
Research
Elbow
January 12, 2026
Is central sensitization in lateral elbow tendinopathy an overlooked pain phenotype? Insights from a cross-sectional study

Introduksjon
Lateral elbow tendinopathy is a leading cause of disability among active populations. Commonly affecting workers engaged in physically demanding and repetitive tasks, lateral elbow tendinopathy is often referred to as tennis elbow and was initially associated with inflammation of the wrist extensor tendons. However, recent advances in the understanding of tendon pathology have led to a reclassification of this condition, with the term tendinopathy now preferred over inflammatory-based terminology.
In chronic presentations, particularly when peripheral tissue structures appear structurally sound, central sensitization is thought to play a crucial role in the persistence of symptoms. Central sensitization involves dysregulation of neural pain signalling within the central nervous system, resulting in heightened pain sensitivity, including symptoms such as hyperalgesia and allodynia. Central sensitization in lateral elbow tendinopathy may represent a key mechanism underlying poor response to evidence-based treatments, highlighting the growing importance of identifying individuals who present with this specific pain phenotype.
This cross-sectional study investigates the relationship between central sensitization in lateral elbow tendinopathy (LET), with a particular focus on the influence of psychosocial factors such as anxiety and depression.
- The primary aim is to examine the predictive role of biopsychosocial factors—including pain intensity, pain interference, and psychological and psychosocial variables—on Central Sensitization Inventory (CSI) scores in individuals with LET.
- The secondary aim is to identify which pain-related and psychosocial measures are associated with functional ability in this population.
Metoder
Study design
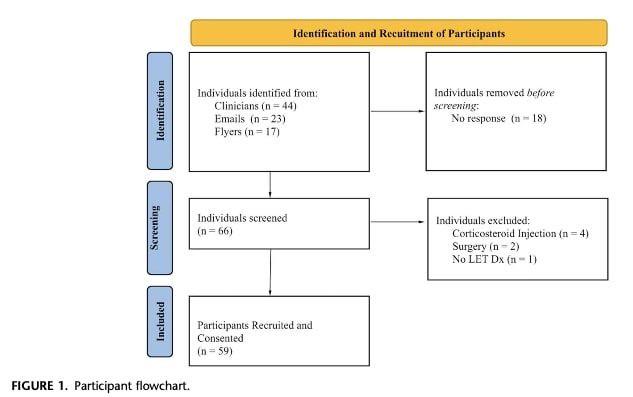
Participants were recruited through convenience sampling, meaning that eligible patients were identified by clinical staff and enrolled via email.
Participants provided:
- Demographic information
- Past medical history
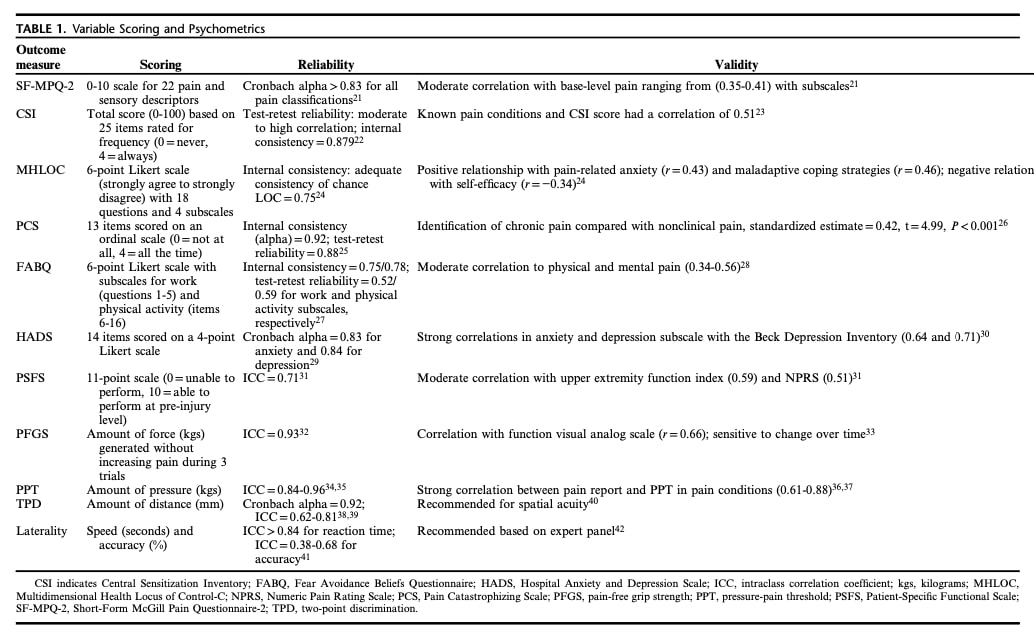
Patient-reported outcome measures, including:
- Patient-Specific Functional Scale (PSFS) : Evaluates meaningful functional tasks that patients find difficult due to lateral elbow tendinopathy.
