
666 recenzije
Research
Diagnosis & Imaging
November 3, 2025
Validnost testiranja usmjerenih preferencija za diskogenu bol u donjem dijelu leđa, novi uvidi iz prospektivne studije dijagnostičke točnosti.

Uvod
Despite advances in research and clinical guidelines, low back pain (LBP) remains the leading cause of disability worldwide. Its persistence reflects the limitations of current diagnostic and therapeutic models, as LBP involves complex interactions between biological, psychological, and social factors.
Traditional patho-anatomical diagnosis is often ineffective because MRI abnormalities frequently appear in asymptomatic individuals, making it difficult to link structural findings to pain. However, older injection-based diagnostic studies suggest that identifying specific pain sources—such as the intervertebral disc—is possible.
Discogenic pain, caused by a damaged or dysfunctional intervertebral disc, is now a well-supported concept, with mechanisms including internal disc disruption and nerve ingrowth. It typically presents as non-radicular, load-sensitive pain. Although provocative discography is the diagnostic gold standard, its invasiveness limits its use, creating a need for reliable non-invasive clinical indicators.
One such indicator is the Centralization Phenomenon (CP)—pain moving proximally or disappearing during repeated movements as described by this Physiotutors article . CP shows good diagnostic value for discogenic pain but only captures part of its spectrum, as not every patient will present CP, but can still greatly improve with repeated movement. A related concept, Directional Preference (DP), refers to specific movements that provide consistent symptom improvement, even without centralization. Directional preference testing is clinically important but lacks studies validating its diagnostic accuracy.
This study therefore aims to:
- Assess the validity of directional preference testing using discography as the reference standard and compare it with CP.
- Develop a clinical diagnostic rule (CDR) for patients without directional preference.
- Develop a CDR for cases where repeated movement testing is not possible.
Methods
This study is a secondary analysis of a prospective, double-blind diagnostic accuracy study (Laslett et al., 2005b) that followed STARD reporting guidelines.
Participants:
Patients with chronic low back pain who underwent both provocative discography (the diagnostic gold standard for discogenic pain diagnosis) and a McKenzie Mechanical Diagnosis and Treatment (MDT) physiotherapy Assessment at a spine care center in New Orleans (2001–2002) were included. Both assessments had to occur within three months of each other to minimize clinical changes in between evaluations. Participants had to speak English, provide consent, and maintain examiner blinding. Two physiotherapists—one senior McKenzie faculty and one certified clinician—conducted respectively 93% and 7% of all evaluations. For this reanalysis, original patient files were transferred to France, double-entered into a new database, and validated by a third researcher.
Index Test (Directional Preference – DP):
Directional preference was the index test, defined as a rapid, lasting, reversible, reproducible, and observable improvement in pain during repeated movement testing in one direction. Improvement was recorded using pain drawings and 0–100 analog scales.
- Rapid: changes observed within one session.
- Lasting: maintained until the end of the session.
- Reversible: opposite movement direction worsens symptoms.
- Reproducible: the pattern is observed at least twice.
Participants were classified as DP+ if they met the core criteria (rapid, lasting, and improved pain). A secondary, stricter analysis included only those meeting all five criteria. Participants who were unable to complete the testing were excluded.
Criterion Standard (Discography):
Discography was considered positive (Disco+) if:
- Injection into a suspect disc reproduced concordant pain, and
- An adjacent control disc produced no pain. This ensured specificity and minimized false positives (<6%).
Blinding and Data Handling:
Physiotherapists were blinded to all imaging, prior injections, and questionnaire data (RMDQ, MZDI, MSPQ). Discography and clinical assessments were performed independently. All patient data were stored securely and later re-entered for the secondary analysis.
Analiza
The researchers first described the study population (DP+/DP−, disco+/disco−, complete/incomplete exams) using means and standard deviations for quantitative data and percentages for categorical data.
For the primary objective, they calculated the sensitivity, specificity, and likelihood ratios (LR+ and LR−) of Directional Preference testing for detecting discogenic pain confirmed by discography.
For the secondary objectives, they developed Clinical Diagnostic Rules (CDRs) following established guidelines. The Best Subset Selection (BeSS) method identified the best predictive model based on the lowest Bayesian Information Criterion (BIC). Model performance and optimal diagnostic thresholds were assessed with ROC curves, Area Under the Curve (AUC), and Youden’s index.
Missing data in pre-visit questionnaires were replaced using mean imputation, while cases with missing clinical exam results were excluded. Statistical significance was set at p < 0.05.
