Research
Diagnosis & Imaging
July 31, 2025
Višedimenzionalno fenotipiziranje boli u donjem dijelu leđa: Klinička korisnost PDDM modela za ciljano liječenje

Uvod
Chronic low back (CLBP) pain is leading cause of disability and represent major socio-economic burden. Chronic low back pain is characterized as a longstanding pain and disability (more than 3 months). Anatomical source of pain is often hard to identify, and chronic low back pain is associated with multidimensional features such as biophysical, socio economic, genetics and emotional distress. Regarding the complexity of chronic low back pain, traditional classification system, used to tailor treatment to patient’s presentation are often falling short when assessing the multidimensionality of this pathology.
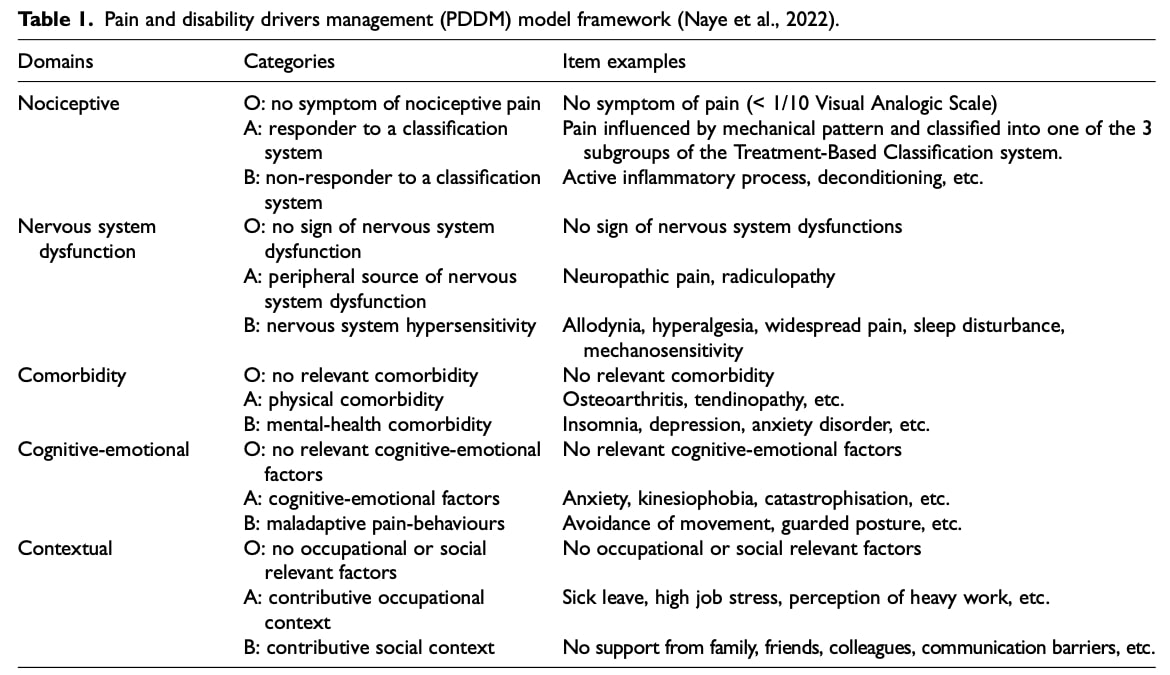
As treatment focusing on multidimensional aspect of chronic low back pain have been demonstrated to impact on low back pain outcomes, it remains to develop a validated system classifying patient based on low back pain presentation. The Pain and Disability Driver Model (PDDM) provides a multidimensional low back pain phenotyping classification that surpasses traditional anatomical systems by incorporating both physical and psychosocial drivers.
To address this gap, this study first investigates the prognostic value of PDDM for pain and disability outcomes. Second, the researchers aimed to determine the analytical value of PDDM for CLBP patients.
Metode
Study design
This study employed a retrospective, monocentric cohort design, meaning that researchers retrospectively evaluated patient data from a single hospital without a predefined intervention protocol, to assess outcomes and determine the prognostic value of the multidimensional low back pain phenotyping classification system.
