
Research
Ankle/Foot
March 9, 2026
High-Load Exercise for Tendons: A Novel Approach Based on Biomechanical Tendon Properties

Introduksjon
This article follows last week’s publication. While the previous article explored the biological and mechanical foundations of tendon adaptation, the present paper shifts the focus toward clinical implications. Specifically, it presents a controlled clinical trial investigating high-load exercise for tendon readaptation.
To briefly revisit key concepts from the previous article, tendons are not inert structures; rather, they are biologically active tissues in which complex mechanical and cellular mechanisms interact to support regeneration. Among the key regulators involved in tendon adaptation are the transcription factors Scleraxis (Scx) and Mohawk (Mkx), which play crucial roles in type I collagen synthesis (fibrillogenesis) and tendon maturation, respectively. However, activation of these transcription factors is load-dependent.
In the context of tendon injury, altered mechanical properties can prevent adequate load transmission to the degenerative portion of the tissue. This phenomenon, known as stress shielding, occurs because the healthier, stiffer regions of the tendon absorb a disproportionate amount of the load, while the more compliant, degenerative areas remain relatively unloaded. As a result, insufficient mechanical stimulation of the injured portion contributes to scar formation and extracellular matrix disorganization.
Emerging evidence suggests that carefully designed exercise protocols—particularly those leveraging the viscoelastic properties of tendon tissue—may help overcome this stress shielding effect. By optimizing load application, it may be possible to stimulate the degenerative region, thereby promoting matrix reorganization and functional recovery.
Metoder
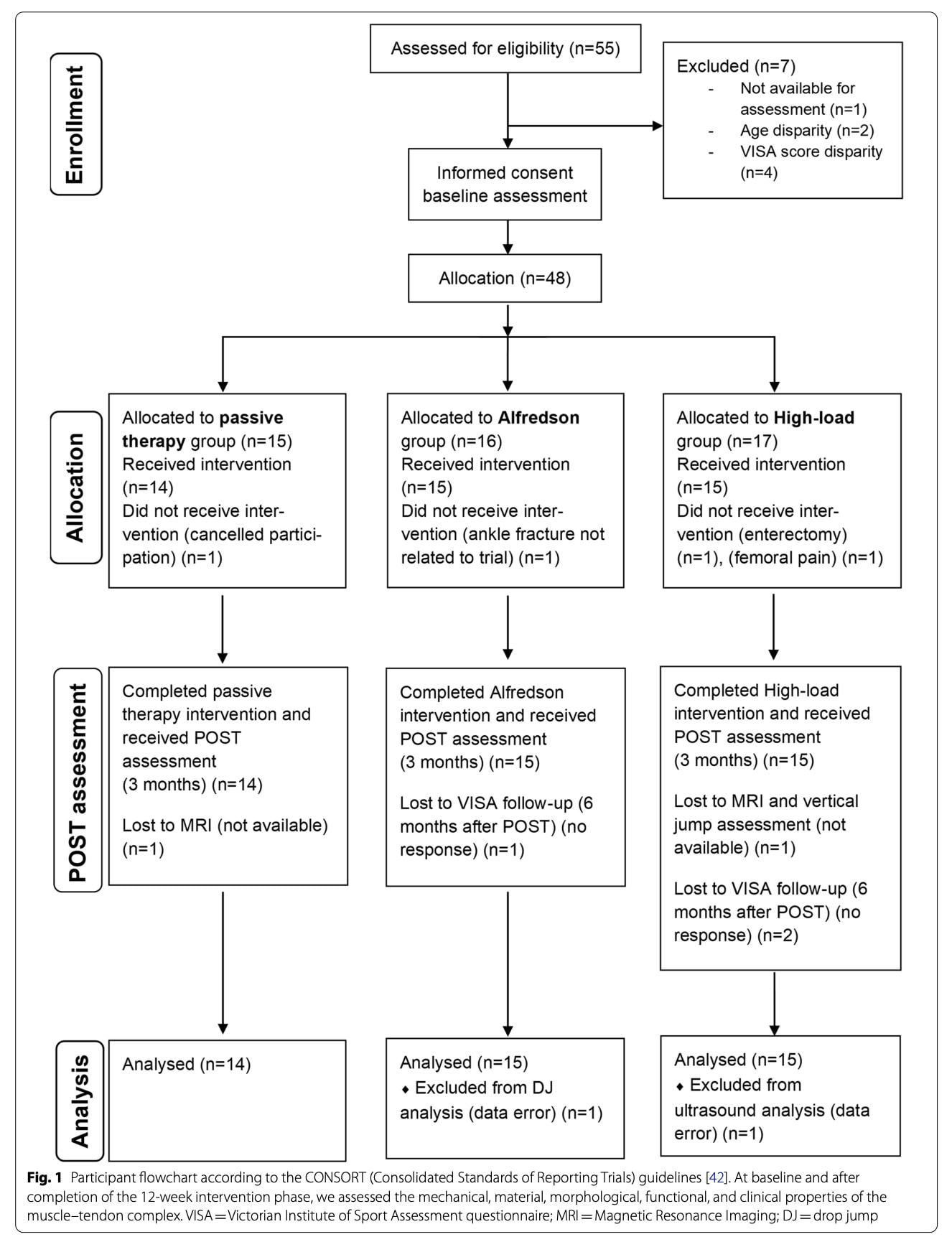
This study was a single-blinded, assessor-blinded controlled trial involving a 12-week intervention program. The design consisted of a three-arm parallel-group trial, with participants allocated to one of three intervention groups.
