
Research
Knee
May 8, 2025
Kinesio taping za patelofemoralnu bol: Učinci utemeljeni na dokazima na ublažavanje boli i funkciju koljena

Uvod
Patellofemoral Pain Syndrome (PFPS) is a common condition among young, active individuals, characterized by retropatellar pain. While its exact etiology remains unclear, known risk factors include an increased Q-angle, gluteal and quadriceps weakness, and imbalances between the medial and lateral femoral muscles. Since PFPS is believed to result from excessive biomechanical stress, activities such as walking, running, squatting, and stair climbing often exacerbate symptoms. Additionally, dynamic movements—particularly those involving knee valgus—can further increase anterior knee stress and worsen pain.
Kinesio Taping (KT) has been proposed as a potential intervention to alleviate PFPS symptoms. Suggested mechanisms include enhanced sensory feedback, improved circulation, and pain modulation via endogenous analgesic pathways. Some evidence also indicates that Kinesio Taping for patellofemoral pain may help rebalance muscle activation between the vastus medialis and lateralis, potentially correcting patellar malalignment and reducing joint stress.
This study systematically evaluates the efficacy of KT in improving function and reducing pain in individuals with PFPS, providing evidence-based insights for clinical practice.
Metode
This review analyzed RCTs investigating Kinesio Taping for patellofemoral pain patients versus control treatments (no taping, placebo, or standard rehab). Required outcomes included at least one of the following : Visual Analog Scale (VAS), Kujala Anterior Knee Pain scale (AKPS), knee extension peak torque, knee flexion peak torque, knee flexion ROM and knee position perception error. Studies with missing data, conference abstracts, duplicates, methodological flaws, or unavailable full texts were excluded.
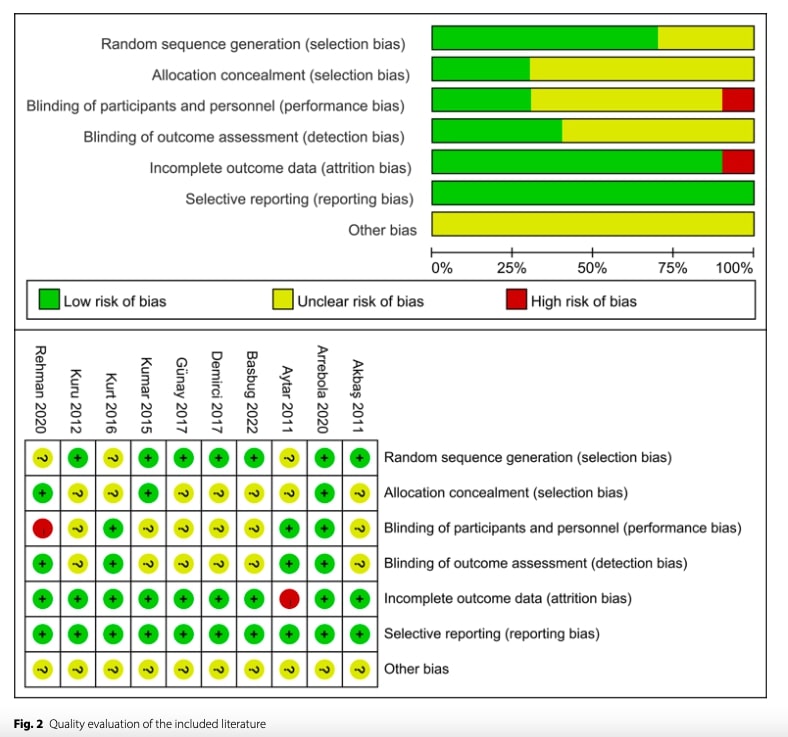
Study quality was evaluated using the Cochrane Risk of Bias tool, assessing seven domains: (1) random sequence generation, (2) allocation concealment, (3) staff blinding, (4) outcome assessor blinding, (5) incomplete outcome data, (6) selective reporting, and (7) other biases. Two independent reviewers rated each domain as low, unclear, or high risk of bias, achieving excellent agreement, the Kappa score of the two reviewers was 0.88 showing a good consistency. Discrepancies were resolved through discussion with a third reviewer.
