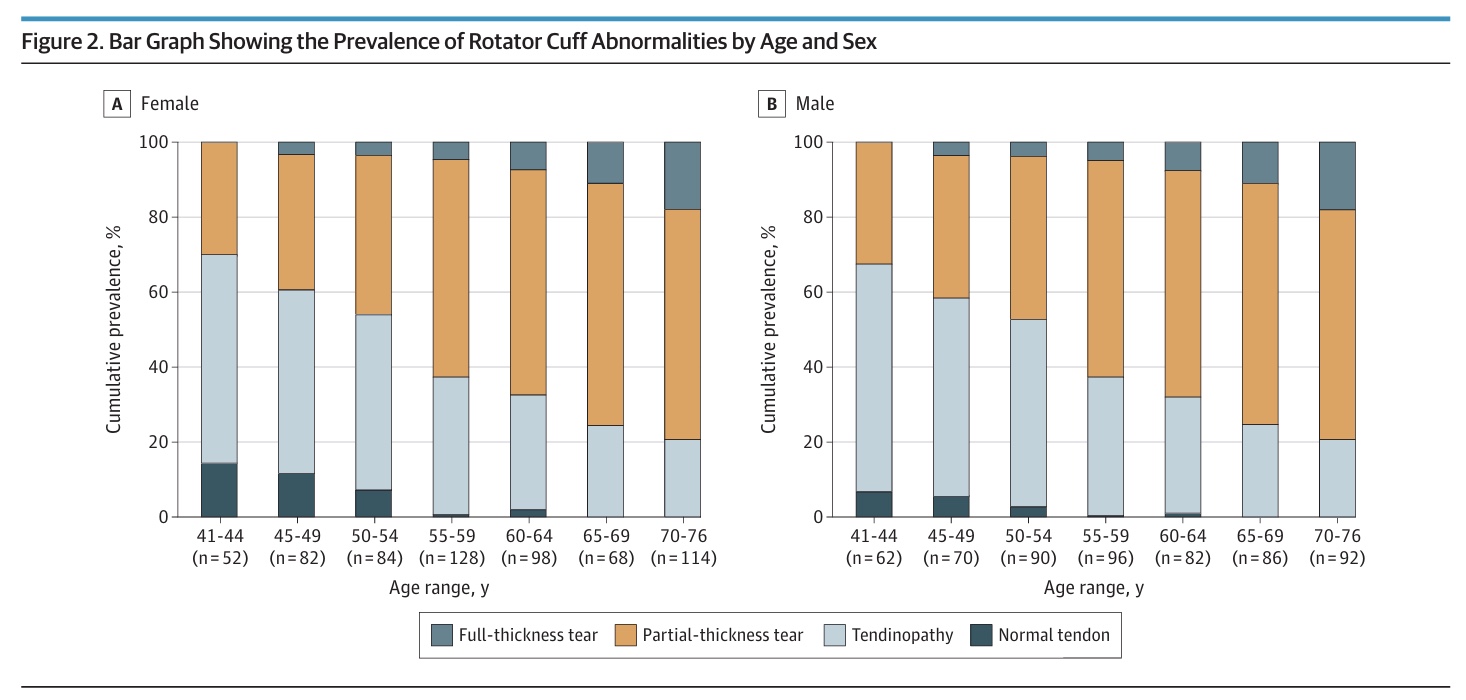
The authors were able to demonstrate a clear age-related progression of the prevalence of rotator cuff abnormalities. Younger patients had milder findings, while older participants had more advanced abnormalities (partial- or full-thickness tears). In younger individuals, tendinopathy was more common, while partial- or full-thickness tears became more prevalent in the age group 55 years and older.
When the population prevalence of rotator cuff abnormalities in symptomatic and asymptomatic shoulders was investigated, the authors found that of the 1204 shoulders, 1076 (90.6%) were asymptomatic and 128 (10.4%) were symptomatic. Rotator cuff abnormalities were observed in 96% of asymptomatic shoulders and in 98% of symptomatic shoulders. This led to a prevalence difference of 1.8% (95% CI -2.9% to 4.7%). The prevalence of tendinopathy findings and partial-thickness tears was similar in symptomatic and asymptomatic individuals. Full-thickness tears were more common in symptomatic shoulders (14.6%) compared to asymptomatic shoulders (6.5%), leading to a significant prevalence difference of 8.1% (95% CI 1.8% to 15.1%).
