
Research
Lumbar/SIJ
March 16, 2026
Do Illness Perceptions of Low Back Pain Influence Treatment Outcomes?

Introduksjon
Low Back Pain is a highly prevalent and recurrent musculoskeletal condition in which biological, psychological, and social factors are believed to contribute to pain and disability. Current clinical recommendations emphasize promoting patients’ self-management, particularly through education and exercise interventions. In this context, illness perceptions of low back pain may play an important role in patient outcomes, as these can influence coping strategies, emotional responses to the condition, and engagement with treatment. Emerging evidence suggests that illness perceptions may affect outcomes in individuals with low back pain. Importantly, illness representations are considered modifiable factors that could potentially be addressed through appropriate clinical management. The BetterBack Model of Care was developed as a physiotherapy-based approach for low back pain, aiming, among other objectives, to improve illness perceptions of low back pain and promote patient enablement. Therefore, the present study investigates how the implementation of this model of care influences treatment outcomes in patients with low back pain.
Metoder
Design
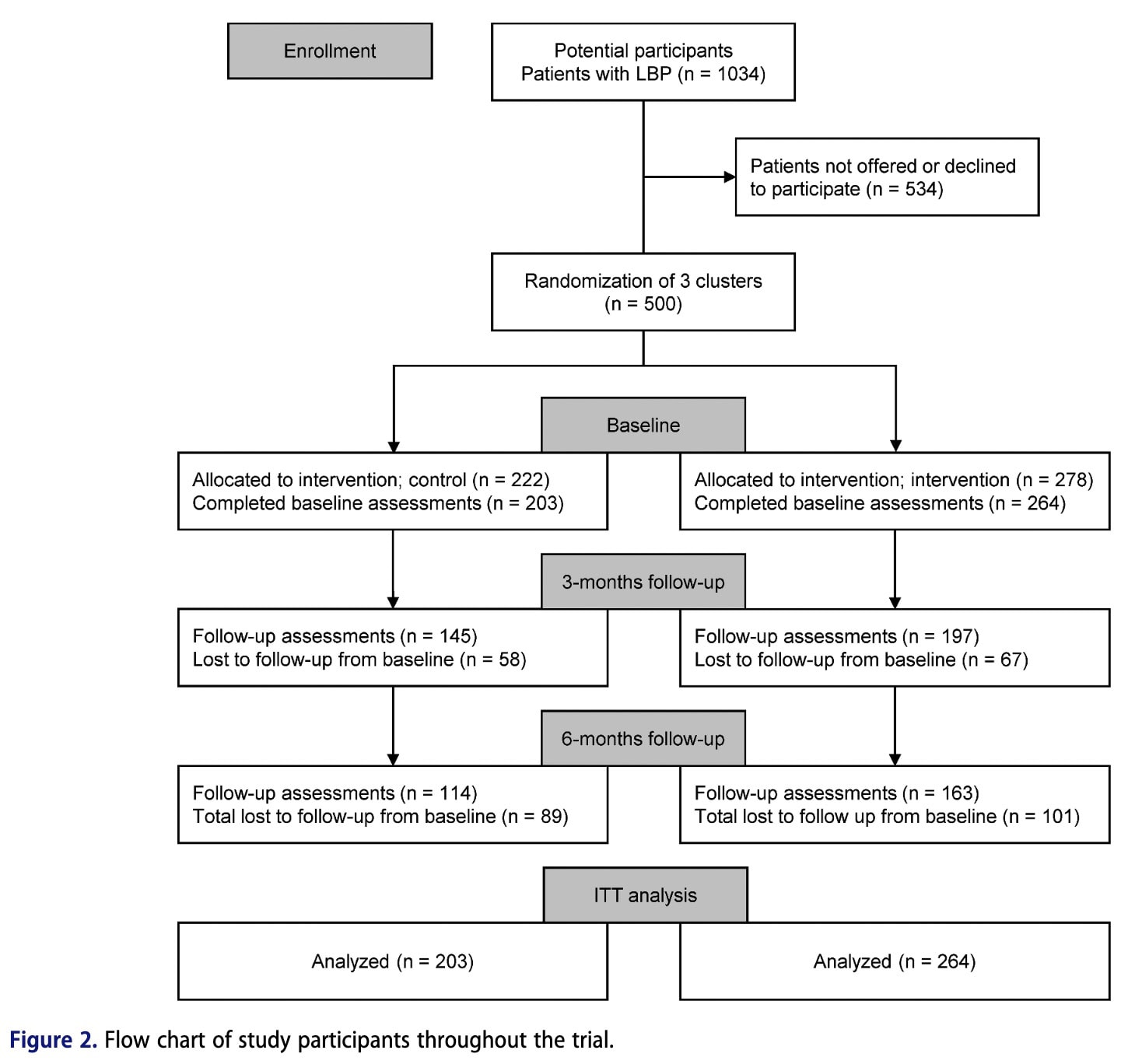
This study was a planned secondary analysis of data from a previous clinical trial. The original study was a single-blinded stepped cluster randomized controlled trial that evaluated physiotherapy care after the implementation of the BetterBack Model of Care (MoC), compared with the routine care previously provided.