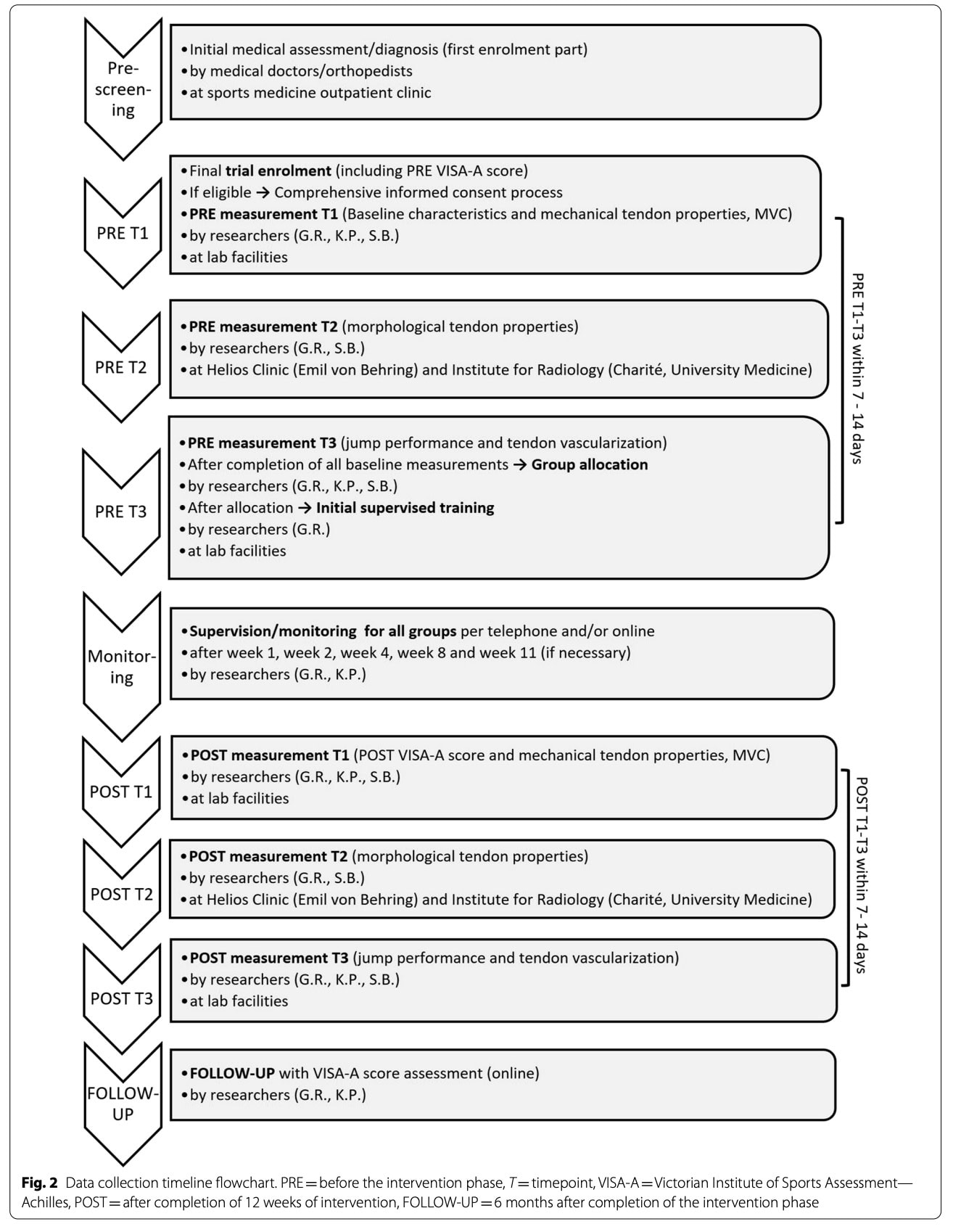
Pre-screening was conducted by medical professionals and included a comprehensive clinical assessment and formal diagnosis. In addition to post-intervention evaluation, a follow-up assessment was conducted online six months after completion of the program.