Data were analyzed using Review Manager 5.3 (α=0.05). Continuous outcomes were pooled using mean difference (MD) or standardized mean difference (SMD) with 95% CIs, depending on measurement consistency. Heterogeneity was assessed via Chi-square tests and I² statistics: fixed-effects models were applied when p≥0.1 and I²<50%, while random-effects models were used for significant heterogeneity (p<0.1 and I²≥50%). Sensitivity analyses evaluated result robustness, and publication bias was assessed via funnel plots when ≥10 studies were available.
Rezultati
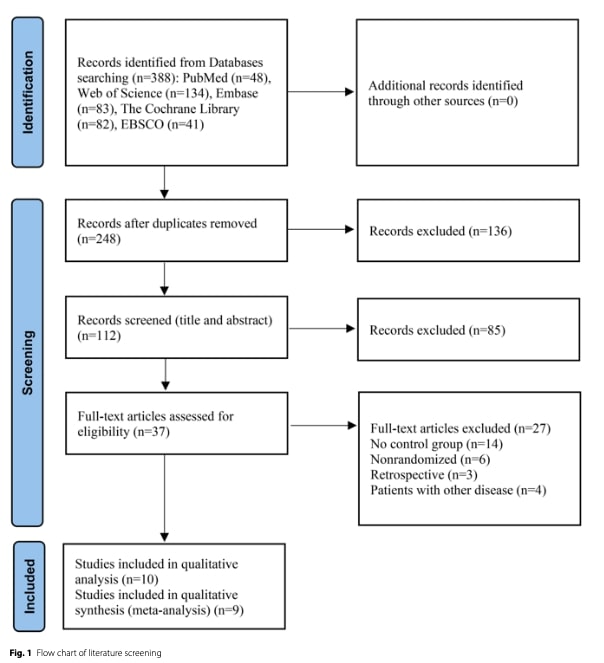
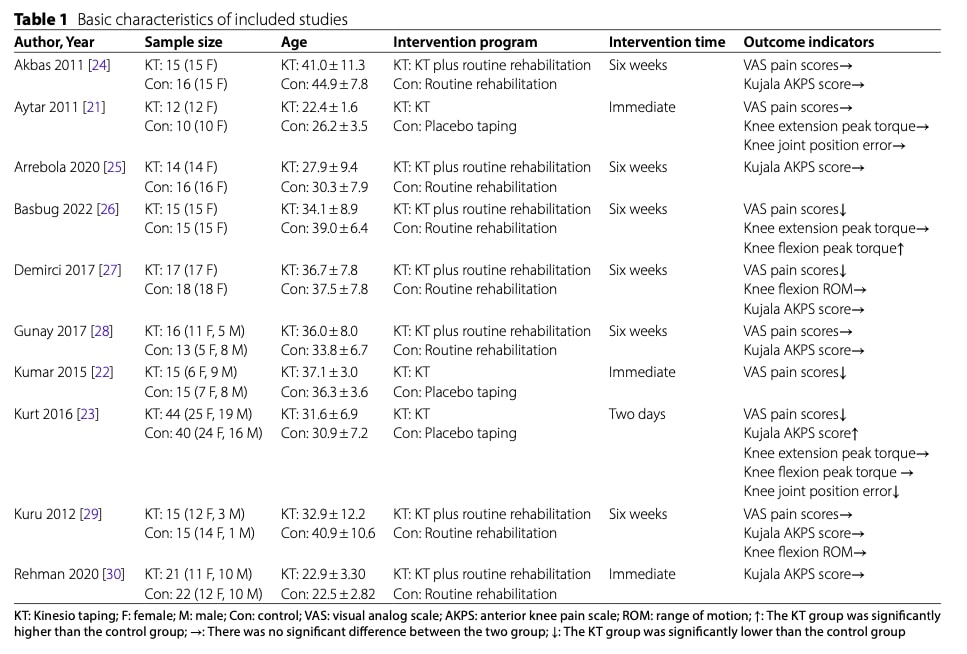
The systematic review included 10 randomized controlled trials comprising 364 patients with patellofemoral pain syndrome (PFPS). Participants were distributed between intervention (n=184) and control (n=180) groups. Three studies evaluated Kinesio Taping for patellofemoral pain (KT) versus placebo taping, while seven examined KT combined with routine rehabilitation compared to rehabilitation alone.
Regarding quality of the studies included, it was relatively low. Concerns are emerging from randomization and blinding process while one study did not provides reasons for patients dropout.