Results
Participants
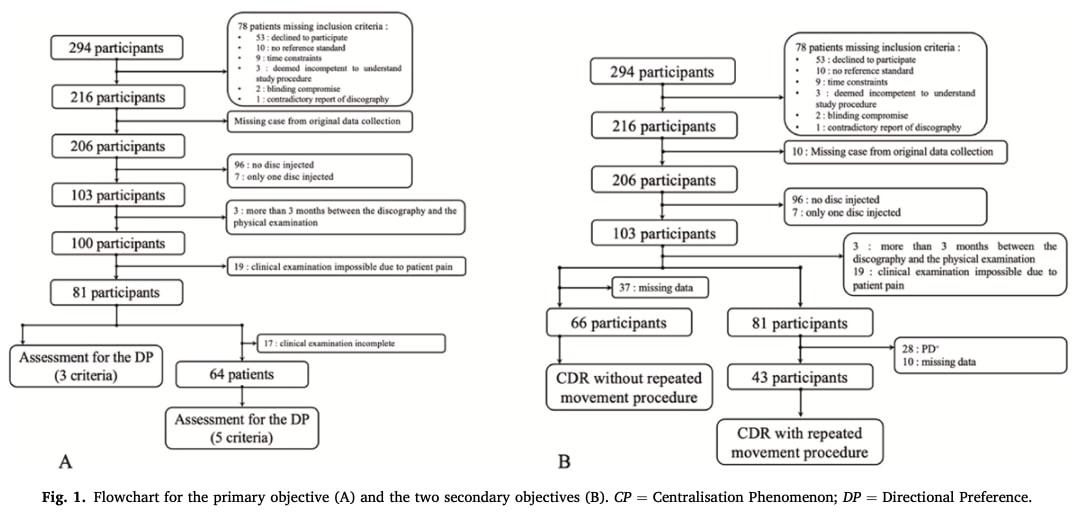
Out of 294 clinic visitors, 216 consented to participate. After exclusions (missing data, excessive delay between tests, and inability to perform movement testing), 81 participants completed at least part of the clinical exam, and 64 completed it fully.
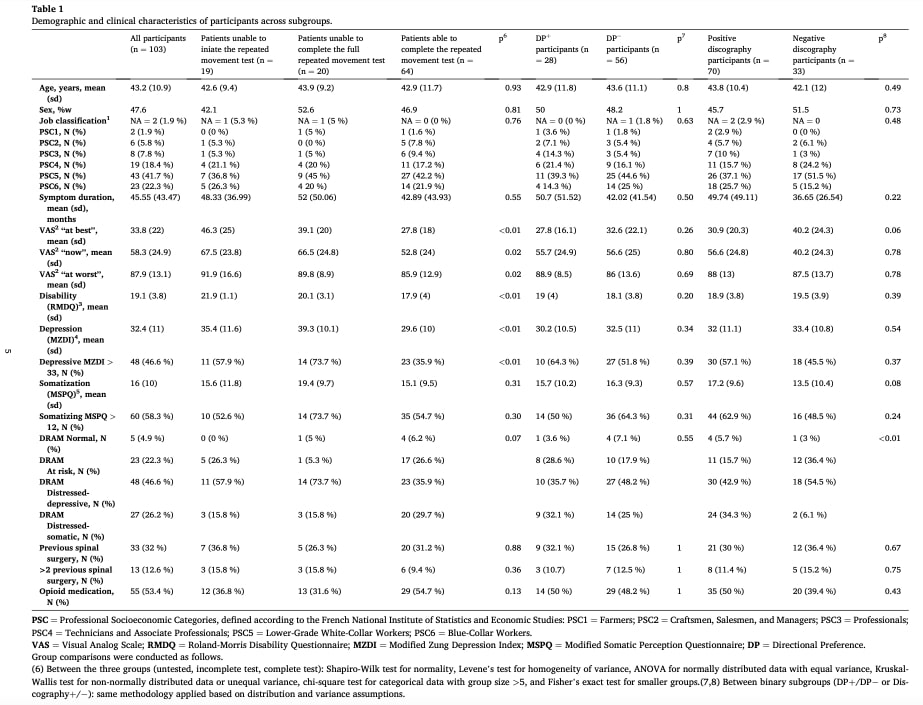
The sample reflected a typical tertiary care population with chronic, severe low back pain lasting on average over 45 months. Mean pain scores ranged from 33.8/100 (best) to 87.9/100 (worst). Participants showed high disability (RMDQ = 19.1), moderate depression (MZDI = 32.4; 48% depressed), and notable somatization (MSPQ = 15.9; 57%). Over half (53%) used opioids, and 32% had prior spinal surgery (12.6% multiple). Most belonged to lower socioeconomic groups (over 70% blue-collar or lower-grade white-collar).