Population
All participants were enrolled from a multidisciplinary rehabilitation program for chronic non-specific low back pain (CLBP), provided they:
- Completed at least 3 weeks of the program
- Met all program entry requirements:
- Had chronic non-specific low back pain
- Experienced work difficulties due to CLBP (either ≥1 month of work absence in past year or currently on sick leave)
- Expressed motivation to return to work
Program Overview
This intensive 4-week rehabilitation program required patients to attend daily 6-hour sessions, 5 days per week. A specialized healthcare team including physiotherapists, physicians, occupational therapists, psychologists, and other experts delivered a comprehensive intervention with three core components: physical rehabilitation (featuring stretching, strengthening, cardio training, and aquatic therapy), pain education (covering spinal pathophysiology, pain mechanisms, and ergonomics), and wellness workshops (Yoga, Qi-Gong, and relaxation techniques). Patients participated in small groups of 4-6, with optional individual consultations available (nutritionist, psychologist or social worker). It is important to note that no specialized therapies—such as graded exposure to feared movements, activity logging, or mirror therapy—were provided to patients in this study.
Assessment Protocol
The program began and ended with thorough evaluations including clinical exams, physical testing, and validated psychosocial questionnaires measuring work-related stress (Karasek), mental health (Hospital Anxiety and Depression scale), functional limitations (Oswestry Disability Index) and pain-related beliefs (Fear-Avoidance Beliefs Questionnaire, Pain Catastrophizing Scale). Patients received structured follow-up at 1, 3, and 6 months post-program with encouragement to maintain physical activity and work reintegration.
Data Collection Protocol
The study gathered baseline sociodemographic information (age, gender, pain duration, and work absenteeism) along with comprehensive biopsychosocial profiling using the PDDM framework. Two healthcare professionals (a physician and physiotherapist) independently applied the multidimensional low back pain phenotyping classification to categorize patients into PDDM domains (O, A, or B), resolving discrepancies through consensus meetings and third-party arbitration when required. While inter-rater reliability ranged from moderate to good for typical cases, it proved more variable for atypical presentations. No preparatory training cases were conducted, which may have compromised the validity of the classification.
Mjere ishoda
Outcomes measured included perceived function (ODI) and pain intensity (VAS, 0-100) at baseline (T0) and program end (T4). Work status was monitored until the final available follow-up, which extended beyond the scheduled 1/3/6-month checkpoints if patients returned for additional care.
Statistical analysis will be further discussed in the Talk nerdy to me section.
Rezultati
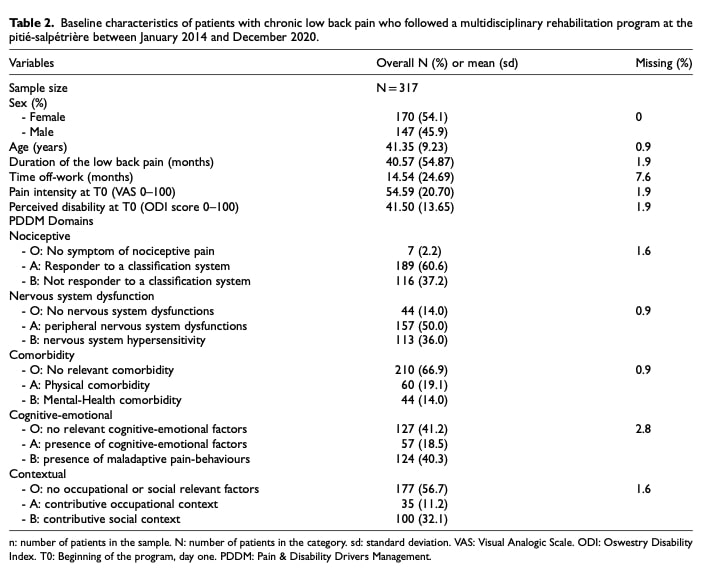
Out of 322 patients enrolled in a multidisciplinary rehabilitation program, 317 were included in the analysis. The average age was 41 years, with 54% women. Patients had chronic low back pain for an average of 40 months and were off work for about 14 months. Baseline disability (ODI) was 41/100, indicating severe disability. Key clinical profiles included: 37% not fitting nociceptive classifications, 36% with signs of central sensitization, 33% with physical or mental comorbidities, 58% with maladaptive cognitive-emotional factors, and 44% with work or social difficulties. The program resulted in significant reductions in disability (mean change: 7.2) and pain intensity (mean change: 9.8).