Inclusion criteria
- Male participants
- Aged 20–55 years
- Chronic Achilles tendinopathy lasting more than 3 months
Diagnosis confirmed by:
- Ultrasound (showing at least discrete hypoechogenic areas in the tendon)
- Clinical assessment by a medical doctor
- VISA-A score < 80, indicating at least moderate symptom severity
If symptoms were bilateral, the more severe leg (lower VISA-A score and higher pain) was selected.
Exclusion criteria
- Corticosteroid injection in the Achilles tendon within the past 12 months.
- Antibiotic use (e.g., fluoroquinolones such as ciprofloxacin, levofloxacin) within the past 12 months.
- Previous leg surgery.
- Tendon rupture or signs of partial rupture.
- Systemic inflammatory diseases (e.g., rheumatoid arthritis, diabetes).
- Spondyloarthropathies (e.g., ankylosing spondylitis).
Allocation and blinding
Forty-eight eligible participants were enrolled and completed all baseline (PRE T1–T3) assessments before group allocation. The allocation sequence was generated and kept confidential by one researcher (G.R.), and remained concealed from all other individuals involved in enrollment, assessment, supervision, and data analysis. Only after completion of baseline measurements was the assessor informed of the participant’s group assignment. All assessments were standardized, study hypotheses were not disclosed, and data were collected and analyzed anonymously without allocation information, ensuring blinding throughout data processing and analysis.
Intervention
During the intervention period, follow-up monitoring and supervision were conducted at weeks 1, 2, 4, 8, and 11 via telephone and/or email to ensure adherence to the protocol. Participants were provided with a training diary to document training frequency, load, and load progression. Daily pain levels were recorded using a Numeric Rating Scale (NRS). The frequency and content of physiotherapy sessions were also documented. Additionally, overall physical activity levels were tracked through the diary.
Participants were permitted to maintain their usual physical training routines, with one restriction: pain had to remain below 3/10 on the NRS during exercise and for 24 hours afterward. No additional strength training specifically targeting the plantar flexors was allowed during the intervention period.
Passive therapy group:
Participants in the passive therapy group received 12 sessions of passive treatment. No exercises involving plantar flexion or active strengthening were performed during the intervention period.
Alfredson group:
The prescribed intervention followed an eccentric heel-raise protocol performed unilaterally on a step, with a 3-second eccentric phase.
Participants completed two sessions per day. Each session consisted of:
- 3 sets of 15 repetitions with the knee extended
- Followed by 3 sets of 15 repetitions with the knee flexed
- A 1-minute rest period was observed between sets.
External load progression was optional and consisted of weekly increments of 5 kg, when tolerated.
High load group:
Participants in the high-load exercise for tendons group received an individualized, feedback-fitted sling device for home-based training.
For the exercise setup, participants were instructed to sit on the floor with knees extended and the forefoot positioned on a footplate. The device was configured to allow maximal isometric contraction at 90° of ankle flexion.
As a warm-up, participants performed 3 sets of 3-second isometric contractions, each followed by 1 minute of rest.
To determine training load, five maximal voluntary contractions (MVCs) were recorded. The prescribed training intensity was set at 90% of the mean value of the five MVCs.
The main exercise protocol consisted of:
- 3-second isometric contractions at 90% MVC
- 3 seconds of rest between repetitions
- Five sets of four repetitions
- 1-minute rest between sets
Training was performed four times per week for 12 weeks. Load progression was set at 5% of the individual training load per week.
For both the Alfredson and high-load groups, no load progression was permitted during the first two weeks of the intervention. Thereafter, progression was allowed only if pain during exercise remained below 6/10 on the Numeric Rating Scale and the individual Rating of Perceived Exertion (RPE) was below 3/10.
Load reduction was recommended if pain exceeded 5/10 or if RPE was greater than 5/10. When reducing the external load was not feasible, the number of repetitions, sets, or training frequency was adjusted accordingly.
Dropout rate reached 8.33%, and participants were reallocated as follows: Passive therapy group (n=14), Alfredson group (n=15) and High-load group (n=15).
Primary outcomes
Mechanical and material properties
Stiffness, Cross-sectional Area (CSA) and Young’s modulus were assessed using dynamometry, electromyography (EMG), ultrasonography and MRI.
Tendon stiffness measurement
Tendon stiffness was assessed using an isokinetic dynamometer with participants seated, the ankle fixed in a neutral position (90°), the knee extended, the hip flexed (~110°), and the pelvis stabilized. Following a standardized warm-up consisting of submaximal plantar flexor contractions and 1–3 maximal voluntary contractions (MVCs), participants performed five ramped 5-second MVCs with 2-minute rest intervals to ensure measurement reliability, followed by 2–3 additional isometric plantar flexor MVCs with similar rest periods and standardized verbal encouragement. Tendon stiffness was calculated as the ratio of tendon force to tendon elongation. Achilles tendon force was estimated by dividing the plantar flexion moment by the tendon lever arm (to note: authors considered the role of antagonist resistance moment when calculating the Achilles tendon force), which was determined using the tendon excursion method by relating displacement of the medial gastrocnemius myotendinous junction, measured via B-mode ultrasound, to ankle joint angular excursion. Changes in lever arm length during contraction were accounted for using a corrective factor in the calculations.