There were no demographic differences between diagnostic subgroups (DP+/DP−, disco+/disco−). However, participants who completed the full clinical exam reported significantly lower pain, disability, and depression than those who only partially completed it, though somatization, opioid use, and surgery history did not differ.
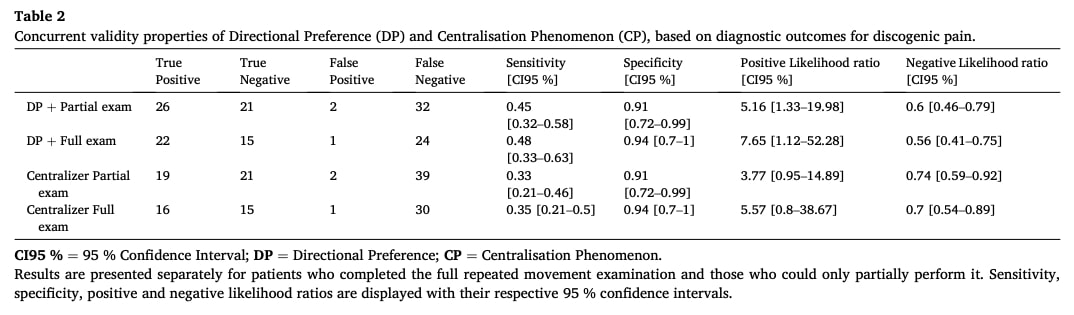
Primary Objective:Directional preference testing showed moderate sensitivity and high specificity for identifying discogenic pain confirmed by discography.
- For participants meeting ≥3 of 5 DP criteria:
- Sensitivity: 0.45
- Specificity: 0.91
- LR+: 5.16
- LR−: 0.60
- For participants completing the full 5-criterion examination:
- Sensitivity: 0.48
- Specificity: 0.94
- LR+: 7.65
- LR−: 0.56
For comparison, the Centralisation Phenomenon demonstrated slightly lower sensitivity (0.33–0.35) but similar specificity (0.91–0.94).
Secondary objectives:
The first secondary objective—developing a Clinical Diagnostic Rule (CDR) for patients who did not exhibit a directional preference—could not be achieved because the dataset included too few DP− participants with complete data across the required explanatory variables. In addition, several variables lacked sufficient observations per category, preventing statistical modelling.
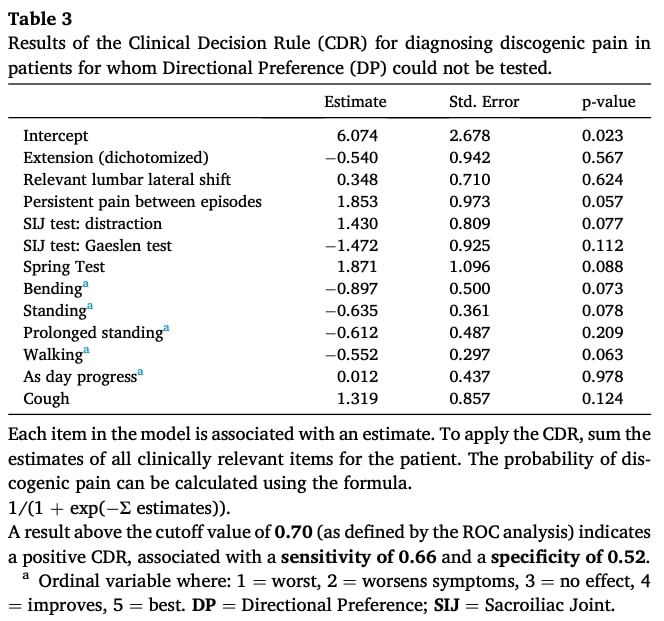
The second secondary objective aimed to establish a CDR for situations in which repeated movement testing could not be performed. This analysis included 55 complete cases (53.4% of the sample). The resulting model integrated several clinical features, including limited extension range of motion, presence of a lateral shift, recurrent pain patterns with persistent pain between episodes, a positive distraction test, negative Gaenslen’s test, positive spring test, improvement of symptoms with bending, standing, or walking, worsening of symptoms as the day progressed, and pain provoked by coughing. Each variable contributed to the total score, with a cutoff of 0.70 selected to optimize sensitivity and specificity. However, the model’s diagnostic performance was weak, with an area under the ROC curve of 0.57, sensitivity of 0.66, specificity of 0.52, LR+ of 1.38, and LR− of 0.66. No individual parameter reached statistical significance.