Primary Objective: Prognostic Value of the PDDM
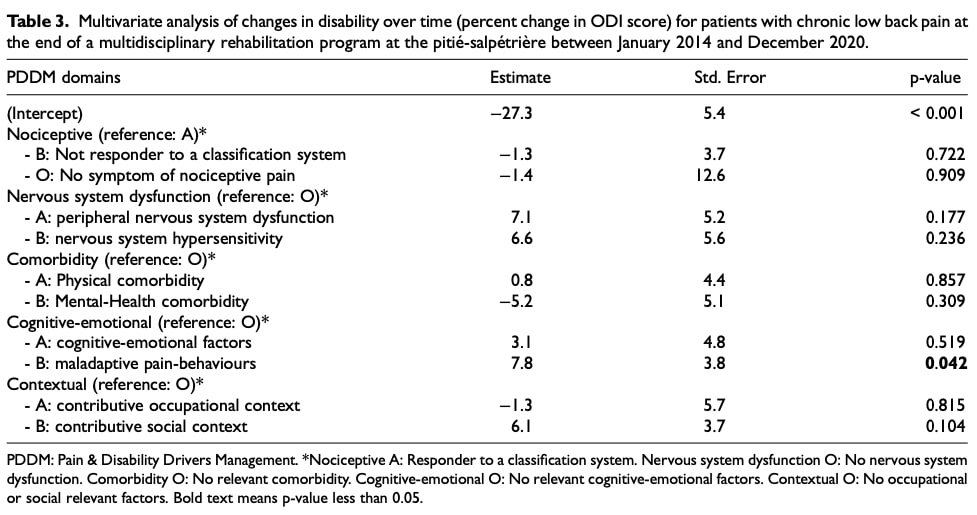
In the main multivariate analysis, patients classified in category B of the cognitive-emotional domain corresponding to maladaptive pain behavior showed a significantly smaller improvement in disability compared to those in category O (estimated difference: –7.8%).
In contrast, classifications in the other domains — nociceptive, nervous system dysfunction, comorbidity, and contextual — did not significantly affect changes in disability during the program (see Table 3). A separate analysis using only complete cases also found no significant association between any domain classifications and disability change over time.
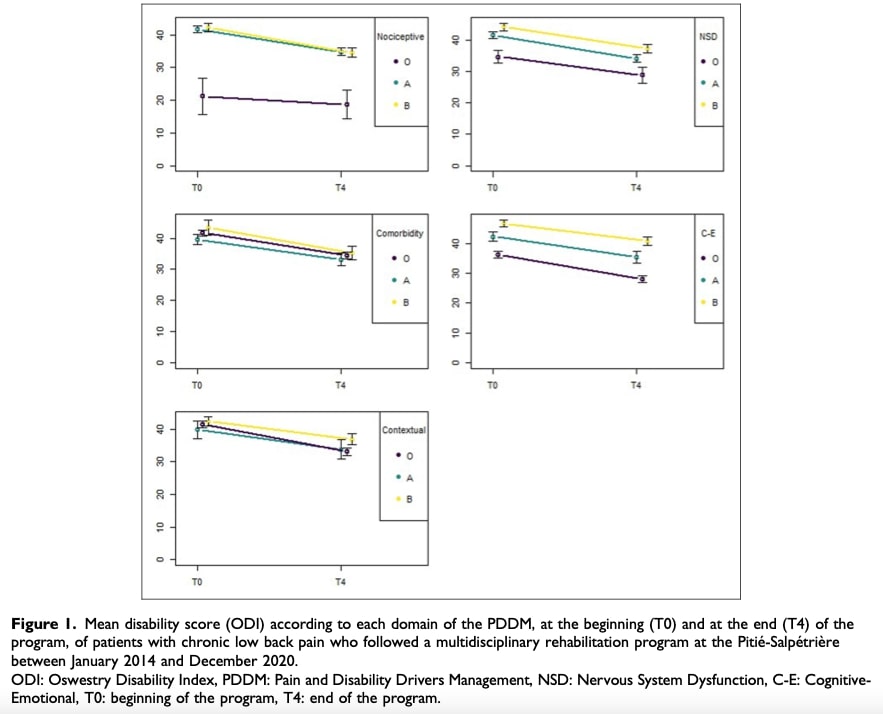
In the bivariate analysis, the same trend was observed: patients in category B of the cognitive-emotional domain had a smaller reduction in disability compared to those in category O. Differences in the other domains were not statistically significant. Figure 1 illustrates the ODI scores at the start (T0) and end (T4) of the program across the different categories.