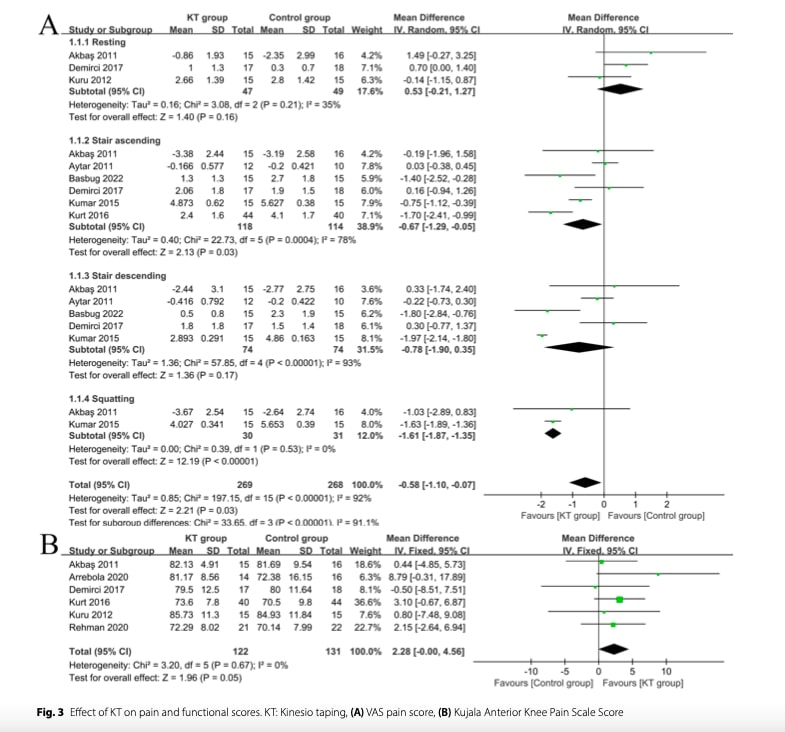
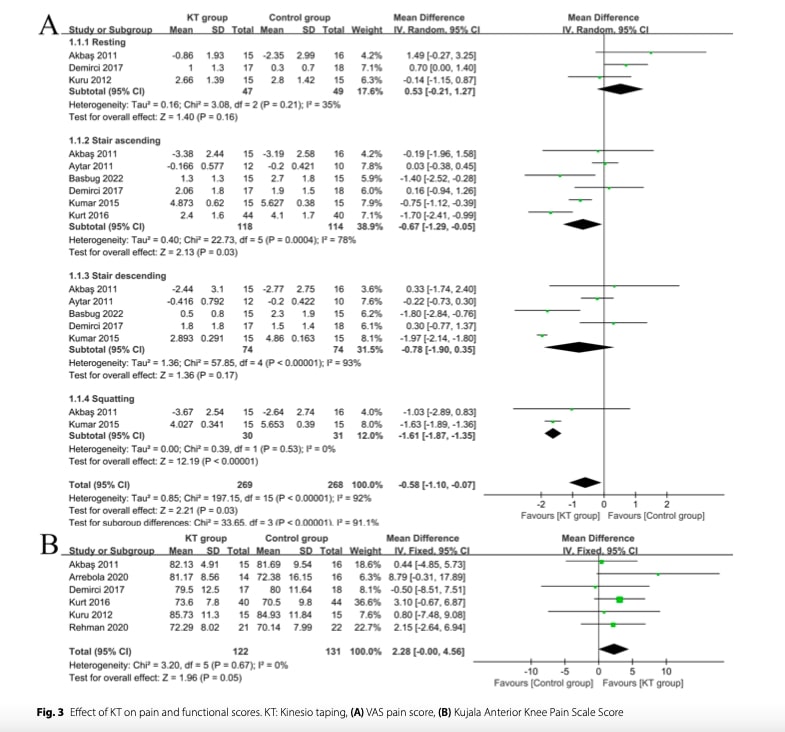
Random-effects meta-analysis of seven studies demonstrated that Kinesio Taping for patellofemoral pain (KT) significantly reduced VAS pain scores compared to control interventions, with particularly notable effects during stair ascent and squatting activities. The substantial heterogeneity suggests important variations across studies in patient characteristics, KT application protocols, or outcome measurement methods. No significant pain reduction was observed during rest or stair descent.