Achilles tendon stiffness was calculated as the slope of the relationship between tendon force and tendon elongation, using data collected between 50% and 100% of the maximum tendon force.
Young’s modulus, a measure of a material’s intrinsic stiffness, of the Achilles tendon was calculated by multiplying tendon stiffness by the ratio of tendon resting length to tendon cross-sectional area.
Clinical outcomes
Clinical severity was assessed using the validated VISA-A score as a patient-reported outcome measure (PROM), evaluated at baseline (PRE, in-person), post-intervention (POST, in-person), and at follow-up (online). A minimum clinically important difference (MCID) of 15 points was considered clinically meaningful. Pain was additionally monitored using a daily Numerical Rating Scale (NRS, 0–10) recorded in a patient diary. Baseline pain values were calculated as the mean of the first 14 days following initial assessment, while post-intervention values were derived from the mean of the final 14 days of the intervention period.
Secondary outcomes
Functional properties
Functional properties were assessed using Counter Movement Jump (CMJ) and Drop Jump (DJ). After a standardized warm-up of up to 12 low- to moderate-intensity jumps, participants performed five maximal CMJ and five drop jumps DJ, barefoot with hands on hips and 1-minute rest between attempts. Drop jumps were executed from a 15 cm box. Ground reaction forces were recorded to determine jump height, calculated using the impulse–momentum method for CMJ and the flight-time method for DJ. For analysis, the mean of the three highest jumps out of five attempts was used for both jump types.
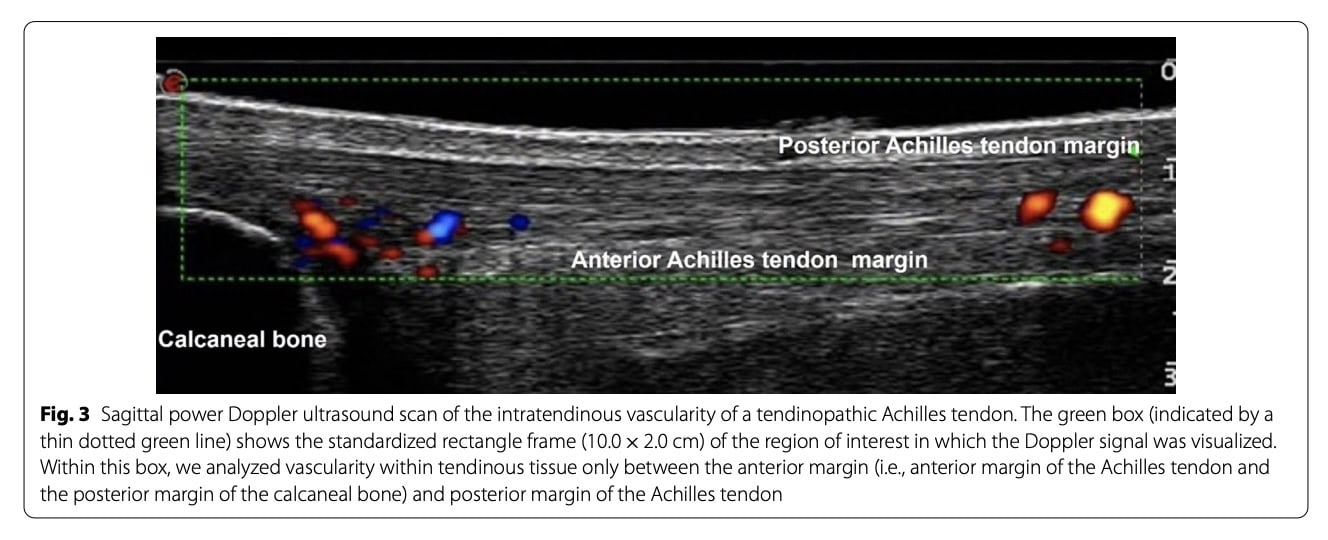
Vascularity
Intratendinous vascularity was assessed using Doppler ultrasonography. Scans were performed to visualize both the proximal calcaneus and the Achilles tendon. Subsequent image analysis enabled quantification of vascularity by converting colored Doppler pixels into an area measurement expressed in mm².