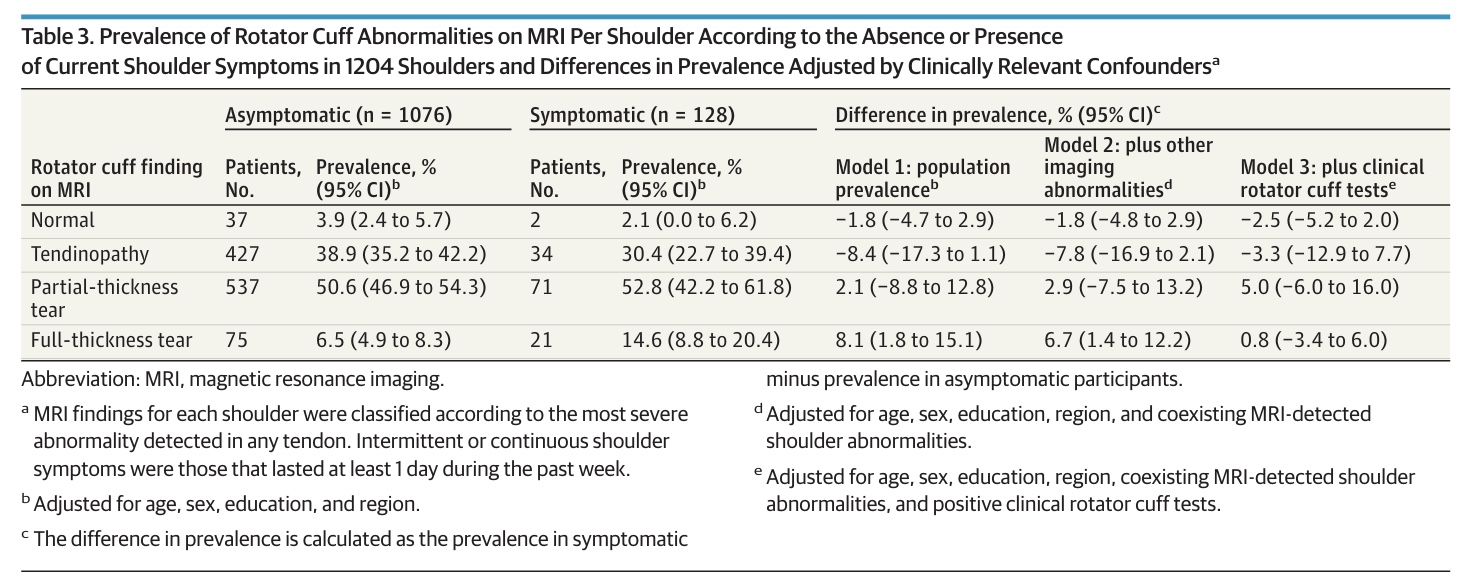
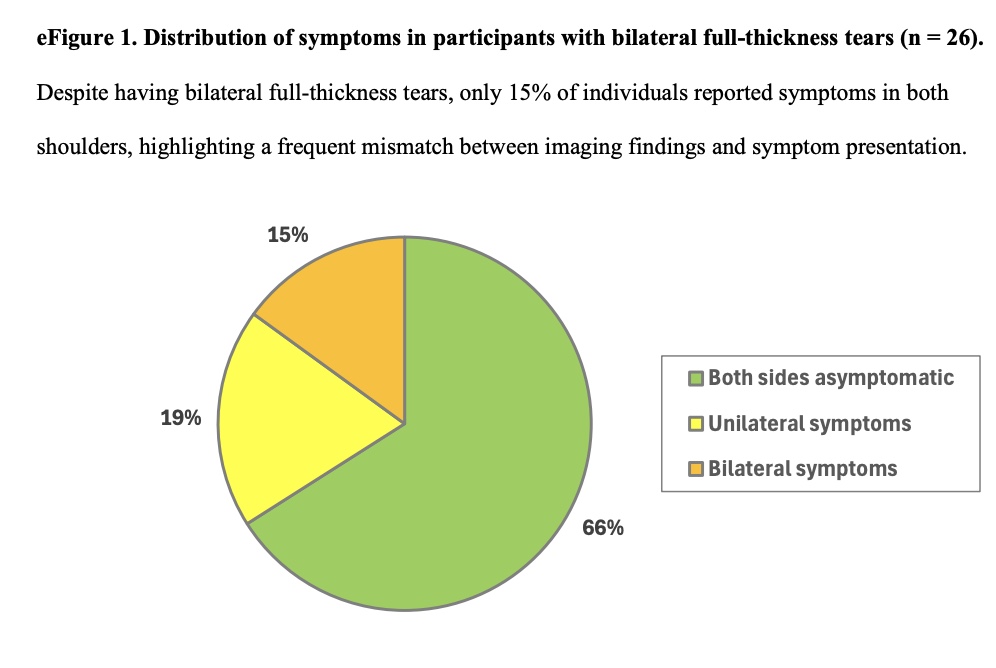
Ninety-six full-thickness tears were counted in 70 people. Of them, 26 participants had bilateral full-thickness tears. Of those 96 full-thickness tears, 75 (78%) were identified in the asymptomatic shoulders. Of the 26 participants with bilateral full-thickness tears, 17 (66%) reported no symptoms in either shoulder, and 5 (19%) reported symptoms in only 1 shoulder.