- Numeric Pain Rating Scale (NPRS): Measures pain intensity on a numerical scale.
- Short-Form McGill Pain Questionnaire–2 (SF-MPQ-2): A self-administered questionnaire used to differentiate neuropathic from non-neuropathic pain.
- Central Sensitization Inventory (CSI): Assesses symptoms related to central sensitization.
- Multidimensional Health Locus of Control–C (MHLOC): Evaluates patients’ beliefs regarding their control over their health condition.
- Pain Catastrophizing Scale (PCS) Measures the presence of exaggerated negative thoughts about anticipated painful experiences.
- Fear-Avoidance Beliefs Questionnaire (FABQ): Examines fear-avoidant behaviours related to pain.
Participants then completed clinical measures:
- Two-Point Discrimination (TPD) Testing: Evaluates the patient’s ability to distinguish between two closely spaced tactile stimuli.
- Pressure-Pain Threshold (PPT): A sensory test that quantitatively measures the amount of pressure required to elicit pain at the lateral elbow on both sides. It also helps to objectively identify hyperalgesia.
- Pain-Free Grip Strength (PFGS): Assessed using a handheld dynamometer to measure grip strength without eliciting pain.
- Laterality Testing: Evaluates the ability to distinguish between the left and right sides of one’s body. Laterality was assessed by measuring participants’ accuracy in identifying the left or right orientation of 25 upper extremity images. Altered laterality recognition has been observed in patients with chronic pain.
Inclusion criteria
- English-speaking and able to read.
- Aged 18 to 75 years
- Diagnosis of lateral elbow tendinopathy (LET), confirmed by pain provoked in at least 2 of the following 4 clinical tests:
Exclusion criteria
- Receipt of any medical intervention for the condition from a state-licensed physician within the past 90 days
- Positive mechanical sensitivity of the median nerve (Upper Limb Neurodynamic Test A [ULNTa])
- Bilateral lateral elbow tendinopathy (LET)
- Pain provocation during passive elbow flexion
A single examiner was involved to enhance internal validity. Cross-sectional design inherently diminishes selection bias. A sample size of 59 participants was determined to ensure adequate statistical power.
Data Analysis.
Primary question (CSI and pain experience):Participants were divided into two groups based on their CSI score: high central sensitization (CS) and low CS. A median split was used because there is no validated CSI cutoff for this specific population.
The two groups were compared to see if they differed in demographics and pain-related measures. Statistical tests were used to compare:
- categorical data (e.g. sex)
- continuous data (e.g. pain scores)
Then, the two groups were compared on multiple pain and psychological measures (pain intensity, pain interference, psychological factors, and sensory tests).
Variables that showed significant differences between groups were included in a logistic regression analysis to determine:
- Which factors were most strongly associated with higher CSI scores
- how much each factor contributed
Secondary question (pain experience and function):A linear regression analysis was used to examine which factors were related to function.
- Functional ability (PSFS score) was the outcome variable
- Pain, psychological, and clinical measures were added step by step as predictors
This approach identified which factors significantly influenced function in people with lateral elbow tendinopathy (LET) and how strongly they were associated with functional limitations.
