
Research
Chronic Pain
January 26, 2026
Centralized pain following nerve injury: diagnostic insights from a recently published systematic review

Introduksjon
Peripheral nerve injury commonly results from surgical procedures, prolonged mechanical compression, or iatrogenic damage and may lead to the development of neuropathic pain. The severity and type of nerve injury can be classified using the Seddon–Sunderland–Mackinnon framework. Neuropraxia is characterized by transient nerve dysfunction without structural damage and typically resolves within weeks to months. Axonotmesis involves axonal disruption with preservation of the connective tissue framework, allowing for potential nerve regeneration. Neurotmesis represents complete nerve transection with disruption of all neural structures and often requires surgical intervention for recovery. Compression-related nerve injuries may range from mild demyelination to complete structural disruption, with each severity level carrying distinct implications for the mechanistic development of centralized pain.
Following peripheral nerve injury, nociplastic pain may develop as a result of altered central pain processing. In such cases, clinical approaches focused solely on peripheral tissue healing may be insufficient. The development of reliable and valid diagnostic criteria is therefore crucial for accurately identifying centralized pain following nerve injury and guiding appropriate management. This systematic review aims to address this gap by synthesizing existing evidence on the clinical characteristics and diagnostic criteria of centralized pain following nerve injury.
Metoder
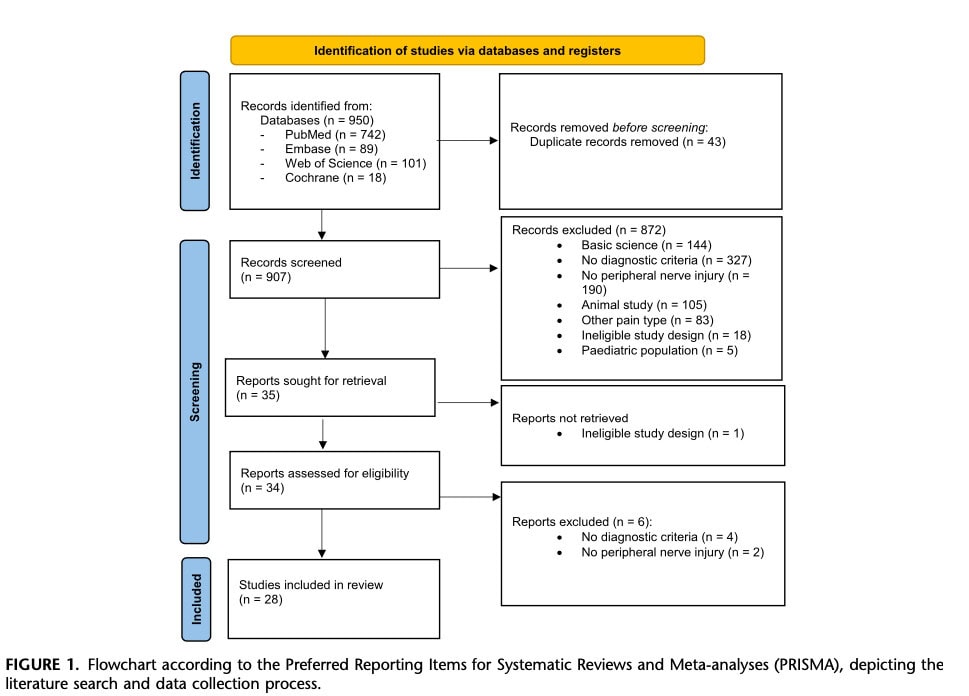
This systematic review adhered to the PRISMA guidelines for systematic reviews and meta-analyses. Research articles evaluating diagnostic approaches for central pain sensitization following peripheral nerve injury were considered for inclusion.
Ekskluderingskriterier:
- Articles published in languages other than English
- Studies involving pediatric populations (<18 years of age)
- Articles with unavailable full tex
- Animal studies
- Studies focusing exclusively on treatment outcomes without diagnostic
- considerations
- Studies addressing acute pain of less than three months’ duration
Articles were screened based on title and abstract. Data were extracted using a standardized form and included the definition of pain centralization, proposed diagnostic criteria or clinical characteristics, assessment methods and diagnostic tests, studied patient populations, clinical signs and symptoms, and quantitative measures used for diagnosis.
Risk of bias was independently assessed using validated tools. The Methodological Index for Non-Randomized Studies (MINORS) was used for non-randomized studies. The quality of case series and case reports was assessed using the Joanna Briggs Institute (JBI) critical appraisal tools. Systematic reviews were evaluated using the Risk of Bias in Systematic Reviews (ROBIS) tool, while narrative reviews were assessed using the Scale for the Assessment of Narrative Review Articles (SANRA).