Secondary Outcomes
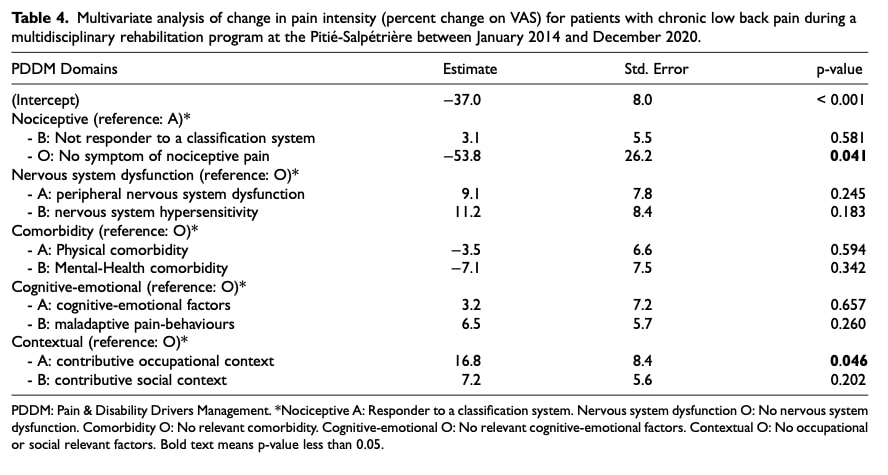
For pain intensity, patients in category O of the nociceptive domain experienced a greater reduction in pain (–53.8%), while those in category A of the environmental domain showed a slight increase in pain intensity (+16.8%). No other domain classifications were significantly associated with changes in pain intensity (Table 4).
Finally, logistic regression analysis revealed that return-to-work outcomes were not significantly associated with any domain of the multidimensional low back pain phenotyping model at final follow-up.
Secondary Objective: Analytic Value of the PDDM
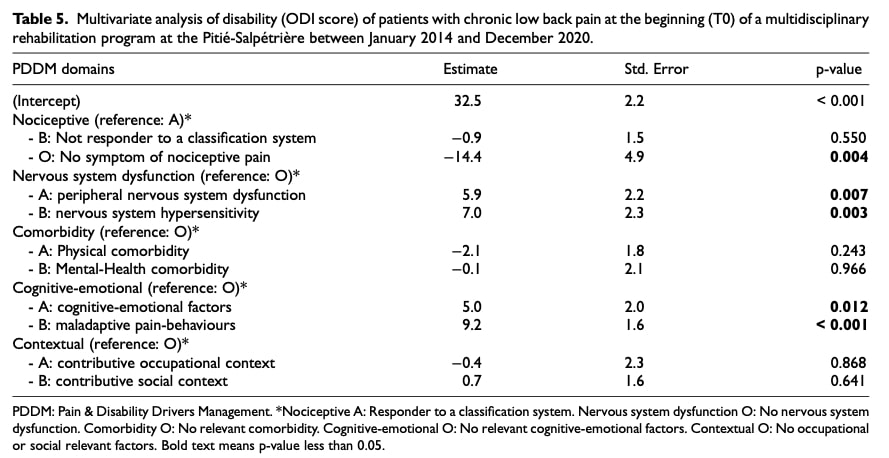
At the start of the program (ODI at T0, on a 100-point scale), baseline disability levels varied according to PDDM domain classifications:
- In the nociceptive domain, patients in category O had significantly lower baseline disability compared to others (Mean difference: –14.4 points)
- In the nervous system dysfunction domain, being in category A or B was associated with higher baseline disability:
- Category A: +5.9 points
- Category B: +7.0 points
- In the cognitive-emotional domain, patients in category A or B also showed higher baseline disability:
- Category A: +5.0 points
- Category B: +9.2 points
- In contrast, classifications within the comorbidity and contextual domains were not significantly associated with baseline disability levels.