Importantly, after adjusting for the 2 clinically relevant potential confounders (the presence of imaging abnormalities in other shoulder structures and positive clinical rotator cuff tests), the difference in full-thickness prevalence between asymptomatic and symptomatic participants was no longer observed (prevalence difference 0.8% with 95% CI -3.4% to 6.0%). Also, accounting for tear size did not change this result.
In the participants with a prior history of shoulder symptoms (418) and without (658), the prevalence of full-thickness tears was more frequent in those with a prior history.
Spørsmål og tanker
In the text, an apparent contradiction appears when the authors state: “Full-thickness tears were more common in symptomatic shoulders (14.6%) than in asymptomatic shoulders (6.5%). Importantly, 78% (75 of 96) of the full-thickness tears observed were identified in asymptomatic shoulders.” It is, however, not contradictory:
- The asymptomatic group (1,076 shoulders) is approximately 8.4 times larger than the symptomatic group (128 shoulders). Because the sheer size of the asymptomatic group is so large, even a low prevalence rate (6.5%) yields a higher absolute number of full-thickness tears than the higher prevalence rate (14.6%) in the much smaller symptomatic group.
- This second statement is the study’s central finding: While full-thickness tears are more likely to be found if a patient has pain, the vast majority of full-thickness tears you might find on an MRI in the general population are completely incidental and not causing symptoms.
- Total full-thickness tears found: 96
- absolute number of asymptomatic full-thickness tears: 75
- absolute number of symptomatic full-thickness tears: 21
- Proportion: 75/96 = approximately 78%
Looking at the first statement, if you were to randomly select 100 people with pain and 100 people without pain, you would find twice as many full-thickness tears in the group with pain. This looks like full-thickness tears are indeed associated with symptoms. BUT, the absolute number reveals that 78% of the full-thickness tears observed were identified in asymptomatic shoulders. When you receive an MRI report showing a full-thickness tear, you must ask yourself: “In the general population, how often does this finding exist without causing symptoms?” The answer is “most of the time”, since 78% of all full-thickness tears in this study were silent.
From a realistic perspective, it is not surprising that many people show incidental rotator cuff abnormalities on MRI. Just think of this: we all learned from textbook-perfect anatomy, but none of us learned how increasing age changes the “perfect” anatomy. Labeling changes seen on MRI as tears, defects, or pathology is not always reliable, as evidenced by the high prevalence of incidental rotator cuff abnormalities in this asymptomatic general population sample. Just think of this example:
You study a group of people aged 41 to 76. Just like a rotator cuff tear, a gray hair is a sign of normal, age-related degeneration. It’s expected and almost guaranteed as you get older. The appearance of a gray hair is a visible sign that your body is aging. It does not mean your hair is “damaged,” or that you should worry every time you see one. It is simply a change from the “perfect” picture of a head of hair from your 20s. The same thing that happens to your hair is happening inside your shoulder. The study shows that in a 50-year-old person, the chance that their MRI shows some kind of rotator cuff abnormality is almost 99%. It’s a structural change that perfectly explains that your body is getting older, but it does not automatically mean:
It is the source of your pain, your shoulder is “damaged” or “broken.”, or you need to stop using your arm. The finding of a tear on an MRI is, in the vast majority of cases, an incidental finding
When the gray hair is not the problem, but the scalp under the hair is severely irritated, bleeding, or infected. The color of the hair is irrelevant; the underlying skin problem is the concern.