Resultater
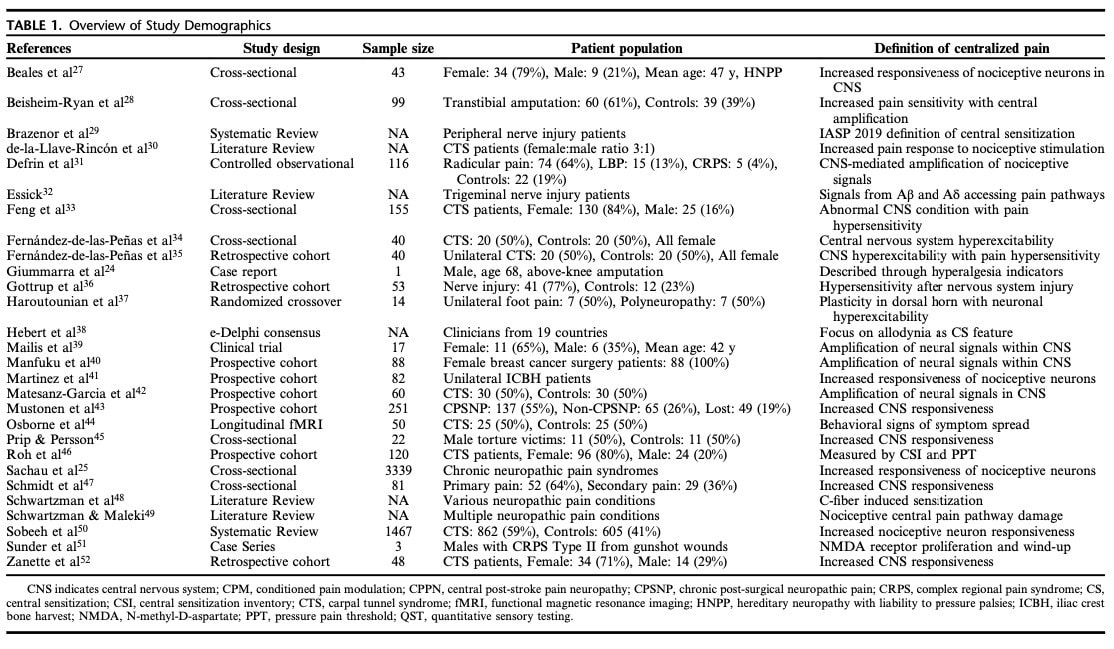
A total of 28 articles were included, encompassing 6,189 patients. These comprised 2 systematic reviews, 4 narrative reviews, 1 case series, 1 case report, 5 cross-sectional studies, and 15 cohort studies (Figure 1). Seven studies focused on carpal tunnel syndrome or post-surgical or amputation-related pain, while three addressed complex regional pain syndrome. The remaining studies investigated a range of conditions, including radiculopathy, traumatic or iatrogenic peripheral nerve injuries, and other chronic pain syndromes.
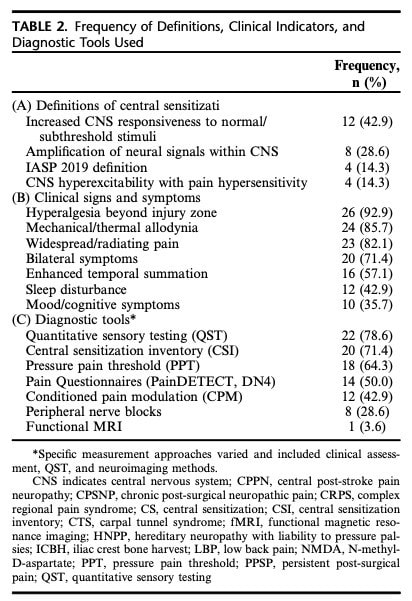
Most methodological limitations, as identified through the various risk-of-bias assessment tools, reflected the absence of prospective sample size calculations and blinding procedures. Across studies, different mechanisms of centralized pain following nerve injury were described; however, all relied on a broadly similar conceptual framework, commonly defined as increased responsiveness of nociceptive neurons within the central nervous system. Additional details on the definitions of centralized pain used in each study are provided in Table 1.