Six studies assessing Kujala Anterior Knee Pain Scale (AKPS) scores demonstrated statistically significant improvements with kinesio taping (KT) versus controls. The moderate heterogeneity (I²=67%, p=0.10) suggests some variability in treatment effects across studies. These findings suggest KT may offer measurable functional benefits for PFPS patients.
Six studies evaluating the Kujala Anterior Knee Pain Scale (AKPS) found that Kinesio Taping for patellofemoral pain provided modest but statistically significant improvements in functional scores compared to control groups. The analysis used a fixed-effects model due to acceptable heterogeneity levels across studies, suggesting relatively consistent treatment effects. While the magnitude of improvement was small, the results indicate that KT may contribute to measurable functional gains in patients with PFPS.
Three studies assessing knee extension peak torque found no significant improvement with kinesio taping (KT) compared to control interventions. Due to substantial heterogeneity across studies, a random-effects model was employed. Subgroup analyses based on isokinetic testing speeds (60°/s and 180°/s) similarly revealed no significant differences in strength outcomes between groups. These results suggest that KT may not enhance quadriceps strength in patients with PFPS, regardless of movement velocity.
The pooled analysis of two studies revealed no significant improvement in knee flexion peak torque with KT compared to controls, with high heterogeneity noted between studies. Subgroup analyses at different isokinetic speeds (60°/s and 180°/s) similarly demonstrated no between-group differences. These findings suggest that KT does not appear to enhance hamstring strength in individuals with PFPS, regardless of movement velocity.
Two studies assessing knee flexion range of motion (ROM) found no significant effect of Kinesio Taping compared to control interventions. The analysis demonstrated consistent results across studies (no observed heterogeneity) and revealed no clinically meaningful differences between groups. These results indicate that KT does not appear to influence passive or active knee flexion mobility in patients with PFPS.
Two studies examining knee joint position sense found no significant improvement with Kinesio Taping compared to control conditions. The consistent results across studies (with minimal heterogeneity) suggest that KT does not appear to enhance proprioceptive accuracy in patients with PFPS. These findings indicate that any potential benefits of KT in PFPS management are unlikely to be mediated through proprioceptive mechanisms.
Pitanja i razmišljanja
First, let’s dive into this study’s limitations. Figure 2 (reporting the quality assessment of included studies) reveals that most research on kinesio taping for patellofemoral pain syndrome (PFPS) suffers from unclear to high risk of three critical biases: selection bias, performance bias, and detection bias. Let’s break down why this matters.
Selection Bias (Randomization & Allocation Issues)
If studies didn’t randomize properly or conceal group assignments, healthier patients might have been assigned to kinesio taping groups—making the tape appear more effective than it truly is for PFPS.
Performance Bias (Lack of Blinding)
Patients who know they’re using kinesio tape—rather than no tape or a sham procedure—might report exaggerated pain relief (placebo effect) or dismiss benefits (nocebo effect), skewing the results.
Detection Bias (Outcome Assessment Flaws)
If researchers knew who received the tape, they might unconsciously rate outcomes more favorably inflating perceived effectiveness.
These biases could mean the actual benefits of kinesio taping for PFPS are weaker than the literature suggests. High-quality reviews flag these issues to help clinicians interpret findings cautiously.
This systematic review revealed considerable heterogeneity (I²=92%, p<0.001) across studies, indicating that KT’s effectiveness for patellofemoral pain likely depends on patient-specific factors (e.g., symptom severity, biomechanics) and technical variations (e.g., taping method, rehabilitation synergy). The extreme variability in VAS outcomes underscores the need for standardized protocols and subgroup analyses to identify optimal candidates for KT.
Studies comparing KT to placebo taping demonstrated superior outcomes, suggesting its effects extend beyond psychological or contextual factors—though these may play a partial role. These observations challenge the proposed mechanisms of Kinesio Taping. While the original rationale emphasized mechanical correction, evidence suggests KT loses tension shortly after application, reducing its capacity for sustained structural alignment. Alternative hypotheses propose that KT enhances proprioception and muscle activation; however, this review found no significant improvements in either strength or joint position sense in PFPS patients. Notably, unlike chronic ankle instability populations (where KT improves proprioception), PFPS patients typically do not present with proprioceptive deficits. Thus, pain reduction in PFPS is unlikely to stem from improved patellar tracking via muscle activation. Instead, the Gate Control Theory may explain KT’s effects, where tactile stimulation from the tape modulates pain perception via sensory afferents. However, if this were the sole mechanism, application techniques would not influence outcomes—yet clinical variability suggests technique matters.