Resultater
Primary outcomes
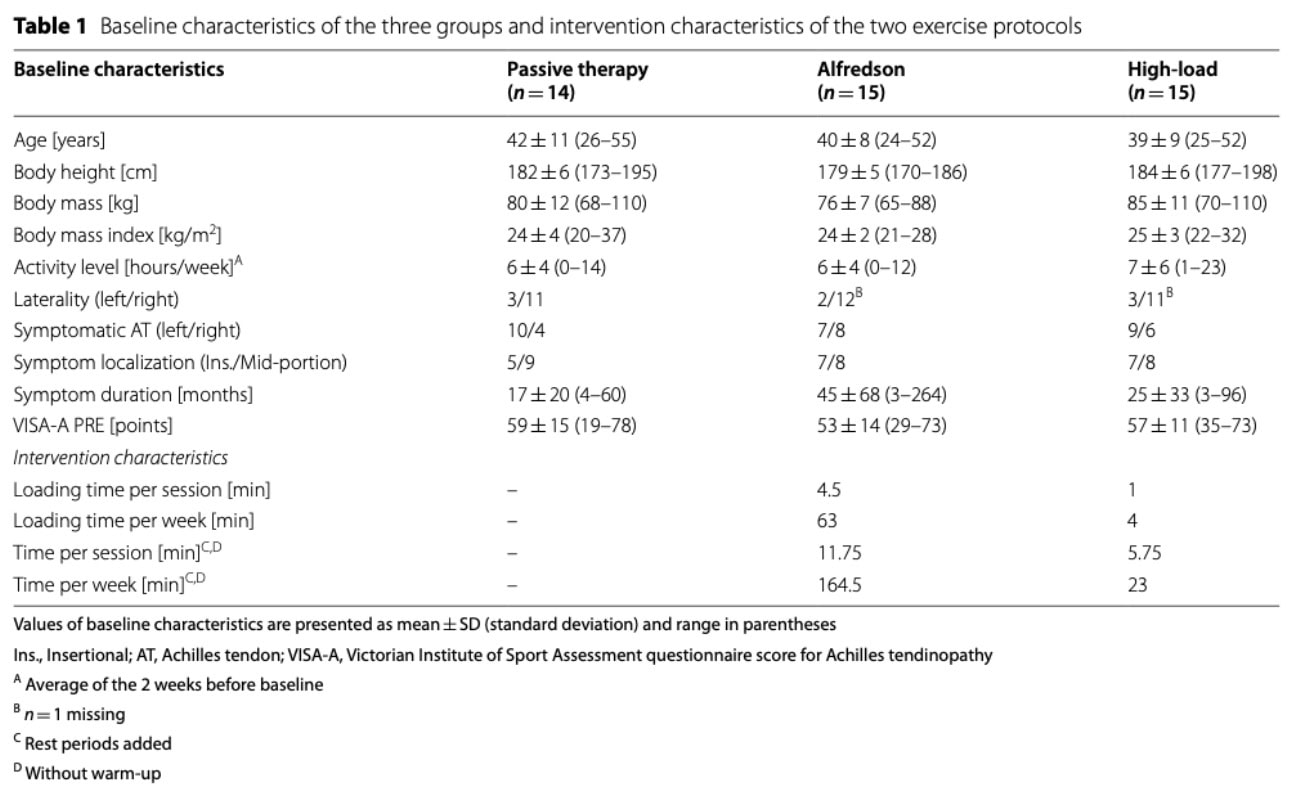
At baseline, plantar flexor strength, tendon force, tendon stiffness, maximum tendon strain, Young’s modulus and tendon rest length did not significantly differ between the three groups.
From PRE to POST, there was a significant time-by-group interaction for MVC measurements, with significant improvements only observed only in the high-load exercise for tendon group.
Tendon force data showed a significant main effect of time from PRE to POST, indicating an overall increase in tendon force. No significant time-by-group interaction was observed. Across groups, tendon force increased.
For tendon stiffness, no overall change was observed over time. However, changes differed between groups: stiffness increased in the high-load exercise for tendon group, decreased in the passive therapy group, and remained stable in the Alfredson group.
Maximum tendon strain showed no overall change over time. However, group-specific responses differed: strain decreased in the High-Load group, while no meaningful changes were observed in the Alfredson or passive therapy groups.
No meaningful changes in stress were observed over time or between groups.