Patient history and physical examination
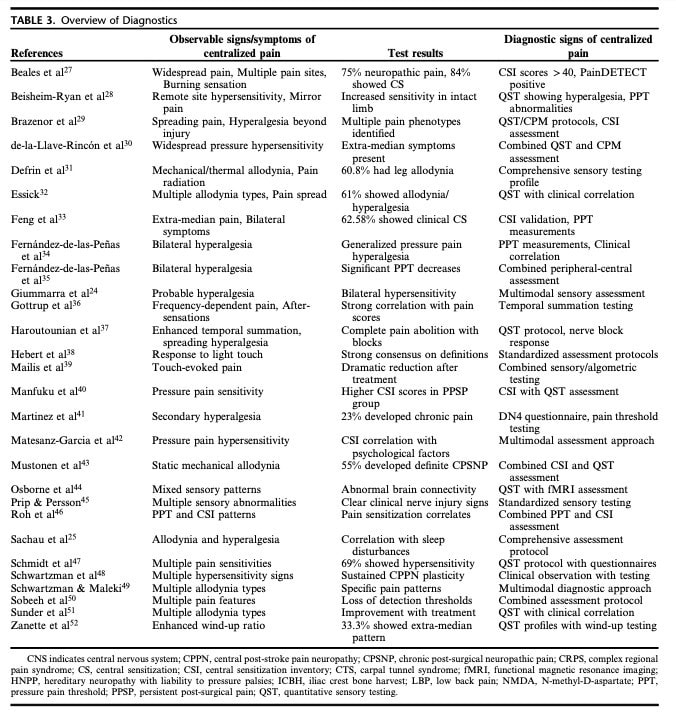
Clinical history and physical examination emerged as key diagnostic components. The presence of widespread pain extending beyond the expected nerve or dermatomal distribution was consistently associated with centralized pain, particularly in carpal tunnel syndrome, where such pain patterns may indicate central sensitization. In patients with radicular pain, leg allodynia was frequently observed (60.8%), whereas it was considerably less common in patients with axial low back pain (13.3%). Sensory testing, particularly light touch and thermal sensation assessment, was identified as an important clinical examination method for detecting features of centralized pain following nerve injury.
Clinical tests
Quantitative Sensory Testing (QST) emerged as a primary tool for the assessment of centralized pain. One study evaluating pressure pain threshold (PPT), conditioned pain modulation (CPM), and temporal summation (TS) reported that these objective measures did not consistently correlate with subjective indicators of central sensitization. In contrast, another study suggested that QST, CPM, and the Central Sensitization Inventory are complementary tools that, when combined, provide a more comprehensive evaluation of central sensitization. Enhanced temporal summation during pinprick testing was identified as a potential indicator of central sensitization. Additionally, one study using the German Research Network on Neuropathic Pain QST protocol found that 69% of patients with both chronic primary and secondary pain exhibited clinical evidence of pain hypersensitivity.
Spørreskjemaer
The Central Sensitization Inventory (CSI) was the most frequently used questionnaire and was commonly administered alongside other patient-reported outcome measures, such as the Pain Catastrophizing Scale. PainDETECT was another widely used questionnaire, while the DN4 questionnaire was commonly employed to assess neuropathic pain.
Intervensjoner
Interventional diagnostic approaches were reported in 9 of 28 studies. These mainly involved pharmacologic agents or nerve blocks to distinguish peripheral from central pain mechanisms. Ketamine-enhanced sympathetic blocks and peripheral nerve blocks were associated with rapid and substantial pain relief, suggesting peripheral contributions to symptoms. Sodium amytal selectively reduced allodynia without affecting deep pain, aiding differentiation between central and peripheral mechanisms. Only one study used imaging diagnostics: longitudinal fMRI revealed abnormal somatosensory connectivity in carpal tunnel syndrome, with both persistent and reversible changes after surgery.
Spørsmål og tanker
Current diagnostic tools, including imaging techniques, provide only indirect measures of centralized pain. This raises the question of whether centralized pain represents a well-defined biological entity or primarily a clinical construct. Many assessments rely on observational or self-reported measures, such as the Central Sensitization Inventory (CSI), which may capture psychological factors such as anxiety or known pain drivers to a greater
extent than nociceptive processes at the structural level. Consequently, these tools may have limited ability to directly assess nociceptive mechanisms underlying pain.