Participants and setting
A total of 467 patients seeking physiotherapy care for low back pain were consecutively recruited from 15 publicly funded primary care physiotherapy clinics. Clinics were organized into three clusters based on geographical and organizational structure. The study used a stepped cluster randomized design, meaning patients were not individually randomized but received routine care or the BetterBack Model of Care (MoC) depending on the clinic cluster and the time during the trial when they sought care. Physiotherapists in the first cluster were trained in the BetterBack MoC at the beginning of the study and delivered the intervention throughout the trial. Physiotherapists in the second cluster initially provided routine care and later received training mid-trial, after which they implemented the BetterBack MoC. Physiotherapists in the third cluster delivered routine care for the entire study period and served as the control group.
Secondary analyses were also performed based on the actual care received, with participants categorized according to whether they received guideline-adherent or non-adherent care, regardless of their original group allocation. Guideline-adherent care followed five key recommendations from the locally adapted clinical guidelines for Low Back Pain, including avoiding unnecessary imaging and specialist referral, providing patient education and exercise, and avoiding non–evidence-based treatments
The BetterBack Model of Care was adapted to the Swedish healthcare context and included several support tools such as clinical reasoning and assessment tools, patient-centered care pathways, patient education materials on low back pain and self-management, group education resources, and functional restoration program resources. The aim was to promote physiotherapy management consistent with guideline-recommended care. Treatment duration and number of sessions were collected from medical records.
Inclusion criteria
- Age between 18 and 65 years
- Fluent in Swedish
- Seeking physiotherapy care for a first-time or recurrent episode of benign low back pain (acute, subacute, or chronic phase), with or without radiculopathy
Exclusion criteria
- Current malignancy or malignancy within the previous 5 years
- Spinal fracture
- Spinal infection
- Cauda equina syndrome
- Ankylosing spondylitis or systemic rheumatic disease