Pitanja i razmišljanja
Physiotherapy management of low back pain has evolved markedly over the past two decades. Using data from 2001–2002 may therefore limit the study’s relevance. The study’s methodology is further limited by a three-month delay between the directional preference testing and the discography, with no information provided on the specific timing of the assessments. A systematic review suggests that spontaneous regression of lumbar disc herniation can be observed within two to three months, which raises questions about the temporal stability of the discogenic pain source. If the discography was performed three months after the initial clinical assessment, it becomes difficult to ensure that the pain captured at both time points originated from the same structural lesion. During this interval, changes such as partial resorption of the herniation, altered muscle tone, maladaptive motor behaviours, or cognitive-affective drivers of pain could have influenced the patient’s symptom profile and pain perception.
Moreover, the mean pain duration of 43.5 months observed in this study challenges the notion that persistent pain necessarily reflects ongoing structural pathology. Chronic pain—commonly defined as pain lasting more than three months—may instead be partly driven by central sensitization and neuroplastic changes. This raises doubts about the ability of discography, which focuses on structural nociception, to reliably identify the primary pain generator in a population with long-standing symptoms. The prolonged duration of pain may also help explain why relatively few directional preference patients were identified in this study. Investigating low back pain in a more acute patient, where nociceptive factors are more likely to explain patient pain, could therefore provide valuable additional insights.
At the structural level, MRI may help identify discogenic pain with Modic Type 1 changes associated with discogenic pain, showing a high positive likelihood ratio despite only a moderate negative likelihood ratio. Interestingly, as mentioned by the authors in the discussion, individuals with Modic Type 1 changes typically do not respond to repeated movement testing and are therefore rarely classified as having a directional preference. This suggests that discogenic pain associated with Modic Type 1 changes and discogenic pain in directional preference patients may represent two distinct clinical phenotypes.
Talk nerdy to me
To appreciate these study results, let’s first discuss what sensitivity and specificity are. Both are expressed as percentages, and the closer they are to 100%, the better the test performs. Sensitivity refers to the ability of a test to correctly identify patients who truly have the condition. A highly sensitive test rarely misses affected individuals, meaning it produces very few false negatives.
On the other hand, specificity reflects the ability of a test to correctly identify people who do not have the condition. A test with high specificity produces very few false positives, meaning it rarely labels a healthy person as being affected.
Likelihood ratios (LRs) take sensitivity and specificity one step further and help us understand what a test result actually means for an individual patient. A positive likelihood ratio (LR+) tells us how much more likely a person with the condition is to have a positive test compared to someone without the condition, while a negative likelihood ratio (LR−) tells us how much less likely a person with a negative test result has the condition. In simple terms, LR+ helps rule in a diagnosis (a good LR+ is generally above 5, ideally above 10), and LR− helps rule out a diagnosis (a good LR− is generally below 0.3, ideally below 0.1). Unlike sensitivity and specificity, which describe test performance in general, likelihood ratios allow clinicians to combine a patient’s pre-test probability (how likely the condition is before testing) with the test result to estimate a post-test probability, giving a clearer picture of the patient’s actual risk.
For this study, patients showing three or more signs of directional preference are likely to have discogenic pain because the test has high specificity (0.91). However, the sensitivity is low (0.45), meaning that many patients who actually have discogenic pain may not be identified by the test. The LR+ of 5.16 indicates that a positive test result substantially increases the probability that a patient truly has discogenic pain, making the test useful for ruling in the diagnosis. Conversely, the test is not very effective at ruling out discogenic pain when the result is negative (LR− = 0.60). For patients showing all five signs of directional preference, the sensitivity remains relatively low (0.48), meaning that many patients who actually have discogenic pain may not be detected by the test. However, the specificity is very high (0.94), indicating that patients who test positive are very likely to truly have discogenic pain, with very few false positives. The LR+ of 7.65 shows that a positive test is useful for ruling in the diagnosis, while the LR− of 0.56 indicates that a negative test result is not very effective for ruling out discogenic pain. Consequently, directional preference testing appears to have limited utility as a screening tool in this patient population.
To address their secondary objectives, the researchers aimed to identify the best combination of clinical signs and symptoms that could accurately predict discogenic pain, effectively developing a clinical decision rule (CDR). Using the Best Subset Selection (BeSS) method, they systematically tested various combinations of clinical findings — such as limitation of lumbar extension, presence of a lateral shift, persistent or recurrent pain, and several provocation tests — to determine which combination offered the best predictive accuracy. The Bayesian Information Criterion (BIC) was then applied to select the most efficient model.