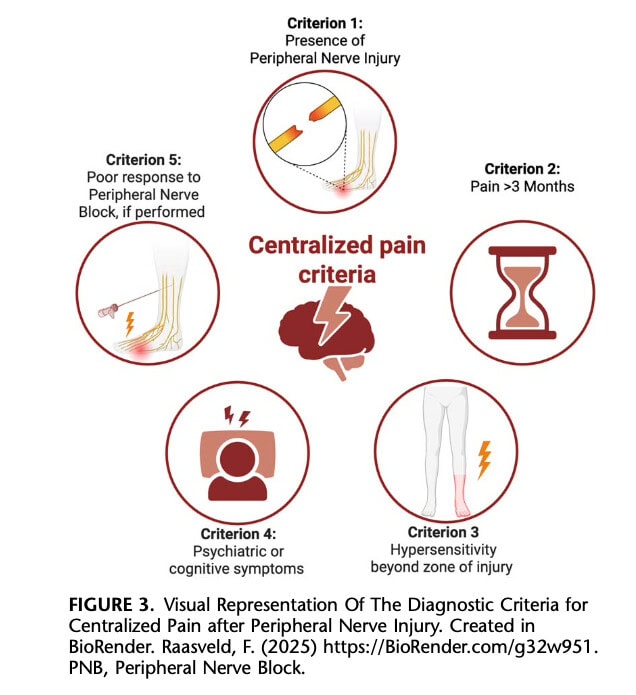
Advanced techniques, such as functional magnetic resonance imaging (fMRI), offer promising insights into altered central pain processing but are not routinely available or used in clinical practice. Interventional diagnostic approaches, such as peripheral nerve blocks, may provide additional information regarding pain mechanisms, as a lack of response or partial response could suggest a centrally mediated pain process. Neuroplastic changes within both the peripheral and central nervous systems are hypothesized to underlie persistent pain, characterized by heightened sensitivity and increased pain facilitation. Clinical phenomena such as temporal summation, which can be directly assessed at the bedside, may reflect these sensitization processes. At the molecular level, neurotransmitters and mediators such as substance P and nerve growth factor are thought to contribute to the reinforcement of pain pathways at both peripheral and central levels. Figure 3 summarizes the proposed diagnostic criteria for central sensitization following peripheral nerve injury.
Snakk nerdete til meg
There is considerable variability in how central sensitization was defined across the included studies. This conceptual inconsistency likely introduced bias, contributing to high heterogeneity and reducing the overall reliability of the findings. The use of more restrictive inclusion criteria and stricter exclusion criteria could have helped limit this heterogeneity. Additionally, heterogeneity could have been further quantified or explored using statistical approaches such as subgroup analyses, sensitivity analyses, or descriptive metrics of variability.
Another methodological concern relates to how the level of evidence informed the authors’ conclusions. Studies ranged from case reports to systematic reviews, yet it remains unclear how these differing levels of evidence were weighted when synthesizing results. It is possible that some conclusions reflect the authors’ subjective selection rather than a systematic, transparent decision-making process.
Given the exploratory nature of this review and the likely scarcity of high-quality data in this field, standard meta-analytic techniques would not have been feasible. Nevertheless, structured subgroup analyses—stratifying studies by the definition of central sensitization, underlying pathology, or study design—would have provided a more systematic approach to assess and report heterogeneity.
Ta med hjem meldinger
- After peripheral nerve injury, persistent pain that extends beyond the expected dermatomal or nerve distribution should raise suspicion of centralized pain mechanisms.
- A thorough history and physical examination are crucial diagnostic steps. Widespread pain, allodynia, altered light-touch or thermal sensation, and enhanced temporal summation are key clinical red flags for central sensitization.
- Questionnaires such as the CSI, PainDETECT, DN4, and catastrophizing scales provide useful context but should not be interpreted as standalone diagnostic tools. They capture symptom burden and pain drivers rather than direct nociceptive mechanisms.
- Quantitative Sensory Testing can help—but isn’t definitive. QST, CPM, PPT, and temporal summation offer valuable objective insights, yet they do not always align with patient-reported measures. A multimodal assessment approach is essential.
- Treatment response is diagnostic information. Limited or absent response to peripherally focused interventions (e.g., nerve gliding, local tissue loading) may suggest a centrally mediated pain component and should prompt a shift in clinical reasoning.
- Neuroplastic changes in the peripheral and central nervous systems—driven by mechanisms such as temporal summation and neurotransmitter activity—underpin real, measurable pain amplification.
- When centralized pain is suspected, management should expand beyond peripheral tissue healing to include pain education, graded exposure, sensory modulation, and strategies targeting the nervous system as a whole.
Listen to this physiotutors podcast to gain more information about central sensitization.
Referanse
Hvordan ernæring kan være en avgjørende faktor for sentral sensibilisering - Videoforelesning
Se denne GRATIS videoforelesningen om Nutrition & Central Sensibilization av Europas #1 kroniske smerteforsker Jo Nijs. Hvilken matpasienter bør unngå vil nok overraske deg!