- Spinal surgery within the past 2 years
- Current pregnancy or pregnancy within the previous 3 months
- Eligibility for multimodal/multiprofessional rehabilitation for complex long-standing pain
- Severe psychiatric disorder
Mediation analyses
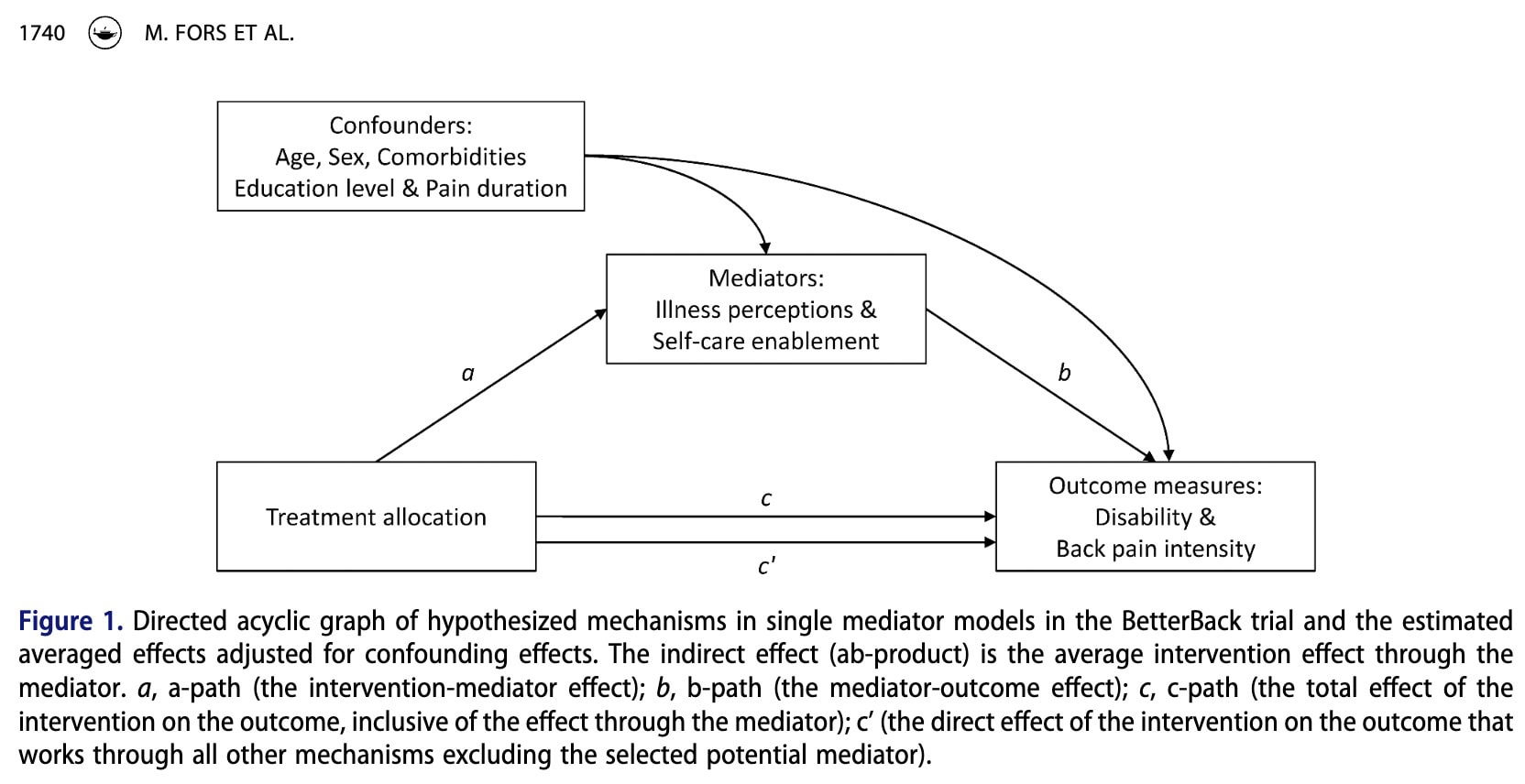
When mediators (Illness perception and Self-care enablement) and outcomes (Disability and Pain) are continuous variables, mediation analysis can be used to break down the total effect of an intervention into different pathways (Figure 1).
The c-path represents the total effect of the intervention on the outcome, including the effect that occurs through the mediator.
The a-path represents the effect of the intervention on the potential mediator. In other words, it shows whether the intervention changes the mediator.
The b-path represents the relationship between the mediator and the outcome. It shows whether changes in the mediator influence the outcome.
The indirect effect (ab) represents the part of the intervention’s effect that works through the mediator. It is calculated by multiplying the a-path and the b-path.
The direct effect (c′) represents the part of the intervention’s effect that influences the outcome through other mechanisms, excluding the mediator being studied
The indirect effect can also be interpreted using two theoretical perspectives. Action theory focuses on whether the intervention successfully changes the mediator (a-path). Conceptual theory focuses on whether the mediator actually influences the outcome (b-path).
If the a-path is strong, it means the intervention effectively targets the mediator. If the b-path is strong, it suggests that the mediator is an important factor influencing the outcome.
Patient-reported outcome measures
Patient-reported outcome measures (PROMs) were collected at baseline by the treating physiotherapist during the first visit. Follow-up data at 3 and 6 months were collected using postal questionnaires sent to the patients.
In this study, mediators were assessed at baseline and at the 3-month follow-up, while outcomes were measured at baseline and at the 6-month follow-up. These time points were planned to ensure the correct temporal order between treatment, mediators, and outcomes. Participant characteristics and potential confounders were assessed before treatment.