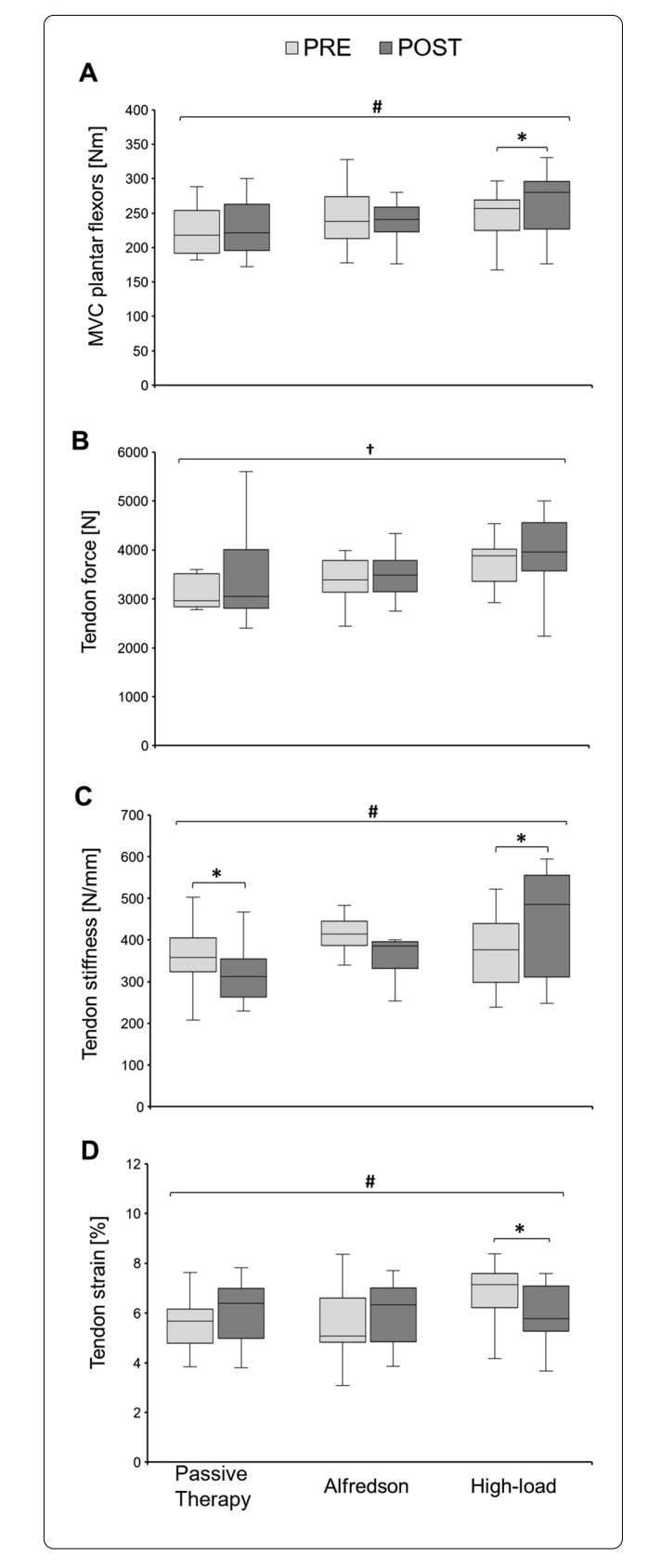
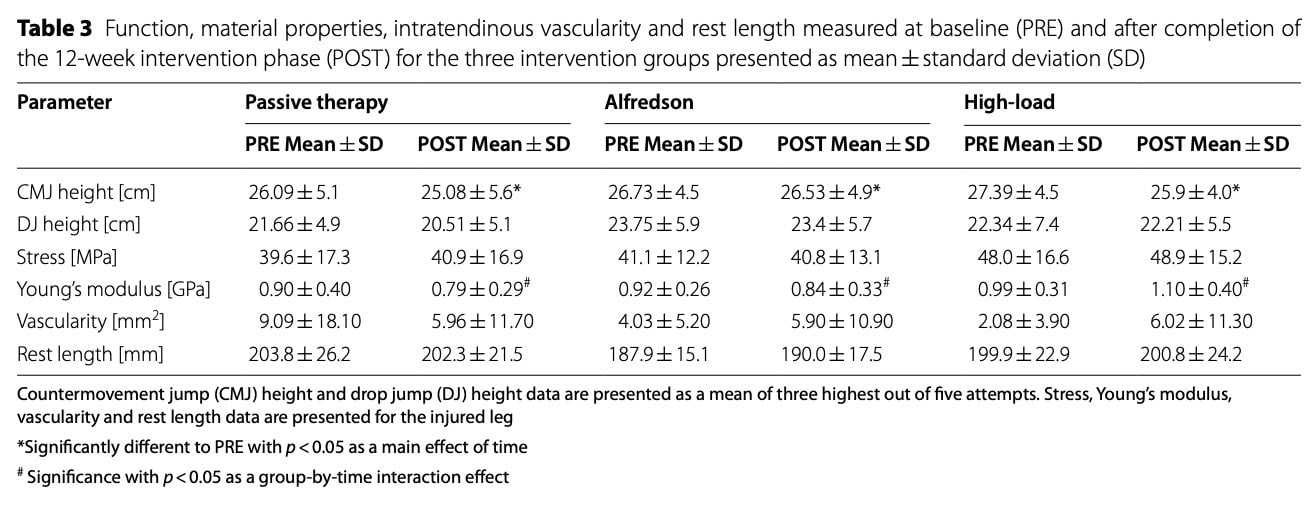
Young’s modulus did not show a clear overall change. Although group-specific variability was observed, no significant pre-to-post differences were detected in any group.
Tendon rest length did not change over time and showed no meaningful differences between groups.