Pitanja i razmišljanja
This study can be analyzed through the lens of the ADTO model for patient care proposed by Kevin Spratt. This framework outlines a structured and rigorous clinical reasoning process involving four key steps:
- A — Assessment: The clinician gathers comprehensive information about the patient’s symptoms, health status, medical history, and expectations.
- D — Diagnosis: Based on the assessment, the clinician identifies the patient’s condition using a structured diagnostic approach.
- T — Treatment: Treatment decisions are made based on the diagnosis and assessment findings.
- O — Outcomes: Patient outcomes are monitored and reassessed to evaluate the efficacy of the treatment and adjust strategies as needed.
In this study, the Assessment component of the multidimensional low back pain phenotyping model involves identifying factors contributing to pain and disability. The authors assessed five domains of the PDDM (nociceptive, nervous system dysfunction, comorbidities, cognitive-emotional, and contextual factors) using validated questionnaires. These included the Karasek questionnaire (psychosocial risk), the Hospital Anxiety and Depression Scale (HAD), the Pain Catastrophizing Scale (PCS), and the Fear-Avoidance Beliefs Questionnaire (FABQ). While these tools provide valuable quantitative data for the cognitive-emotional, contextual, and comorbidity domains, they offer limited insight into the nociceptive and nervous system dysfunction domains. Moreover, the absence of quantitative assessments or advanced examinations for these latter domains limits the reliability and consistency of their evaluation.
Regarding the Diagnosis step, a major limitation of the PDDM model is its lack of quantitative thresholds for classifying patients within the five domains, which compromises its reliability as a classification tool. In the nociceptive domain, the study relies on the Treatment-Based Classification (TBC) system. However, studies have shown moderate reliability for TBC, with category agreement ranging from 66% to 81%. This variability calls into question the diagnostic consistency of the biopsychosocial classification of low back pain and, by extension, the appropriateness of treatments based on it.
In comparison, the Mechanical Diagnosis and Therapy (MDT) system has demonstrated moderate to good reliability among trained clinicians, but significantly lower reliability among those without formal MDT training 1. If a classification tool is unreliable or inconsistently applied, the resulting treatment strategies are inherently biased. This complicates the interpretation of patient progress: Are improvements due to treatment efficacy, contextual factors, placebo effects, or simply natural recovery?
This uncertainty could explain why the study did not observe substantial improvement in patients categorized within the nociceptive and nervous system dysfunction domains. Furthermore, central sensitization was not directly assessed in this study, limiting the opportunity to address it with advanced treatments such as graded motor imagery. The treatment protocol is difficult to generalize, as it involved intensive sessions lasting six hours per day, five days a week. Moreover, the lack of patient centered treatment, individualized care and specialized intervention may have limited its effectiveness. As the PDDM (Pain and Disability Drivers Model) is a valuable tool for identifying biopsychosocial contributors to patient pain and disability, it should guide targeted interventions. Previous Physiotutors reviews 2, 3. have demonstrated the effectiveness of Cognitive Functional Therapy (CFT) in reducing pain and disability for patients with chronic nonspecific low back pain.
In terms of Outcomes, the study reassessed only disability (ODI), pain levels, and return-to-work status. Other important patient-reported outcomes — such as psychological distress and fear-avoidance behavior (measured by Karasek, HADS, PCS, and FABQ) — were not re-evaluated post-intervention. This omission makes it difficult to determine whether these psychosocial and emotional domains improved and, if so, whether they influenced pain and disability outcomes. Conversely, it remains unclear whether persistent psychological or contextual factors may have limited recovery.
Reassessing all domains could have provided more individualized insights. For instance, if a patient initially showed high levels of emotional distress on the HADS and received appropriate psychosocial intervention, a quantitative reduction in depression or anxiety might be observable. If this did not correlate with improved pain or function, clinicians could then revisit their clinical reasoning and form new hypotheses, potentially adapting the treatment plan.
Pričaj štreberski sa mnom
Descriptive Analysis
The researchers used descriptive statistics to summarize the study sample. For quantitative variables (like age or disability scores), they reported the mean and standard deviation, while categorical variables (such as gender or classification within PDDM domains) were expressed as percentages.