Outcomes
The primary outcomes of this secondary analysis were group differences in disability and low back pain intensity at 6 months post-baseline.
Disability was measured using the Oswestry Disability Index (ODI). Pain intensity was assessed using the Numeric Rating Scale for low back pain (NRS-LBP), which ranges from 0 (no pain) to 10 (worst pain imaginable).
Changes in ODI and NRS-LBP over 6 months are commonly recommended measures for evaluating improvements in pain and function in patients with Low Back Pain. They are part of the core outcome domains recommended for clinical trials in non-specific LBP.
Potential mediator
The study hypothesized that the BetterBack Model of Care (MoC) would reduce disability and pain by influencing two potential mediators: patients’ illness perceptions and self-care enablement.
Illness perceptions of low back pain was measured using the Brief Illness Perception Questionnaire (BIPQ), which is based on the Common-Sense Model of Self-Regulation. The questionnaire includes nine items assessing cognitive and emotional representations of illness. Eight items are scored from 0 to 10 and summed to a total score ranging from 0 to 80, where higher scores indicate a more threatening perception of the illness.
Self-care enablement was assessed using the Patient Enablement Instrument (PEI), which measures patients’ perceived ability to understand and cope with their illness. Scores range from 0 to 12, with higher scores indicating greater enablement. The PEI is a transition measure and is therefore not assessed at baseline.
Potential confounders
For mediation analyses to support causal interpretation, several assumptions must be met, including the absence of unmeasured confounders in the relationships between treatment, mediators, and outcomes.
In the main trial, randomization helped ensure that treatment groups were comparable at baseline, which likely reduced confounding in the relationships between treatment and mediators, and between treatment and outcomes. However, confounding may still exist in the relationship between the mediators and outcomes.