- The full-thickness tear is not the problem, but the function of the shoulder is severely impaired. The patient has concordant, positive clinical tests (e.g., severe weakness on specific movements, or intense pain when the tendon is loaded). Action: The tear is now clinically relevant because it aligns with a functional problem you can test.
Of course, this is true for slow-occurring findings. When you have a sudden specific high-energy trauma like a fall, this can, of course, lead to an acute traumatic tear. But that was not what this study was about. In short, your attention should shift from the picture (the MRI) to the patient’s performance (the clinical exam). A tear without pain is a gray hair. A tear that causes profound weakness and pain during movement is a clinically significant problem.
Tendinopathy was more common in younger people, and with advancing age, the prevalence of tendonopathies became less, while on the other hand, the prevalence of partial-thickness tears rose. Is tendinopathy a precursor for worse outcomes in the future? That is something we cannot say looking at this study, since it used a cross-sectional design, where only one snapshot in time was analyzed, and people were not followed longitudinally. But this may be a relevant question for a follow-up study, in my opinion.
Snakk nerdete til meg
What really stood out in this study was the adjustment for confounding variables. By building three hierarchical models, the study adjusts for demographic factors (such as age) and other imaging abnormalities (since pain can arise from sources beyond the rotator cuff), as well as clinical tests, leading to significantly more certainty in the evidence compared to earlier methodologically weaker studies.
How should we interpret these findings? As a physiotherapist, you should always be able to relate the images to the patient’s complaint, and thereby, you should already be aware of the risk of an abnormality. For example, in a 50-year-old person from the general population, the chance that there is some rotator cuff abnormality is almost 99% (595 of 602 shoulders of the general population aged 41-76 years, leading to 98.7%). This is simply normal aging.
When a patient has pain, you cannot simply blame the tear on the MRI. The study shows that the difference in severe tears between people with and without pain disappears as soon as you include the findings from your own clinical examination (such as pain with specific movements). In other words: Your clinical exam is more important than the picture.” The same is true for the presence of abnormalities in other shoulder structures. The fact that the full-thickness tears difference became non-significant after adjustment strongly suggests that the full-thickness initial association with pain was actually a confounding effect.
- Those with full-thickness tears who also reported pain were more likely to have other structural problems (like acromioclavicular joint osteoarthritis, glenohumeral osteoarthritis, or superior labrum abnormalities) than those who had full-thickness tears but no pain. So, the pain was likely driven by these other structures (or a combination thereof), and the full-thickness tear was merely a co-existing, incidental finding. The full-thickness tears were “guilty by association” until the researchers statistically isolated the real culprits.
- The same was true for the positive clinical rotator cuff tests. A patient with a full-thickness tear who had pain was more likely to have a positive finding on a clinical test than a patient with a full-thickness tear who had no pain. This means that the clinical exam is a better predictor of the current pain than the imaging finding.
Ta med hjem meldinger
Almost every person over the age of 40 has some form of rotator cuff abnormality or tear. In a 50-year-old, the chance that something shows up on the MRI is almost 99%. This is simply a normal, age-related change and not a diagnosis of disease. A rotator cuff abnormality on an MRI is, in most cases, the internal equivalent of a gray hair. It confirms your body is aging, but it does not cause pain. You only need to pay attention to the “gray hair” if the patient has concordant, positive clinical tests that indicate the function is severely compromised. A tear without pain is a gray hair; a tear with pain and weakness is a clinically significant problem. The study proved that the imaging result loses its relationship to pain once you account for the findings from your own clinical examination. Your hands, your observations, and your specific tests are a better predictor of the current pain than the picture.
Referanse
TO MYTER BRUTE OG 3 KUNNSKAPBOMBBER GRATIS
Hvilket universitet forteller deg ikke om skulderimpingementsyndrom og scapula dyskinesis og hvordan du massivt oppgraderer skulderspillet uten å betale en eneste cent!