To evaluate changes over time, they calculated the mean change in disability and mean change in pain intensity from the beginning to the end of the program. These changes were tested using paired Student’s t-tests for exploratory purposes.
Primary Objective – Main Analysis
To evaluate whether PDDM-based multidimensional low back pain phenotyping could predict disability changes, researchers performed multivariate linear regression analysis. The outcome was the percentage change in disability between T0 and T4. As explanatory variables, they included the five domains of the PDDM model, with each domain coded as a categorical variable comprising three levels:
- O: absence of domain-related issues
- A: moderate presence
- B: strong presence
They used a multiple linear regression model to explore how the categories of each PDDM domain were associated with the percentage change in disability. This allowed them to assess the individual contribution of each domain, while adjusting for the influence of the others.
No additional covariates (such as age or sex) were included, as the PDDM framework is intended to integrate all relevant biopsychosocial factors related to pain and disability.
Secondary and Exploratory Analyses
To complement the primary analysis, they conducted bivariate comparisons to explore the relationship between each PDDM domain and the percentage change in disability. These comparisons aimed to offer a preliminary, unadjusted view of how disability outcomes differed between the three levels (O, A, B) within each domain. Student’s t-tests or Wilcoxon rank-sum tests were used, depending on the distribution of the data.
Researchers conducted supplementary multivariate analyses to examine the prognostic value of multidimensional low back pain phenotyping domains for additional clinically relevant outcomes:
- A multiple linear regression was performed on imputed data to assess whether PDDM domain classifications predicted the percentage change in pain intensity (VAS) over the course of the program.
- A multiple logistic regression was conducted on complete cases to examine whether PDDM classifications were associated with return-to-work status (yes/no) at the final follow-up.
These exploratory analyses were intended to determine whether the PDDM framework could also provide prognostic insight beyond disability outcomes, by evaluating its potential to predict pain reduction and return to work.
Handling of Missing Data
They assumed that missing data were missing at random (MAR) and used statistical imputation to address them.
- Categorical variables were imputed using a proportional odds model.
- Continuous variables were imputed using predictive mean matching.
To test the reliability of their findings, they also performed a sensitivity analysis using complete cases only for the primary analysis. The consistency between the main and sensitivity analyses suggested that the missing data did not significantly affect the results.
Model Specifications
In all multivariate regression models, they selected category A of the nociceptive domain as the reference group, rather than the usual category O. This choice was based on the fact that all patients included in the program had low back pain—making category A the most clinically representative group. However, a few patients who fell into category O (i.e., without nociceptive input) were also included in the analysis.
For the remaining PDDM domains, they used category O as the reference level, representing the absence of relevant features in each domain.
Nosi poruke kući
Prognostic Insights from PDDM Classification:
- Maladaptive behaviors(Cognitive-Emotional Domain B) predict poorer long-term disability outcomes.
- Baseline disability levels vary by subtype:
- Absence of nociceptive pain was associated with lower baseline disability.
- Nervous system dysfunction & cognitive-emotional issues were associated with higher baseline disability.
- Comorbidities were not linked to increased baseline disability.
Assessment & Treatment Priorities:
- Screen rigorously: Use validated tools to identify cognitive-emotional drivers (e.g., fear-avoidance, catastrophizing) earlyand monitor them longitudinally.
- Diagnose collaboratively: Align subtypes (e.g., nociceptive vs. neuropathic) with patient-reported symptoms and
- Treat dynamically: Tailor interventions to dominant drivers (e.g., graded exposure for maladaptive behaviors), then reassess to validate subtype classification.
Study Limitations to Address in Practice:
- Reassess psychosocial factors duringtreatment (not just baseline).
- Document treatment protocols systematically to clarify what works for each PDDM subtype.
Want to learn more about the PDDM? Listen to Physiotutors’ podcast discussion with Yannick Tousignant-Laflamme, one of the study’s co-authors.
Referenca
100% besplatan program kućnih vježbi protiv glavobolje
Preuzmite ovaj BESPLATNI program vježbanja kod kuće za svoje pacijente koji pate od glavobolje. Samo ga isprintajte i dajte im da mogu izvoditi ove vježbe kod kuće