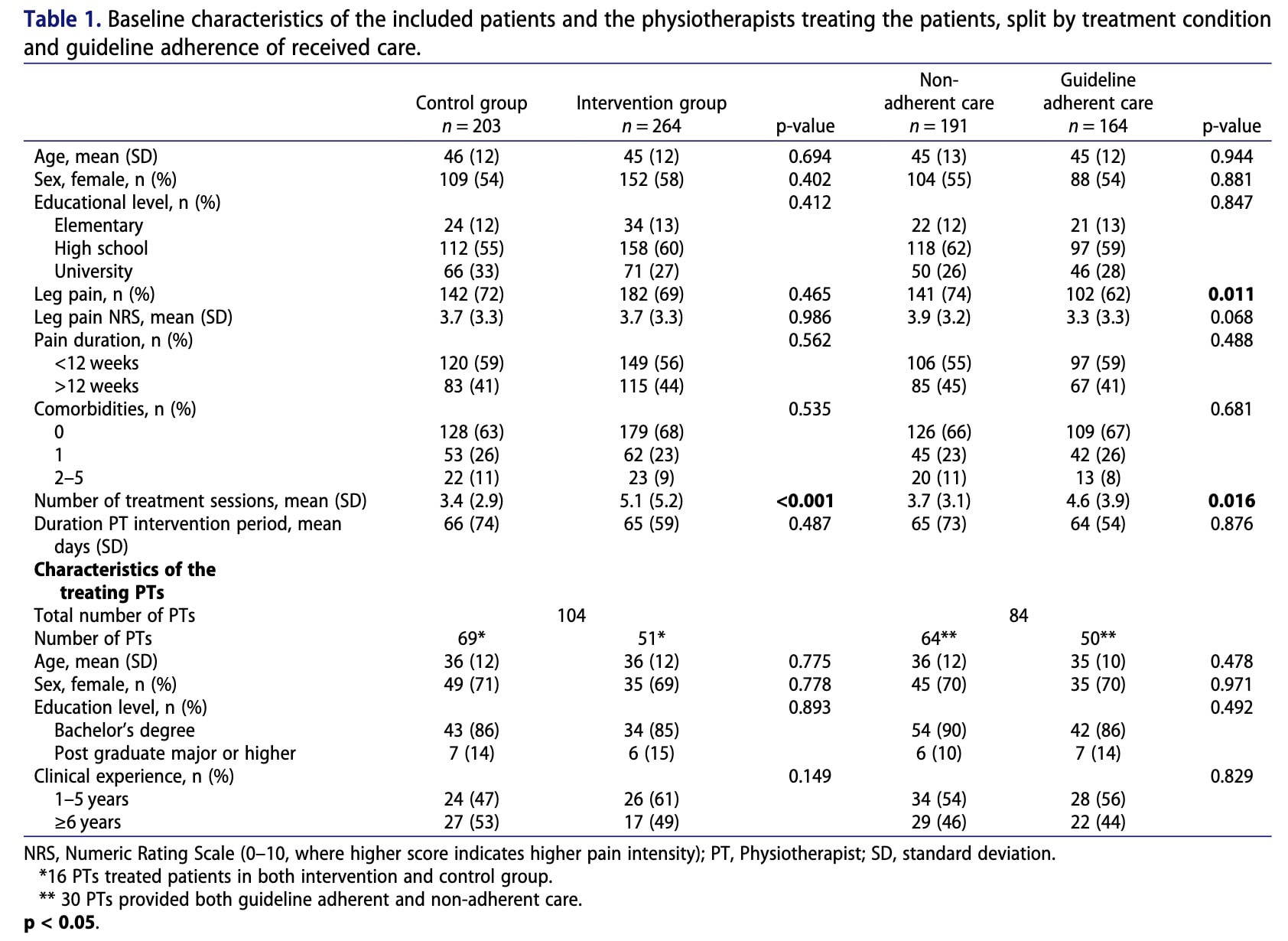
To address this, several pre-treatment covariates were considered as potential confounders based on previous research and consensus within the research group. These included age, sex, comorbidities, education level, and pain duration.
In the exploratory analysis comparing guideline-adherent care with non-adherent care, patients were not randomized. Therefore, confounding may exist in the relationships between treatment, mediators, and outcomes. In addition to patient characteristics, physiotherapist characteristics (sex, age, and clinical experience) were also considered as potential confounders.
Resultater
Baseline assessments were completed by 467 participants. Retention at 3 months was 71% in the control group and 75% in the intervention group, while retention at 6 months was 56% and 62%, respectively. The participant demographic characteristics were similar between groups. Finally, the treating physiotherapists had similar levels of clinical experience among groups.