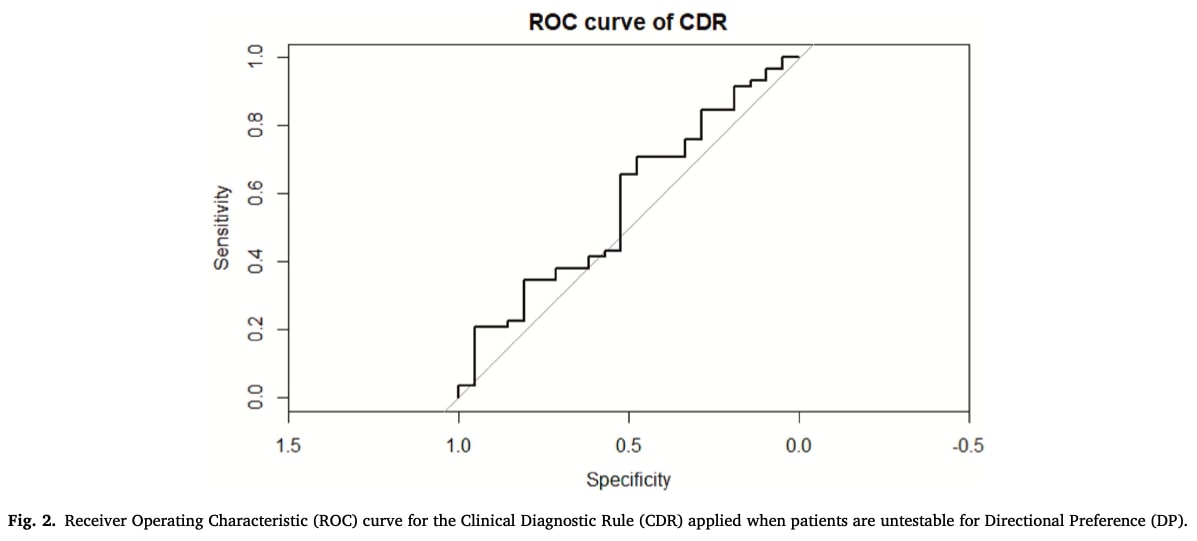
After selecting the optimal subset of predictors, the researchers evaluated the model’s diagnostic performance. They used a Receiver Operating Characteristic (ROC) curve to examine the trade-off between sensitivity and specificity, calculating an Area Under the Curve (AUC) of 0.57, which indicates poor discriminative ability. The optimal diagnostic threshold, identified through Youden’s index, yielded a sensitivity of 0.66 and a specificity of 0.52, with corresponding positive and negative likelihood ratios (LR+ = 1.38; LR- = 0.66). Together, these results demonstrate that the proposed CDR had limited diagnostic value and was unable to reliably distinguish between discogenic and non-discogenic pain for patients who are not able to undergo the directional preference testing. Further RCTs should be conducted before any adoption in clinical practice.
Take-home messages
- High specificity, low sensitivity: Directional preference testing has high specificity (0.91–0.94) but low sensitivity (0.45–0.48) for detecting discogenic low back pain. This means a positive DP test strongly suggests true discogenic pain, but a negative test does not rule it out.
- Useful for ruling in, not for screening: The positive likelihood ratio (LR+ 5.16–7.65) indicates directional preference testing is valuable to confirm discogenic pain in patients, but its limited ability to detect all cases makes it unsuitable as a general screening tool.
- Chronicity matters: In populations with long-standing low back pain (mean duration >3.5 years), it is likely that directional preference testing may identify fewer positive cases due to the broader implications of various pain drivers.
- Acute vs chronic patients: directional preference testing may be more informative in patients with more acute low back pain, where nociceptive factors are more likely to drive symptoms.
- Distinct phenotypes: Discogenic pain associated with Modic Type 1 changes may not respond to repeated movement testing and rarely shows a directional preference, suggesting different clinical phenotypes that physiotherapists should consider.
- Complementary assessment: Directional preference testing should be used alongside other clinical findings, patient history, and, when appropriate, imaging to guide individualized management rather than as a standalone diagnostic tool.
Here’s a helpful Physiotutors guide to support your LBP assessments.
Reference
Kako prehrana može biti presudan čimbenik za centralnu senzibilizaciju - video predavanje
Pogledajte ovo BESPLATNO video predavanje o prehrani i središnjoj senzibilizaciji od strane europskog broj 1 istraživača kronične boli Joa Nijsa. Koju hranu bi pacijenti trebali izbjegavati vjerojatno će vas iznenaditi!