Results
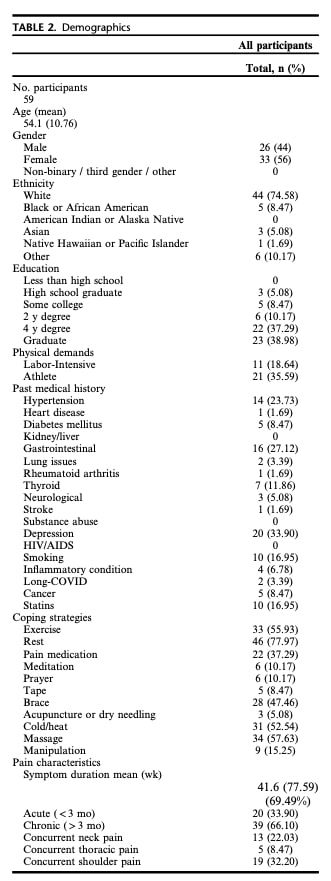
59 participants were enrolled in the study. Table 2 further provides demographic details.
Patients were divided into a high central sensitization group (n = 29) and a low central sensitization group (n = 30). A CSI cutoff score of 21 was used to distinguish between the high and low central sensitization groups.
No statistically significant differences were found between the groups in terms of age, sex, or duration of symptoms.
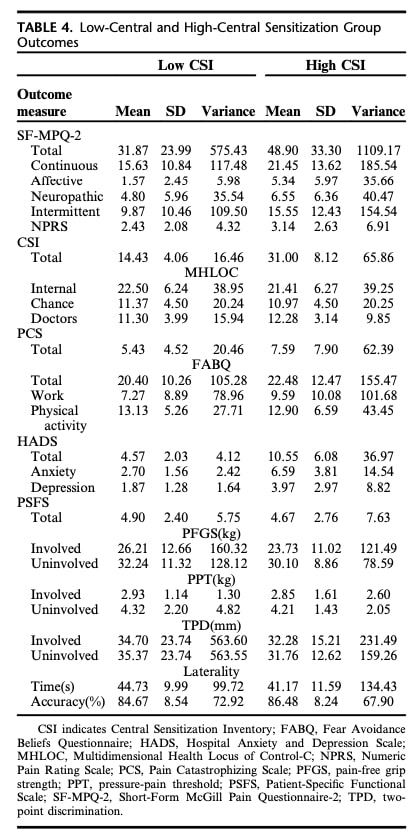
Significant differences were observed between the groups for the SF-MPQ-2 continuous, SF-MPQ-2 intermittent, SF-MPQ-2 affective, HADS anxiety, and HADS depression subscores.
Meaningful differences were also found between the groups regarding past medical conditions, including gastrointestinal issues and depression, with the high central sensitization group showing a higher prevalence of these conditions.
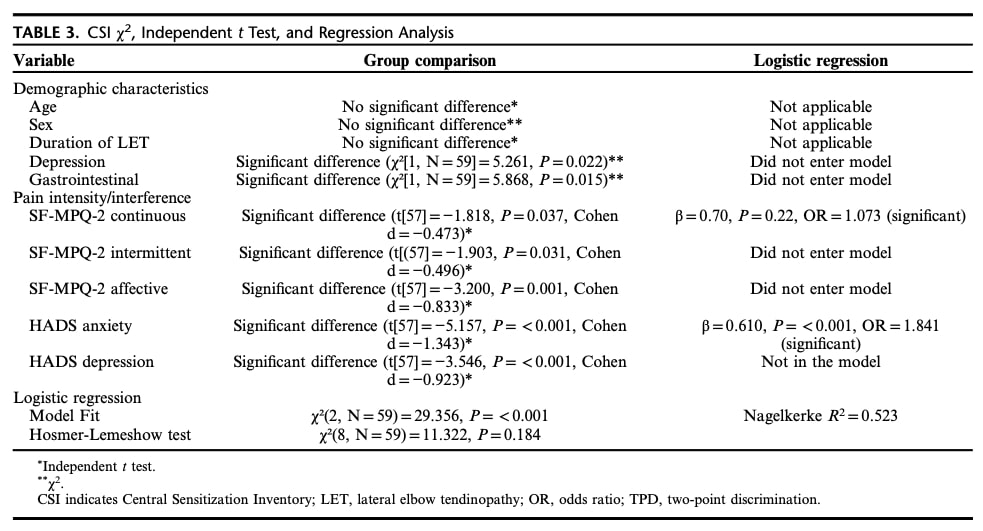
A logistic regression analysis was used to determine which pain and psychological factors could predict whether individuals with lateral elbow tendinopathy (LET) belonged to the high or low central sensitization (CS) group. The analysis met all statistical assumptions and showed a good model fit.