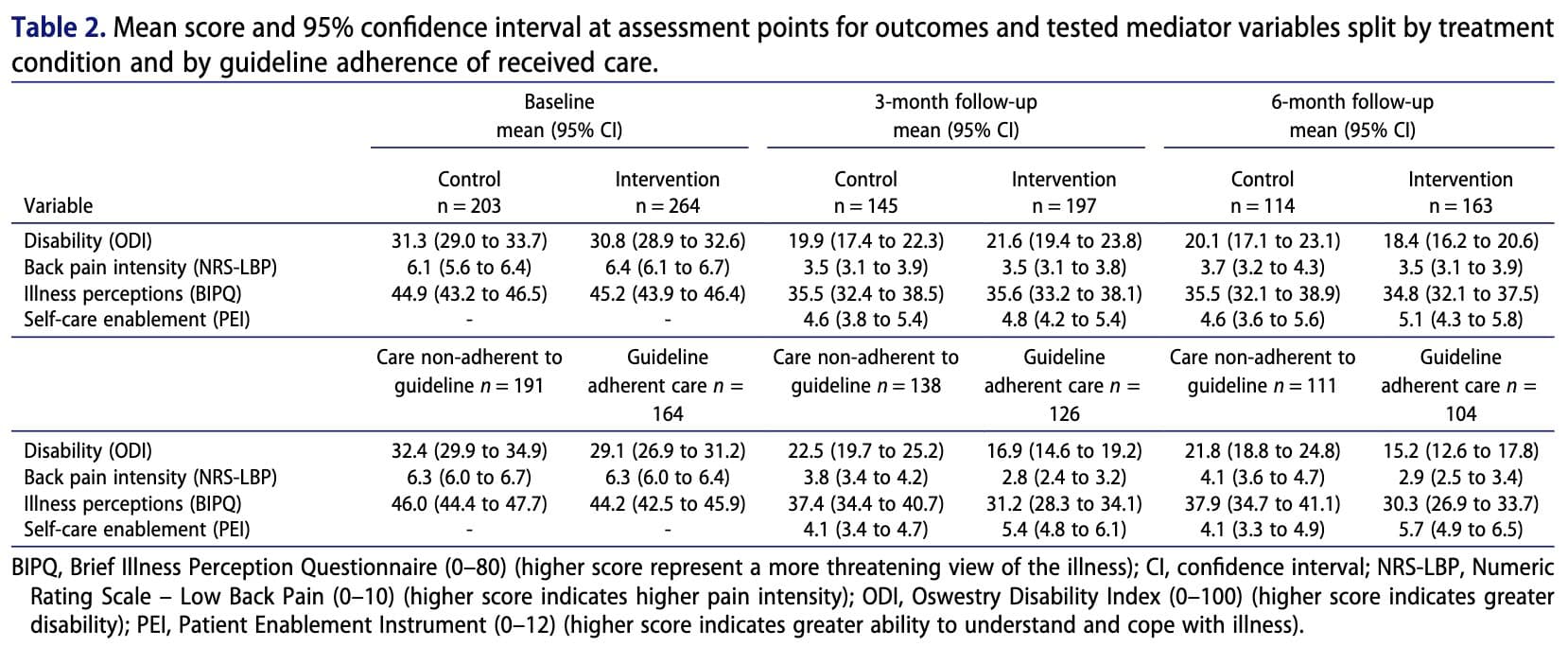
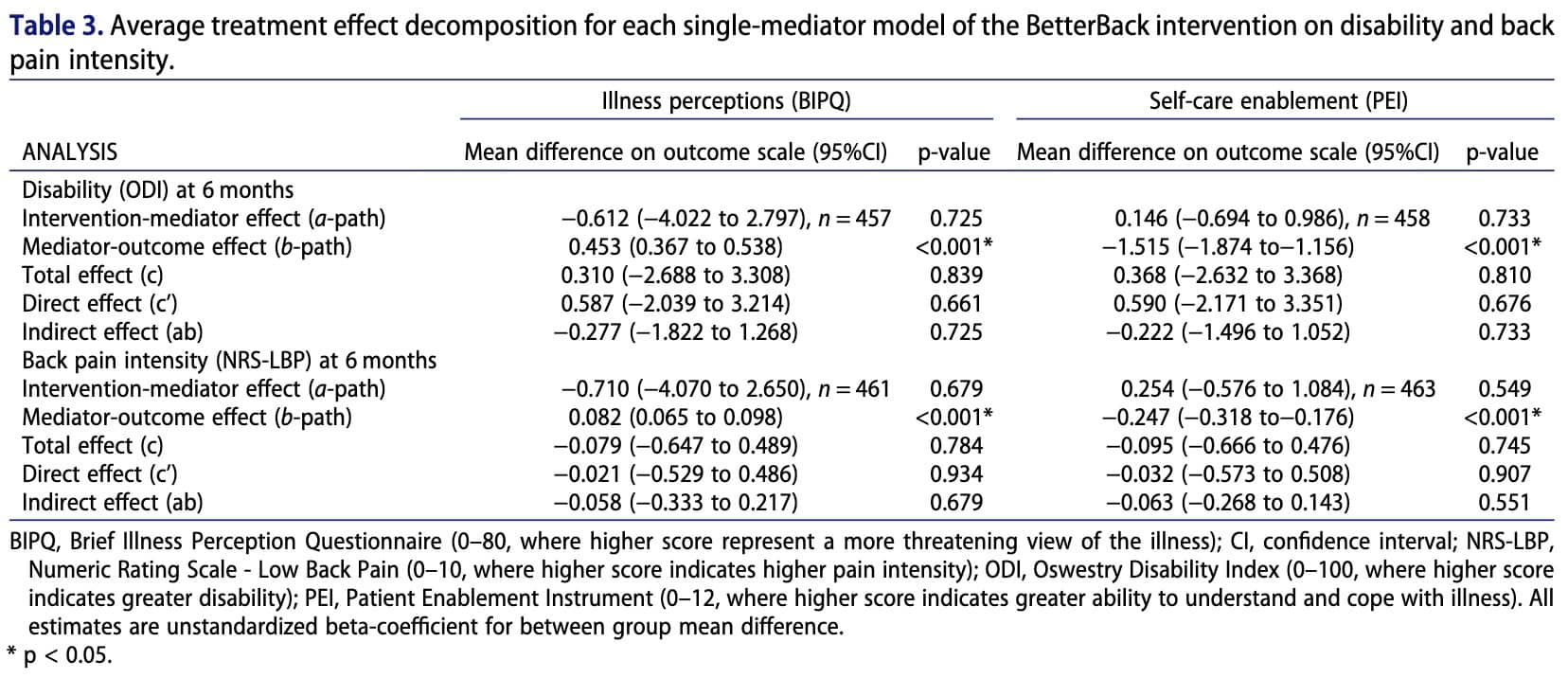
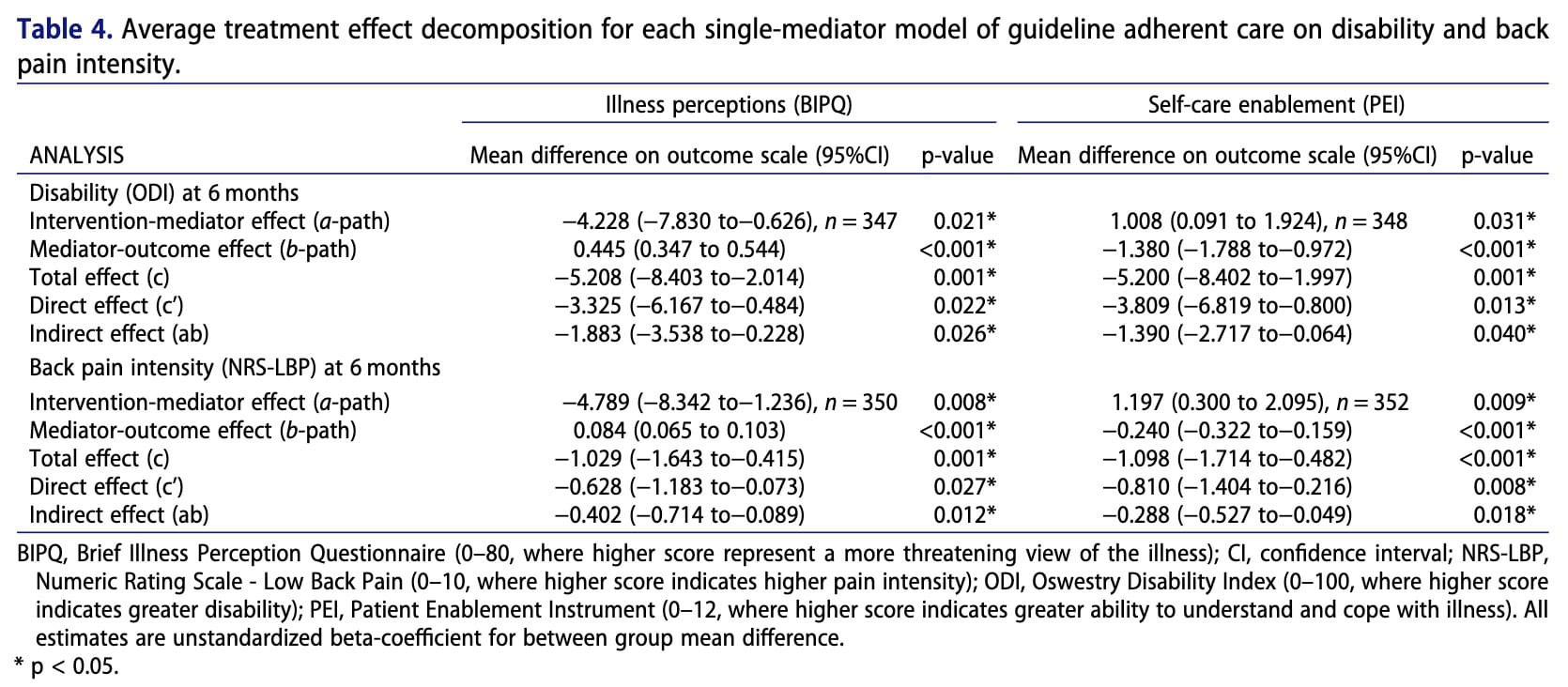
Overall, there were no significant differences between the intervention and control groups in terms of disability, back pain intensity, illness perceptions, or self-care enablement. However, the analysis showed that patients who held more maladaptive beliefs about their illness at three months tended to experience greater disability and higher pain intensity at six months. Conversely, higher self-care enablement at three months was associated with lower disability and reduced pain at six months. While the intervention itself did not directly outperform routine care, patients who received care adhering to clinical guidelines exhibited more positive illness perceptions and greater self-care enablement. These factors, in turn, were linked to better outcomes through indirect effects, suggesting that how care influences patient beliefs and self-management capacity may be important in improving long-term results.