Pričaj štreberski sa mnom
The research team performed all analyses using Review Manager 5.3, establishing statistical significance at *p* < 0.05. Continuous outcome measures (e.g., pain scales, strength assessments) were analyzed using mean differences (MD) for consistent measurement methods or standardized mean differences (SMD) for variable units, both reported with 95% confidence intervals.
To evaluate whether variation between studies exceeded chance expectations, the investigators assessed heterogeneity using two complementary methods:
- Chi-square test:Determines whether observed differences in effect sizes between studies are statistically significant (*p* < 0.10 suggests real heterogeneity exists). In this study, the Chi-square test for VAS pain scores yielded *p* < 0.001, indicating that the variation in pain reduction across studies was extremely unlikely to be due to chance alone. This implies that clinical or methodological differences (e.g., patient populations, KT application techniques) likely contributed to the divergent results.
- I² statistic:Quantifies the percentage of total variation attributable to true clinical/methodological differences (vs. random error). An I² > 50% indicates substantial heterogeneity. For VAS outcomes, the I² of 92% demonstrates that nearly all observed variability stemmed from real differences in study characteristics, such as patient demographics (e.g., activity levels), KT protocols (e.g., tape tension, duration), or assessment methods.
Based on these metrics, the team selected the appropriate analysis model:
- Fixed-effects model (used when I² < 50% AND *p* ≥ 0.1): Assumes all studies estimate a single true effect size, giving more weight to larger studies. This was applied to homogeneous outcomes like knee flexion ROM (I²=0%).
- Random-effects model (used when I² ≥ 50% OR *p* < 0.1): Accounts for between-study variability by assuming different true effects exist. This conservative approach was necessary for highly heterogeneous outcomes like VAS pain scores (I²=92%).
The team further conducted sensitivity analyses to identify influential studies and used funnel plots to detect publication bias—particularly important for avoiding overestimation of treatment effects when negative results are unpublished.
Sensitivity Analysis
The stability of the results was confirmed through sensitivity analyses—systematically excluding individual studies and recalculating the pooled effect sizes did not significantly alter them. This robustness persists despite high heterogeneity (e.g., I²=92%), indicating findings aren’t driven by outliers but reflect true variability in KT’s effects across studies.
Publication Bias
Funnel plot asymmetry for VAS scores suggests unpublished null studies may exist, potentially inflating KT’s apparent pain benefits. While results are statistically stable, clinicians should interpret pain reduction magnitudes cautiously due to this bias.
Nosi poruke kući
Despite methodological limitations in the literature, Kinesio Taping for patellofemoral pain demonstrates potential benefits.
Evidence Summary:
- Pain Reduction: KT may provide modest short-term pain relief during functional activities (e.g., squatting),
- Function: Small improvements in AKPS scores (~2 points) were observed, though clinical relevance is unclear.
- Strength/Proprioception: No significant effects on quadriceps/hamstring strength or joint position sense.
Key Clinical Implications:
- Adjunct, Not Standalone: Use KT as a temporary pain-modulating tool alongside exercise therapy (the cornerstone of PFPS treatment).
- Test-Retest Approach: Apply KT and immediately reassess functional tasks (e.g., squatting, stairs) to identify responders.
- Technique Matters: Outcomes vary with application method (e.g., tension, direction). Tailor to patient symptoms (e.g., patellar maltracking vs. general pain).
These two Physiotutors videos will provide you with evidence-based taping techniques for optimal clinical application. Video 1, video 2.
When to Use/Caution:
- Best for: Acute flare-ups or to facilitate exercise tolerance in pain-dominated PFPS.
- Avoid Overreliance: Discontinue if no immediate benefit is observed. Prioritize strengthening (esp. gluteals/quads) and movement retraining.
Check this Physiotutors article on Patellofemoral Pain Syndrome to guide you in the diagnosis process and management strategies.
Referenca
ULOGA VMO-a & QUAD-ova U PFP-u
Pogledajte ovo BESPLATNO VIDEO PREDAVANJE U 2 DIJELA stručnjakinje za bolove u koljenima Claire Robertson koja secira literaturu o toj temi i kako ona utječe na kliničku praksu .