The model explained about 52% of the differences in CSI scores and correctly identified nearly 80% of individuals with high CS, which was a clear improvement compared to chance. Among all variables tested, continuous pain intensity (SF-MPQ-2) and anxiety (HADS-Anxiety) were the only significant predictors of belonging to the high-CS group. Individuals with high CS reported higher ongoing pain and higher anxiety levels, supporting the study’s main hypothesis.
To examine which factors were related to functional ability, a second analysis was performed using PSFS as the outcome measure. All pain-related, psychological, and clinical measures were tested. The final model was statistically significant but explained only 7.6% of functional performance, indicating a weak predictive ability.
Only two-point discrimination (TPD) of the affected elbow was significantly associated with function, but the overall model was not strong enough to reliably predict functional ability in individuals with LET.
Spørsmål og tanker
Positive mechanical sensitivity testing of the median nerve was used as a differential test to identify a radicular source of pain. However, a negative Upper Limb Neurodynamic Test (ULNT) alone does not necessarily rule out cervical spine involvement; The cluster of Weiner provides additional assessments to confirm or rule in cervical contributions. Modulation of symptoms through repetitive movement testing could also help differentiate central sensitization in lateral elbow tendinopathy from cervical involvement.
Table 2 presents patient demographics, showing that 22.0% of patients reported concurrent neck pain, 8.5% thoracic pain, and 32.2% shoulder pain, highlighting the potential for patient misclassification and involvement of additional peripheral structures instead of sensitization in lateral elbow tendinopathy.
Anxiety and continuous pain were significant predictors of group membership (high versus low central sensitization), suggesting that these easily assessed clinical characteristics may be valuable for identifying patients presenting central sensitization in lateral elbow tendinopathy.
Talk nerdy to me.
The authors determined the CSI cutoff score by dividing patients into high and low central sensitization groups using the median CSI score. This approach enabled the use of a non-continuous analysis method; however, the CSI is inherently a continuous scale, with higher scores indicating greater central sensitization. Using a median-based dichotomization represents an alternative method that is not formally validated.
This dichotomization may have influenced the study results. For example, Table 4 shows similar laterality discrimination scores between the high and low CS groups, despite no statistically significant relationship being reported. This could be due to the arbitrary CSI cutoff chosen by the authors. The high variance observed in the High CS group suggests a heterogeneous distribution, indicating that the CSI-based classification may not be sensitive enough to detect subtle differences, potentially limiting the clinical relevance of this outcome.
Beyond age, sex, and duration of lateral elbow tendinopathy symptoms, it is unclear whether the two groups were well-matched for other demographic or clinical factors. Potential confounders, such as medication use, were not reported. Regular use of over-the-counter analgesics, for instance, could reduce perceived pain levels, thereby affecting outcomes on pain and function questionnaires.
Take-home messages
- Anxiety and continuous pain are important indicators to evaluate central sensitization in lateral elbow tendinopathy.
- Administering tools such as the HADS and SF-MPQ-2 can help clinicians better understand the patient’s pain experience.
- The Central Sensitization Inventory (CSI) can be used to assess CS in lateral elbow tendinopathy.
- Results should be interpreted as a continuum, with higher scores indicating greater central sensitization.
- Two-Point Discrimination (TPD) testing shows promise as a quantitative clinical measure of central sensitization in lateral elbow tendinopathy, but further research is needed to confirm its utility.
Methodological caution:
- The study’s dichotomization of CSI scores using a median cutoff is not validated and may introduce bias, limiting the interpretation of results.
Clinical assessment recommendations:
- Evaluate all relevant body structures and adopt a comprehensive biopsychosocial approach.
- Consider using the Pain and Disability Drivers Management Model as a framework to identify the primary drivers of pain and disability and guide individualized rehabilitation https://www.physiotutors.com/understanding-the-pain-and-disability-drivers-management-model-for-rehabilitation/
Referanse
Hvordan ernæring kan være en avgjørende faktor for sentral sensibilisering - Videoforelesning
Se denne GRATIS videoforelesningen om Nutrition & Central Sensibilization av Europas #1 kroniske smerteforsker Jo Nijs. Hvilken matpasienter bør unngå vil nok overraske deg!