Spørsmål og tanker
The results of the mediation analysis raise important questions regarding the mechanisms through which physiotherapy interventions may influence outcomes in patients with Low Back Pain. Although illness perceptions and self-care enablement were significantly associated with disability and pain outcomes, the BetterBack Model of Care (MoC) did not substantially modify these mediators, whereas the guideline-adherent care approach did. This suggests that while these factors appear to be relevant determinants of recovery, the strategies used in the BetterBack MoC—primarily patient education and exercise—are insufficient to meaningfully change patients’ illness perceptions of low back pain and coping strategies.
Alternative approaches may offer promising avenues. For example, Cognitive Functional Therapy (CFT) has shown encouraging results, as highlighted in a previous review, in the management of low back pain by targeting beliefs, behaviours, and movement patterns through individualized education and gradual exposure to feared movements. By reducing kinesiophobia and addressing maladaptive beliefs through experiential learning, such approaches may more effectively modify illness perceptions of low back pain.
Overall, these findings highlight the importance of continuing to explore and develop interventions specifically designed to target psychological and behavioural mediators, such as illness perceptions and self-care enablement. Future research should investigate whether interventions that more directly address these mechanisms can produce greater improvements in pain and disability outcomes.
Snakk nerdete til meg
From a methodological perspective, the study used Structural Equation Modelling (SEM) to investigate the mechanisms underlying treatment effects. This approach allows researchers to model several causal pathways simultaneously and estimate direct effects (c′ path) as well as indirect effects (ab path) through mediation analysis. In this framework, the a-path represents the effect of the intervention on the mediator, while the b-path represents the association between the mediator and the outcome.
Each pathway corresponds to a regression equation describing how changes in one variable are associated with changes in another variable. The results presented in Table 3 show that the intervention did not significantly influence the mediators (non-significant a-paths). However, the mediators were significantly associated with the outcomes (significant b-paths), indicating that these variables are related to patient outcomes but were not strongly modified by the intervention.
Another methodological consideration concerns intervention fidelity. It is important to determine whether physiotherapists in the BetterBack MoC group consistently applied the intervention protocol during consultations. If the model of care was not implemented as intended, this could have reduced the observed intervention effects and contributed to the absence of significant mediation.
According to the published protocol of the BetterBack Model of Care protocol study, physiotherapists received a two-day training program, access to an online educational platform, and a two-hour interactive workshop three months after the implementation of the program. While these measures aimed to support the adoption of the model of care, the protocol does not clearly report quantitative measures of adherence to the intervention, such as fidelity checks, consultation audits, or standardized adherence scoring.
Without systematic monitoring of treatment fidelity, it remains difficult to determine whether the intervention was delivered consistently across clinicians.
Ta med hjem meldinger
- Patient beliefs strongly influence outcomes.Negative illness perceptions of low back pain are associated with higher pain intensity and disability over time. How patients understand their condition matters for recovery.
- Self-management confidence is key.Patients who feel capable of managing their condition (higher self-care enablement) tend to report less pain and disability months later.
- Guideline-based care may shape beliefs.Patients receiving guideline-adherent care showed more positive illness perceptions and greater self-care enablement compared with those receiving non-adherent care.
- Education alone may not change beliefs enough.Traditional education and exercise programs may not sufficiently modify illness perceptions of low back pain, suggesting that more targeted psychological or behavioural strategies may be needed.
- Target beliefs as part of treatment.Approaches like psychologically informed physiotherapy, behavioural coaching, and graded exposure may help reshape patient beliefs and improve long-term outcomes.
Referanse
Hvordan ernæring kan være en avgjørende faktor for sentral sensibilisering - Videoforelesning
Se denne GRATIS videoforelesningen om Nutrition & Central Sensibilization av Europas #1 kroniske smerteforsker Jo Nijs. Hvilken matpasienter bør unngå vil nok overraske deg!