Morphological properties
Mean Achilles tendon cross-sectional area (CSA) did not differ between groups at baseline. Over time, changes in CSA varied by intervention: tendon hypertrophy was observed across the whole tendon length in the High-Load group, whereas no meaningful CSA changes occurred in the passive therapy or Alfredson groups.
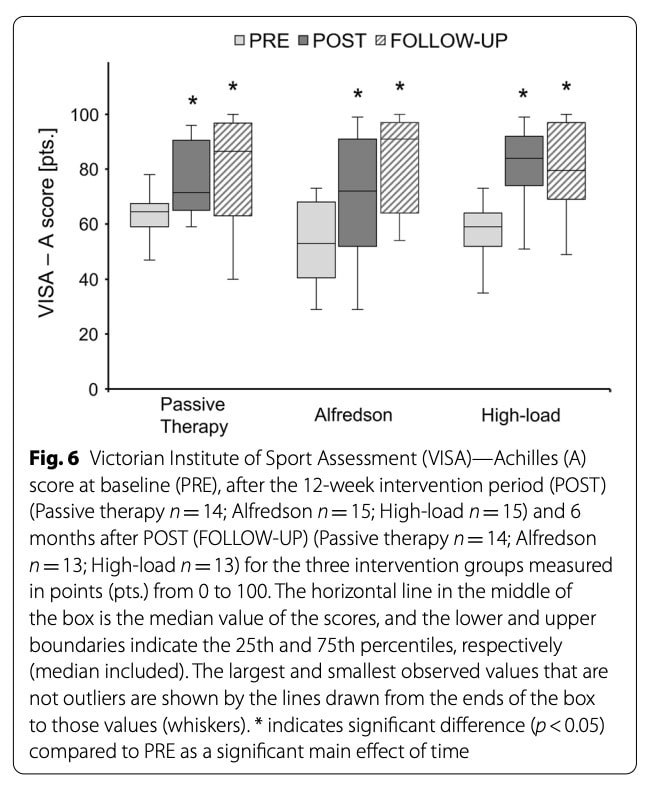
VISA-A scores
Baseline VISA-A scores were comparable between groups. All groups demonstrated clinically meaningful improvements in VISA-A scores from pre- to post-intervention, with gains maintained at follow-up. Improvements were observed across groups, and no meaningful differences in the magnitude of change between groups were detected. VISA-A scores remained stable between post-intervention and follow-up.
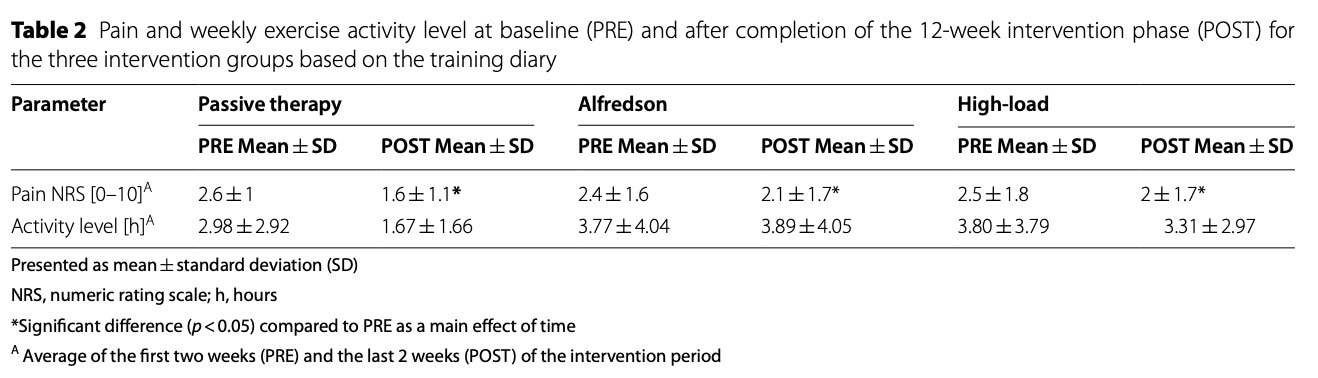
Pain
Baseline pain scores were comparable between groups. Pain decreased over time in all three groups, demonstrating a meaningful reduction in reported symptoms. No significant differences in the magnitude of pain reduction between groups were observed.
Secondary outcomes
Jump performance
Baseline performance was comparable between groups for both countermovement jumps (CMJ) and drop jumps (DJ). CMJ height showed a small overall decrease over time, while no meaningful changes were observed in drop jump height.
Vascularity
Intratendinous vascularity of the injured Achilles tendon was comparable between groups at baseline and showed no meaningful changes over time.
Training Diary Analyses
Compliance
Overall adherence to the interventions was high across all groups, with no meaningful differences between them. Additional attendance at passive therapy sessions varied but remained moderate. No adverse events related to the interventions were reported.
Activity Level
Self-reported activity levels remained stable throughout the intervention period, with no meaningful differences between groups or changes over time.
Progresjon
Both exercise groups progressively increased training load during the intervention, but the magnitude of progression was similar between groups.
Passive Therapy Treatment
Physiotherapists applied a range of non–lower limb loading interventions tailored to individual patients, including manual therapy, core stability exercises, massage and soft tissue techniques, and electro- or thermotherapy modalities. Treatment strategies varied between participants but followed common physiotherapeutic approaches.
Spørsmål og tanker
Pain outcomes did not differ between groups, further calling into question the relationship between structural tendon improvements and symptom relief. Although the high-load exercise for tendons protocol increased tendon stiffness, force production and induced tendon hypertrophy, these structural adaptations were not accompanied by significant pain reduction in the High-Load group. Nevertheless, the capacity of high-load training to enhance tendon mechanical properties suggests potential value for injury prevention, consistent with evidence showing reduced tendinopathy incidence in adolescent handball athlete populations exposed to higher loading strategies.
From a mechanobiological perspective, the limited structural adaptations observed may relate to insufficient loading duration. The three-second isometric holds used in this high-load exercise for tendons protocol may not have generated adequate stress relaxation and creep to load degenerative tendon regions under the stress-shielding model effectively. No differences in vascularity or tissue quality were detected between groups, supporting the idea that mechanical stimuli were below the threshold required to drive measurable matrix remodelling. Experimental evidence from an animal study and a human cadaver study showed that isometric loading at longer holds—approximately 30 seconds—is necessary to achieve meaningful mechanical strain and activation of mechanotransduction pathways on the patellar tendon. Given that tendon tension decreases substantially within this time frame, shorter holds may fail to transmit sufficient mechanical stimulus to the degenerative matrix. This could explain the reduced structural adaptation observed in the present study compared with protocols using prolonged isometric loading.
Snakk nerdete til meg
Both insertional and midportion Achilles tendinopathy were included in the study, which may have introduced heterogeneity in patient responses and potentially influenced the results. As discussed in last week’s article, tendons do not share identical mechanical properties, as these depend on the type of loading to which they are chronically exposed. Tendons subjected to greater compressive loads tend to develop more fibrocartilaginous characteristics. Therefore, the research high-load exercise for tendons protocol may have benefited from a more detailed phenotypic classification of participants.
Although the researchers attempted to standardize group characteristics at baseline (e.g., age, height, weight, activity level), such variables may be insufficient to adequately capture clinically meaningful differences between patients. These considerations raise important questions regarding the phenotypic presentation and classification of individuals with Achilles tendinopathy.
It is well established that imaging findings correlate poorly with pain intensity and functional limitations in this population. Consequently, a purely pathoanatomical classification appears insufficient. There is a need for more comprehensive classification systems that account for the multifactorial nature of Achilles tendinopathy. Future research should aim to identify the biological, psychological, and social factors that contribute to pain and functional impairment. A deeper understanding of these dimensions could facilitate more accurate patient phenotyping and ultimately support the development of precision-based physiotherapy interventions.
Ta med hjem meldinger
- Load matters — but symptoms and structure do not always move together. High-load exercise for tendons improved mechanical properties (stiffness, force production, hypertrophy), yet pain and VISA-A scores improved similarly across all groups — including passive therapy. Structural adaptation does not automatically translate into superior symptom relief.
- Mechanical adaptation requires sufficient stimulus. Tendons are biologically active and load-dependent tissues. However, short 3-second isometric contractions may not provide enough stress relaxation and creep to effectively overcome stress shielding and stimulate degenerative regions. If the goal is structural remodeling, loading parameters (intensity, duration of contraction, time under tension) likely matter more than we traditionally assume.
- Pain-guided loading is safe and feasible. Both active protocols allowed symptom-monitored progression and achieved high adherence with no adverse events. Using pain thresholds (e.g., controlled pain <5–6/10) appears clinically acceptable and practical.
- Passive therapy can reduce pain — but does not improve tendon capacity. While pain decreased in all groups, only high-load training improved mechanical properties. If the objective is long-term tendon resilience or injury prevention, loading strategies remain essential.
- Achilles tendinopathy is not one homogeneous condition. Insertional and midportion tendinopathy likely differ mechanically and biologically. A purely structural or imaging-based classification is insufficient. Future clinical reasoning should integrate mechanical, biological, and psychosocial factors to move toward precision physiotherapy.
Referanse
HVA SKAL SE ETTER FOR Å FORHINDRE SKADER MED HAMSTRING, LEGG OG QUADRICEPS
Enten du jobber med idrettsutøvere på høyt nivå eller amatør, vil du ikke gå glipp av disse risikofaktorene som kan utsette dem for høyere risiko for skade. Dette webinaret vil gjøre deg i stand til å oppdage disse risikofaktorene for å jobbe med dem under rehabilitering!
